Open Reduction and Internal Fixation of Scaphoid Fractures
DEFINITION
The scaphoid is the most commonly fractured carpal bone, accounting for 1 in every 100,000 emergency department visits.15Scaphoid fractures typically result from a fall on an outstretched hand or less commonly following forced palmar flexion of the wrist20 or axial loading of the flexed wrist such as in punching.12Scaphoid nonunion or proximal pole avascular necrosis (AVN) after a fracture has been associated with considerable morbidity and a predictable pattern of wrist arthritis.18,21,25The complex anatomy and tenuous blood supply to the scaphoid make operative management of these fractures technically challenging.25
ANATOMY
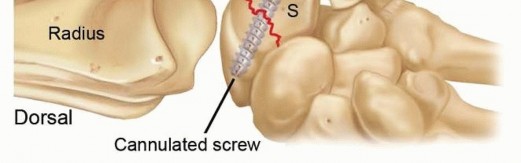
The scaphoid has a complex three-dimensional geometry that has been likened to a “twisted peanut.” It can be divided into three regions: proximal pole, waist, and distal pole.The scaphoid functions as the primary link between the forearm and the distal carpal row and therefore plays a critical role in maintaining normal carpal kinematics.Articulating with the scaphoid fossa of the radius, the lunate, capitate, trapezium, and trapezoid, more than 70% of the scaphoid is covered with articular cartilage.Gelberman and Menon8 have described the vascular supply of the scaphoid. The main arterial supply is from the radial artery; it enters the scaphoid via two main branches:A dorsal branch, entering through the dorsal ridge, is the primary supply and provides 70% to 80% of the vascularity, including the entire proximal pole via retrograde endosteal branches.A volar branch, entering through the tubercle, supplies the remaining 20% to 30%, predominantly the distal pole and tuberosity.The proximal pole is at increased risk for AVN secondary to disruption of its tenuous retrograde blood supply after a fracture of the scaphoid waist or proximal pole.Due to its tenuous vascular supply, the scaphoid heals almost entirely by primary bone healing, resulting in minimal callus formation.The size and shape of the scaphoid, in combination with its precarious blood supply, demands attention to detail and accurate implantation of fixation devices during fracture fixation. Scaphoid dimensions vary between genders; the male scaphoid is usually longer and wider than the females. In addition, the diameter of mostcommercially available standard screws are larger than the proximal pole of the female scaphoid.11
PATHOGENESIS
Scaphoid fractures are most commonly seen in young, active males.15With the wrist dorsiflexed greater than 95 degrees, in combination with 10 degrees or more of radial deviation, the distal radius abuts the scaphoid and precipitates a fracture.15The scaphoid can also be fractured with forced palmar flexion of the wrist20 or axial loading of the flexed wrist.12 Most of these fractures occur at the waist region, although 10% to 20% occur in the proximal pole.Proximal pole fractures are associated with an increased risk of nonunion, delayed union, and AVN. In children, scaphoid fractures are less common and are most frequently seen in the distal pole.
NATURAL HISTORY
An untreated or inadequately treated scaphoid fracture has a higher likelihood of nonunion. The overall incidence of nonunion is estimated at 5% to 10%, but the risk is significantly increased with nonoperative treatment of a displaced waist or proximal pole fracture.The natural history of scaphoid nonunions is controversial, but they are believed to result in a predictable pattern of progressive radiocarpal and midcarpal arthritis.8,9,14,17,18,21,25In an established scaphoid nonunion, the distal portion of the scaphoid may flex, producing a “humpback” deformity of the scaphoid. The loss of scaphoid integrity can result in carpal instability and abnormal carpal kinematics, most frequently manifesting as a dorsal intercalated segment instability (DISI) pattern.The pattern of carpal instability and secondary arthrosis due to an unstable scaphoid nonunion has been termed anSNAC wrist(scaphoid nonunion advanced collapse pattern of wrist arthritis).14,21In the SNAC wrist, there is a loss of carpal height with proximal capitate migration, flexion and pronation of the scaphoid, and secondary midcarpal arthritis.21Factors associated with the development of a scaphoid fracture nonunion include the following17:Delayed diagnosis or treatment Inadequate immobilizationProximal fractureInitial and progressive fracture displacement Fracture comminutionPresence of associated carpal injuries (ie, perilunate injury)P.340
PATIENT HISTORY AND PHYSICAL FINDINGS
Scaphoid fractures classically occur in the active, young adult population. Patients present with radial-sided wrist pain.Classic physical examination findings include the following:Swelling over the dorsoradial aspect of the wrist Tenderness to palpation in the “anatomic snuffbox”Tenderness with palpation volarly over the distal tuberclePain with axial compression of the wrist (scaphoid compression test) Scaphoid fractures can be part of a greater arc injury.The physician should examine the entire wrist carefully for areas of tenderness and swelling.Plain radiographs are scrutinized for an associated ligamentous injury or disruption of the midcarpal joint as seen in the transscaphoid perilunate fracture-dislocation.
IMAGING AND OTHER DIAGNOSTIC STUDIES
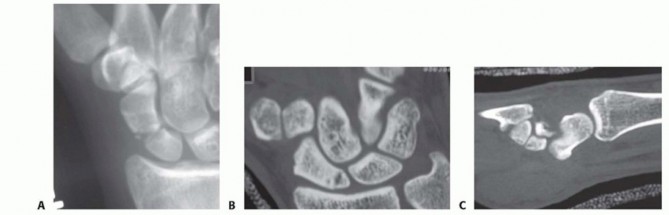
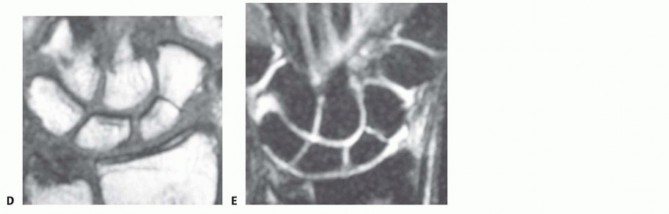
FIG 1 • A. Radiograph (scaphoid view) of an acute, displaced, comminuted scaphoid waist fracture. B,C. Axial and sagittal CT scan images demonstrating a fracture of the proximal pole of the scaphoid. D,E. T1- and T2-weighted MRI images demonstrating a nondisplaced scaphoid waist fracture. (Copyright Peter J.L. Jebson, MD.) The semipronated oblique view provides the best visualization of the waist and distal pole regions. The semisupinated oblique view provides the best visualization of the dorsal ridge.The lateral view permits an assessment of fracture angulation, carpal alignment, and carpal instability.The dedicated scaphoid view is a PA view with the wrist in ulnar deviation. This results in scaphoid extension, allowing visualization of the scaphoid in profile (FIG 1A).The following criteria define a displaced or unstable fracture as noted on plain radiographs2,9,17:At least 1 mm of displacementMore than 10 degrees of angular displacement Fracture comminutionRadiolunate angle of more than 15 degrees Scapholunate angle of more than 60 degrees Intrascaphoid angle of more than 35 degreesComputed tomography (CT) with reconstruction images in multiple planes is used to identify an acute fracture not detected on plain radiographs and to determine the amount of displacement and comminution (FIG 1B,C).CT is most useful in evaluating an established scaphoid nonunion or malunion.6Because plain radiographs are often unreliable, CT is preferred for confirming union after a scaphoid fracture particularly before permitting a return to contact sports.Magnetic resonance imaging (MRI) may be indicated in the evaluation of a suspected scaphoid fracture not detected on plain radiographs (FIG 1D,E). MRI is highly sensitive, withP.341a specificity approaching 100% when performed within 48 hours of injury.16Bone bruising without a fracture detected on MRI can lead to an occult fracture in 2% of cases.23MRI with intravenous gadolinium contrast is helpful in assessing the vascularity of the proximal pole, particularly in the patient with an established nonunion.A technetium bone scan has been shown to be up to 100% sensitive in identifying an occult fracture.27Unfortunately, it is also associated with a low specificity and often will not be positive immediately after the fracture.
DIFFERENTIAL DIAGNOSIS
Scapholunate injury Wrist sprainWrist contusionFracture of other carpal bone Greater arc injuryDistal radius fracture
NONOPERATIVE MANAGEMENT
Nonoperative management is indicated for a nondisplaced, stable scaphoid waist or distal pole fracture.Unstable fractures and nondisplaced fractures of the proximal pole are indications for internal fixation based on studies that have demonstrated a poor outcome with nonoperative treatment.2,4,17The appropriate type and duration of cast immobilization remain controversial and none has proven to be superior. Our preference is a short-arm thumb spica cast until the clinical examination and radiologic studies (usually a CT scan) confirm fracture union. If there are concerns for patient compliance, we prefer an initialperiod (4 to 6 weeks) of long-arm thumb spica cast immobilization.Clinical studies have failed to demonstrate any benefit from including the thumb or fingers in the cast.2,4 Similarly, wrist position has not been proven to improve scaphoid fracture healing.Numerous studies have revealed no difference in union rates for a long-arm versus short-arm cast; however,a randomized prospective study by Gellman et al10 documented a shorter time to union and fewer nonunions and delayed unions with initial use of a long-arm cast.The morbidity of a nonoperative approach, specifically cast immobilization, has become of increasing concern. A prolonged duration of immobilization is often required for waist fractures, and this can be accompanied by muscle atrophy, stiffness, reduced grip strength, and residual pain. In addition, cast immobilization can cause significant inconvenience for the patient and interference with activities of daily living. The prolonged duration of immobilization is of particular concern in the young laborer, athlete, or military personnel, who typically desireexpedient functional recovery.5,19,29If the clinical history and physical examination are suggestive of a scaphoid fracture but initial radiographs are negative, the wrist should be immobilized for 2 weeks. Repeat radiographs are then obtained. If a fracture is present, resorption at the fracture may be noted. If wrist pain and “snuffbox” tenderness persist but radiographsare negative, an MRI or CT scan may be obtained.16,27Alternatively, if there is a high index of suspicion at initial presentation with “normal” radiographs or if there is a need to know the status of the scaphoid, such as in the elite athlete, we prefer MRI.
SURGICAL MANAGEMENT
Indications for open reduction and internal fixation (ORIF) of scaphoid fractures include the following2,17:Proximal pole fractureA displaced, unstable fracture of the scaphoid waist Associated carpal instability or perilunate instability Associated distal radius fractureDelayed presentation (more than 3 to 4 weeks) with no prior treatmentA nondisplaced, stable scaphoid waist fracture in a patient who wishes to avoid the morbidity of cast immobilization. In this clinical scenario, operative treatment should occur only after an explanation of the rationale for, and the risks and benefits of, operative treatment versus cast immobilization.
PREOPERATIVE PLANNING
All imaging studies should be reviewed to accurately define the fracture pattern. Required equipment are as follows:Portable mini-fluoroscopy unit Kirschner wiresCannulated headless compression screw system. We prefer to use the Acutrak 2 or mini-Acutrak 2 screw system (Acumed, Beaverton, OR), but any cannulated screw system that permits screw insertion beneath the articular surface may be used.
POSITIONING
General or regional anesthesia may be used.The patient is positioned supine on the operating table with a radiolucent hand table at the shoulder level. The fluoroscopy unit is draped and positioned at the end of the hand table.A pneumatic tourniquet is carefully applied to the proximal arm.An intravenous antibiotic is provided before inflation of the tourniquet as prophylaxis for infection.The limb is prepared and draped, followed by exsanguination of the limb with an Esmarch bandage and tourniquet inflation, usually to a pressure of 250 mm Hg.
APPROACH
ORIF of scaphoid fractures can be performed through either a dorsal or volar approach. The specific approaches that will be described include the following:Open dorsal approach19 Open volar approachP.342
TECHNIQUES
Open Dorsal Approach (Authors' Preferred Approach)
Open Dorsal Approach (Authors' Preferred Approach)
EXPOSURE


TECH FIG 1 • A. Skin incision used for ORIF of scaphoid fractures via the dorsal approach. B. Retracting the thumb and wrist extensor tendons radially and the finger extensor tendons ulnarly facilitates exposure of the underlying capsule. C. A limited capsulotomy should be performed to expose the proximal scaphoid and scapholunate ligament. (Copyright of Peter J.L. Jebson, MD.)
FRACTURE REDUCTION AND PROVISIONAL FIXATION
Distract the carpus manually via longitudinal traction on the index and long fingers.If the fracture is displaced, insert 0.045-inch Kirschner wire joysticks perpendicularly into the proximal and distal scaphoid fragments to assist in the reduction (TECH FIG 2A).The accuracy of the reduction can be determined by assessing congruency of the radioscaphoid and scaphocapitate articulations.When a satisfactory reduction has been achieved, obtain provisional fixation with parallel derotational 0.045-inch Kirschner wires.The first wire is inserted dorsal and ulnar to the central axis of the scaphoid, into the trapezium for enhanced stability.The second derotational wire may be inserted volar and radial to the anticipated central axis insertion site if more fixation is needed.The derotational wires must be placed such that they will not interfere with central axis guidewire placement, reaming, and screw insertion (TECH FIG 2B).
GUIDEWIRE PLACEMENT

SCREW INSERTION

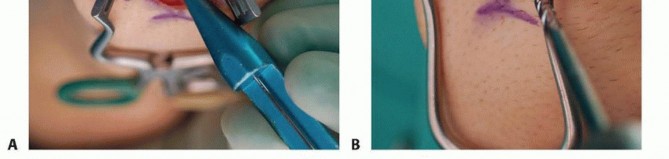

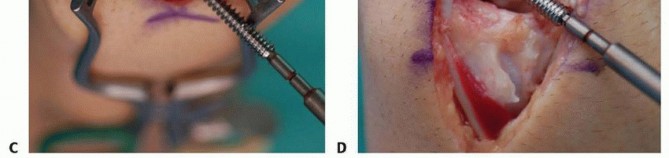
TECH FIG 4 • A. Determining the appropriate screw length. B. Reaming with the cannulated reamer. C,D. Insertion of the screw. A-D: Top is distal, bottom is proximal, left is radial, and right is ulnar. (Copyright Peter J.L. Jebson, MD.)
Open Volar Approach
OPEN VOLAR APPROACH
EXPOSURE
Radially, deviate the wrist and palpate the scaphoid tubercle.Make a 3- to 4-cm incision centered over the scaphoid tubercle, directed distally toward the base of the thumb and proximally over the flexor carpi radialis (FCR) tendon sheath. If the superficial volar branch of the radial artery is encountered, cauterize it at the level of the wrist flexion crease.Open the FCR sheath, and retract the tendon ulnarly. Open the floor of the sheath distally to expose the underlying volar wrist capsule.Distally, develop the interval by splitting the origin of the thenar muscles in line with their fibers over the distal scaphoid and trapezium.Incise the capsule longitudinally, taking care to avoid damage to the underlying articular cartilage.Proximally, divide the thickened radiolunate and radioscaphocapitate ligaments to allow exposure of theproximal scaphoid pole.Identify the scaphotrapezial joint with a Freer elevator and bluntly expose it.Dissection over the radial aspect of the scaphoid is limited to avoid injury to the dorsal ridge vessel.Define and clear the fracture site by irrigation, sharp excision of periosteal flaps, and curetting of debris and hematoma.Assess the instability of the fracture by wrist manipulation.It is critical to identify any bone loss, as compression during screw placement can result in an iatrogenic malunion.
FRACTURE REDUCTION AND FIXATION

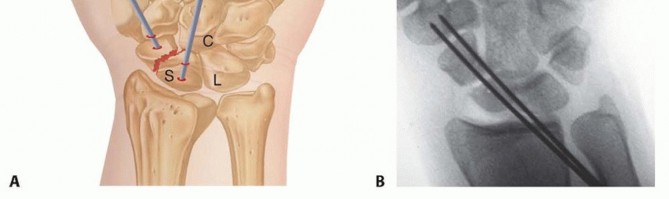
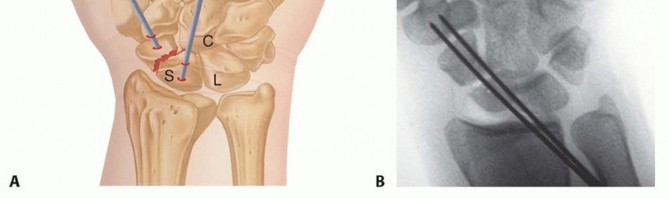
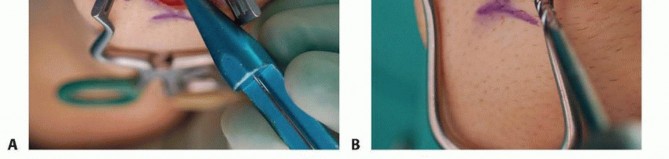
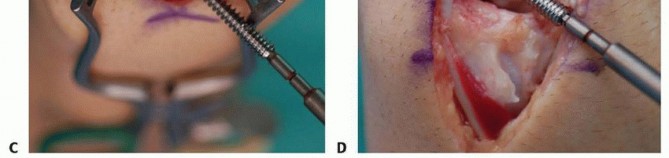
TECH FIG 5 • Accurate insertion of a screw via the volar approach usually requires partial resection or dorsal displacement of the volar trapezium to expose the distal scaphoid. The cannulated compression screw may be inserted using a freehand technique or a commercial device, which simultaneously facilitates fracture reduction and guidewire positioning.Fluoroscopy is invaluable during wire and screw insertion and to confirm accurate placement and fracture reduction as described earlier.Precisely repair the volar wrist capsule and radiolunate and radioscaphocapitate ligaments with permanentsuture.
PEARLS AND PITFALLS
Injury to thescaphoid blood supply1. Meticulous limited dissection of the capsule. Avoid any dissection on the dorsalridge of the scaphoid.Malpositioningof guidewire1. Pronate and flex wrist during the dorsal approach to allow appropriate trajectory.Confirm position on multiple views to ensure insertion in the central axis of the scaphoid.Screw position ▪ Select a screw that is 4 mm shorter than measured length unless fracturefragments are separated; in that case, choose a shorter screw.Reduction ofan unstable fracture1. Perpendicular Kirschner wire joysticks inserted into the proximal and distalscaphoid fragments are useful to obtain a reduction.2. Provisional derotational Kirschner wires placed before screw insertion can be used to stabilize fragments during screw insertion.3. Recognize comminution and bone loss to avoid inadvertent shortening or malreduction with screw compression.Small proximalpole fracture1. Use of a small screw (ie, mini-Acutrak 2) may be necessary to preventcomminution of the proximal fragment.2. Confirm central axis screw position, especially in the proximal pole.
POSTOPERATIVE CARE
The patient is immobilized in a below-elbow volar splint and discharged to home with instructions on strict limb elevation and frequent digital range-of-motion exercises.At 2 weeks, the patient returns for suture removal. Range-of-motion exercises are begun, and a removable forearm-based thumb splint is worn. The splint is discontinued at 6 weeks postoperatively.If the fracture involves the proximal pole or if significant comminution was noted at surgery and there is concern regarding stability of the fixation, immobilization in a short-arm cast for 6 to 10 weeks is indicated. Typically, such fractures take longer to achieve union.After cast removal, a formal supervised therapy program is initiated to achieve satisfactory range of motion, strength, and function.Fracture healing is assessed at 2, 6, and 12 weeks postoperatively with plain radiography. Fracture union is defined as progressive obliteration of the fracture and clear trabeculation across the fracture site (FIG 2).If there is any question regarding fracture union, a CT scan is obtained at 3 months postoperatively or before the patient is allowed to return to unrestricted sporting activities.
OUTCOMES
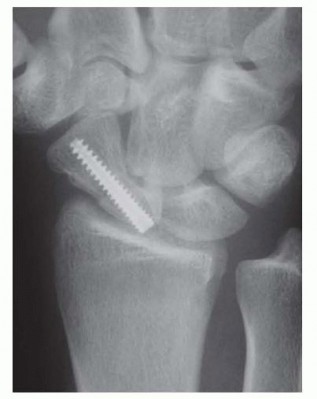
FIG 2 • A healed scaphoid waist fracture after ORIF via the dorsal approach. Although the screw may appear slightly long, both the proximal scaphoid and distal scaphoid are covered with hyaline cartilage not detected on diagnostic imaging. (Copyright Peter J.L. Jebson, MD.) A volar approach has traditionally been used for screw insertion. However, recent studies have raised potential concerns regarding eccentric screw placement and damage to the scaphotrapezial articulationwith this approach.29Our preferred technique for fixation of a scaphoid proximal pole or waist region fracture involves a limiteddorsal approach with compression screw fixation.19 The technique is simple and permits visualization of a reliable starting point for screw placement within the central axis of the scaphoid, offering a significant potential advantage over the volar approach. We recently reported our clinical experience in a consecutiveseries of nondisplaced scaphoid waist fractures.3
COMPLICATIONS
Postoperative wound infections are rare and can be prevented with routine preoperative antibiotic prophylaxis, thorough wound irrigation, and appropriate soft tissue management.Intraoperative technical problemsInadvertent bending or breakage of the guidewire can occur if the wrist is dorsiflexed with the wire in position or during drilling before screw insertion.Care should be taken to confirm that the screw is fully seated beneath the articular cartilage to avoid prominence and erosion of the distal radius articular surface. Similarly, failure to carefully judge accurate screw length intraoperatively can result in prominence within the scaphotrapezial articulation.Nonunion with or without AVN can occur despite compression screw fixation, particularly with a proximal pole or displaced waist fracture. Stripping of the dorsal ridge vasculature should be avoided. Supplemental cancellous bone graft from the distal radius may be used at the time of fixation of a displaced or comminuted fracture if desired.Other potential but rare complications Hypertrophic scarInjury to the dorsal branches of the superficial radial nerveDamage to the scaphotrapezial articulation Proximal pole fragment comminution
REFERENCES
- Adams BD, Blair WF, Reagan DS, et al. Technical factors related to Herbert screw fixation. J Hand Surg Am 1988;13(6):893-899.
- Amadio PC, Moran SL. Fractures of the carpal bones. In: Green D, Hotchkiss R, Pederson WC, eds. Green's Operative Hand Surgery, ed 5. Philadelphia: Churchill Livingstone, 2005:711-740.
- Bedi A, Jebson PJ, Hayden RJ, et al. Internal fixation of acute, nondisplaced scaphoid waist fractures via a limited dorsal approach: an assessment of radiographic and functional outcomes. J Hand Surg Am 2007;32(3):326-333.
- Burge P. Closed cast treatment of scaphoid fractures. Hand Clin 2001;17:541-552.
- Chen AC, Chao EK, Hung SS, et al. Percutaneous screw fixation for unstable scaphoid fractures. J Trauma 2005;59:184-187.
- Dias JJ, Taylor M, Thompson J, et al. Radiographic signs of union of scaphoid fractures. An analysis of inter-observer agreement and reproducibility. J Bone Joint Surg Br 1988;70(2):299-301.
- Dodds SD, Panjabi MM, Slade JF III. Screw fixation of scaphoid fractures: a biomechanical assessment of screw length and screw augmentation. J Hand Surg Am 2006;31(3):405-413.
- Gelberman RH, Menon J. The vascularity of the scaphoid bone. J Hand Surg Am 1980;5(5):508-513.
- Gelberman RH, Wolock BS, Siegel DB. Fractures and non-unions of the carpal scaphoid. J Bone Joint Surg Am 1989;71A:1560-1565.
- Gellman H, Caputo RJ, Carter V, et al. Comparison of short and long thumb-spica casts for non-displaced fractures of the carpal scaphoid. J Bone Joint Surg Am 1989;71(3):354-357.
- Heinzelmann AD, Archer G, Bindra RR. Anthropometry of the human scaphoid. J Hand Surg Am 2007;32(7):1005-1008.
- Horii E, Nakamura R, Watanabe K, et al. Scaphoid fracture as a “puncher's fracture.” J Orthop Trauma 1994;8:107-110.
- Jørgsholm P, Thomsen NO, Björkman A, et al. The incidence of intrinsic and extrinsic ligament injuries in scaphoid waist fractures. J Hand Surg Am 2010;35(3):368-374.
- Kerluke L, McCabe SJ. Nonunion of the scaphoid: a critical analysis of recent natural history studies. J Hand Surg Am 1993;18(1):1-3.
- Kozin SH. Incidence, mechanism, and natural history of scaphoid fractures. Hand Clin 2001;17:515-524.
- Kukla C, Gaebler C, Breitenseher MJ, et al. Occult fractures of the scaphoid. The diagnostic usefulness and indirect economic repercussions of radiography versus magnetic resonance scanning. J Hand Surg Br 1997;22(6):810-813.
- Leslie IJ, Dickson RA. The fractured carpal scaphoid. Natural history and factors influencing outcome. J Bone Joint Surg Br 1981; 63-B(2):225-230.
- Mack GR, Bosse MJ, Gelberman RH, et al. The natural history of scaphoid nonunion. J Bone Joint Surg Am 1984;66(4):504-509.
- Martus J, Bedi A, Jebson PJL. Cannulated variable pitch compression screw fixation of scaphoid fractures using a limited dorsal approach. Tech Hand Up Extrem Surg 2005;9:202-206.
- Ritchie JV, Munter DW. Emergency department evaluation and treatment of wrist injuries. Emerg Med Clin North Am 1999;17: 823-842.
- Ruby LK, Stinson J, Belsky MR. The natural history of scaphoid non-union. A review of fifty-five cases. J Bone Joint Surg Am 1985;67(3):428-432.
- Schädel-Höpfner M, Junge A, Böhringer G. Scapholunate ligament injury occurring with scaphoid fracture—a rare coincidence? J Hand Surg Br 2005;30:137-142.
- Thavarajah D, Syed T, Shah Y, et al. Does scaphoid bone bruising lead to occult fractures? A prospectivestudy of 50 patients. Injury 2011;42:1303-1306.P.347
- Thomsen L, Falcone MO. Lesions of the scapholunate ligament associated with minimally displaced or non-displaced fractures of the scaphoid waist. Which incidence? Chir Main 2012;31:234-238.
- Trumble TE, Clarke T, Kreder HJ. Non-union of the scaphoid: treatment with cannulated screws compared with treatment with Herbert screws. J Bone Joint Surg Am 1996;78(12):1829-1837.
- Trumble TE, Gilbert M, Murray LW, et al. Displaced scaphoid fractures treated with open reduction and internal fixation with a cannulated screw. J Bone Joint Surg Am 2000;82(5):633-641.
- Waizenegger M, Wastie ML, Barton NJ, et al. Scintigraphy in the evaluation of the “clinical” scaphoid fracture. J Hand Surg Br 1994;19(6):750-753.
- Wong TC, Yip TH, Wu WC. Carpal ligament injuries with acute scaphoid fractures: a combined wrist injury. J Hand Surg Br 2005;30: 415-418.
- Yip HS, Wu WC, Chang RY, et al. Percutaneous cannulated screw fixation of acute scaphoid waist fracture. J Hand Surg Br 2002; 27(1):42-46.Chapter 35Open Reduction and Internal Fixation of Scaphoid FracturesAsheesh Bedi Peter J.L. Jebson Levi Hinkelman
DEFINITION
The scaphoid is the most commonly fractured carpal bone, accounting for 1 in every 100,000 emergency department visits.15Scaphoid fractures typically result from a fall on an outstretched hand or less commonly following forced palmar flexion of the wrist20 or axial loading of the flexed wrist such as in punching.12Scaphoid nonunion or proximal pole avascular necrosis (AVN) after a fracture has been associated with considerable morbidity and a predictable pattern of wrist arthritis.18,21,25The complex anatomy and tenuous blood supply to the scaphoid make operative management of these fractures technically challenging.25
ANATOMY
The scaphoid has a complex three-dimensional geometry that has been likened to a “twisted peanut.” It can be divided into three regions: proximal pole, waist, and distal pole.The scaphoid functions as the primary link between the forearm and the distal carpal row and therefore plays a critical role in maintaining normal carpal kinematics.Articulating with the scaphoid fossa of the radius, the lunate, capitate, trapezium, and trapezoid, more than 70% of the scaphoid is covered with articular cartilage.Gelberman and Menon8 have described the vascular supply of the scaphoid. The main arterial supply is from the radial artery; it enters the scaphoid via two main branches:A dorsal branch, entering through the dorsal ridge, is the primary supply and provides 70% to 80% of the vascularity, including the entire proximal pole via retrograde endosteal branches.A volar branch, entering through the tubercle, supplies the remaining 20% to 30%, predominantly the distal pole and tuberosity.The proximal pole is at increased risk for AVN secondary to disruption of its tenuous retrograde blood supply after a fracture of the scaphoid waist or proximal pole.Due to its tenuous vascular supply, the scaphoid heals almost entirely by primary bone healing, resulting in minimal callus formation.The size and shape of the scaphoid, in combination with its precarious blood supply, demands attention to detail and accurate implantation of fixation devices during fracture fixation. Scaphoid dimensions vary between genders; the male scaphoid is usually longer and wider than the females. In addition, the diameter of mostcommercially available standard screws are larger than the proximal pole of the female scaphoid.11
PATHOGENESIS
Scaphoid fractures are most commonly seen in young, active males.15With the wrist dorsiflexed greater than 95 degrees, in combination with 10 degrees or more of radial deviation, the distal radius abuts the scaphoid and precipitates a fracture.15The scaphoid can also be fractured with forced palmar flexion of the wrist20 or axial loading of the flexed wrist.12 Most of these fractures occur at the waist region, although 10% to 20% occur in the proximal pole.Proximal pole fractures are associated with an increased risk of nonunion, delayed union, and AVN. In children, scaphoid fractures are less common and are most frequently seen in the distal pole.
NATURAL HISTORY
An untreated or inadequately treated scaphoid fracture has a higher likelihood of nonunion. The overall incidence of nonunion is estimated at 5% to 10%, but the risk is significantly increased with nonoperative treatment of a displaced waist or proximal pole fracture.The natural history of scaphoid nonunions is controversial, but they are believed to result in a predictable pattern of progressive radiocarpal and midcarpal arthritis.8,9,14,17,18,21,25In an established scaphoid nonunion, the distal portion of the scaphoid may flex, producing a “humpback” deformity of the scaphoid. The loss of scaphoid integrity can result in carpal instability and abnormal carpal kinematics, most frequently manifesting as a dorsal intercalated segment instability (DISI) pattern.The pattern of carpal instability and secondary arthrosis due to an unstable scaphoid nonunion has been termed an SNAC wrist (scaphoid nonunion advanced collapse pattern of wrist arthritis).14,21In the SNAC wrist, there is a loss of carpal height with proximal capitate migration, flexion and pronation of the scaphoid, and secondary midcarpal arthritis.21Factors associated with the development of a scaphoid fracture nonunion include the following17:Delayed diagnosis or treatment Inadequate immobilizationProximal fractureInitial and progressive fracture displacement Fracture comminutionPresence of associated carpal injuries (ie, perilunate injury)P.340
PATIENT HISTORY AND PHYSICAL FINDINGS
Scaphoid fractures classically occur in the active, young adult population. Patients present with radial-sided wrist pain.Classic physical examination findings include the following:Swelling over the dorsoradial aspect of the wrist Tenderness to palpation in the “anatomic snuffbox”Tenderness with palpation volarly over the distal tuberclePain with axial compression of the wrist (scaphoid compression test) Scaphoid fractures can be part of a greater arc injury.The physician should examine the entire wrist carefully for areas of tenderness and swelling.Plain radiographs are scrutinized for an associated ligamentous injury or disruption of the midcarpal joint as seen in the transscaphoid perilunate fracture-dislocation.
IMAGING AND OTHER DIAGNOSTIC STUDIES
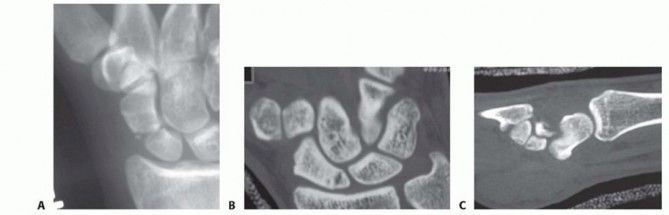
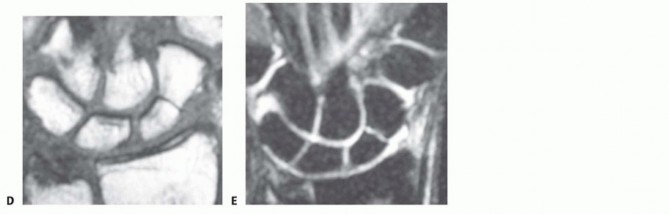
FIG 1 • A. Radiograph (scaphoid view) of an acute, displaced, comminuted scaphoid waist fracture. B,C. Axial and sagittal CT scan images demonstrating a fracture of the proximal pole of the scaphoid. D,E. T1- and T2-weighted MRI images demonstrating a nondisplaced scaphoid waist fracture. (Copyright Peter J.L. Jebson, MD.) The semipronated oblique view provides the best visualization of the waist and distal pole regions. The semisupinated oblique view provides the best visualization of the dorsal ridge.The lateral view permits an assessment of fracture angulation, carpal alignment, and carpal instability.The dedicated scaphoid view is a PA view with the wrist in ulnar deviation. This results in scaphoid extension, allowing visualization of the scaphoid in profile (FIG 1A).The following criteria define a displaced or unstable fracture as noted on plain radiographs2,9,17:At least 1 mm of displacementMore than 10 degrees of angular displacement Fracture comminutionRadiolunate angle of more than 15 degrees Scapholunate angle of more than 60 degrees Intrascaphoid angle of more than 35 degreesComputed tomography (CT) with reconstruction images in multiple planes is used to identify an acute fracture not detected on plain radiographs and to determine the amount of displacement and comminution (FIG 1B,C).CT is most useful in evaluating an established scaphoid nonunion or malunion.6Because plain radiographs are often unreliable, CT is preferred for confirming union after a scaphoid fracture particularly before permitting a return to contact sports.Magnetic resonance imaging (MRI) may be indicated in the evaluation of a suspected scaphoid fracture not detected on plain radiographs (FIG 1D,E). MRI is highly sensitive, withP.341a specificity approaching 100% when performed within 48 hours of injury.16Bone bruising without a fracture detected on MRI can lead to an occult fracture in 2% of cases.23MRI with intravenous gadolinium contrast is helpful in assessing the vascularity of the proximal pole, particularly in the patient with an established nonunion.A technetium bone scan has been shown to be up to 100% sensitive in identifying an occult fracture.27Unfortunately, it is also associated with a low specificity and often will not be positive immediately after the fracture.
DIFFERENTIAL DIAGNOSIS
Scapholunate injury Wrist sprainWrist contusionFracture of other carpal bone Greater arc injuryDistal radius fracture
NONOPERATIVE MANAGEMENT
Nonoperative management is indicated for a nondisplaced, stable scaphoid waist or distal pole fracture.Unstable fractures and nondisplaced fractures of the proximal pole are indications for internal fixation based on studies that have demonstrated a poor outcome with nonoperative treatment.2,4,17The appropriate type and duration of cast immobilization remain controversial and none has proven to be superior. Our preference is a short-arm thumb spica cast until the clinical examination and radiologic studies (usually a CT scan) confirm fracture union. If there are concerns for patient compliance, we prefer an initialperiod (4 to 6 weeks) of long-arm thumb spica cast immobilization.Clinical studies have failed to demonstrate any benefit from including the thumb or fingers in the cast.2,4 Similarly, wrist position has not been proven to improve scaphoid fracture healing.Numerous studies have revealed no difference in union rates for a long-arm versus short-arm cast; however,a randomized prospective study by Gellman et al10 documented a shorter time to union and fewer nonunions and delayed unions with initial use of a long-arm cast.The morbidity of a nonoperative approach, specifically cast immobilization, has become of increasing concern. A prolonged duration of immobilization is often required for waist fractures, and this can be accompanied by muscle atrophy, stiffness, reduced grip strength, and residual pain. In addition, cast immobilization can cause significant inconvenience for the patient and interference with activities of daily living. The prolonged duration of immobilization is of particular concern in the young laborer, athlete, or military personnel, who typically desireexpedient functional recovery.5,19,29If the clinical history and physical examination are suggestive of a scaphoid fracture but initial radiographs are negative, the wrist should be immobilized for 2 weeks. Repeat radiographs are then obtained. If a fracture is present, resorption at the fracture may be noted. If wrist pain and “snuffbox” tenderness persist but radiographsare negative, an MRI or CT scan may be obtained.16,27Alternatively, if there is a high index of suspicion at initial presentation with “normal” radiographs or if there is a need to know the status of the scaphoid, such as in the elite athlete, we prefer MRI.
SURGICAL MANAGEMENT
Indications for open reduction and internal fixation (ORIF) of scaphoid fractures include the following2,17:Proximal pole fractureA displaced, unstable fracture of the scaphoid waist Associated carpal instability or perilunate instability Associated distal radius fractureDelayed presentation (more than 3 to 4 weeks) with no prior treatmentA nondisplaced, stable scaphoid waist fracture in a patient who wishes to avoid the morbidity of cast immobilization. In this clinical scenario, operative treatment should occur only after an explanation of the rationale for, and the risks and benefits of, operative treatment versus cast immobilization.
PREOPERATIVE PLANNING
All imaging studies should be reviewed to accurately define the fracture pattern. Required equipment are as follows:Portable mini-fluoroscopy unit Kirschner wiresCannulated headless compression screw system. We prefer to use the Acutrak 2 or mini-Acutrak 2 screw system (Acumed, Beaverton, OR), but any cannulated screw system that permits screw insertion beneath the articular surface may be used.
POSITIONING
General or regional anesthesia may be used.The patient is positioned supine on the operating table with a radiolucent hand table at the shoulder level. The fluoroscopy unit is draped and positioned at the end of the hand table.A pneumatic tourniquet is carefully applied to the proximal arm.An intravenous antibiotic is provided before inflation of the tourniquet as prophylaxis for infection.The limb is prepared and draped, followed by exsanguination of the limb with an Esmarch bandage and tourniquet inflation, usually to a pressure of 250 mm Hg.
APPROACH
ORIF of scaphoid fractures can be performed through either a dorsal or volar approach. The specific approaches that will be described include the following:Open dorsal approach19 Open volar approachP.342
TECHNIQUES
Open Dorsal Approach (Authors' Preferred Approach)
Open Dorsal Approach (Authors' Preferred Approach)
EXPOSURE


TECH FIG 1 • A. Skin incision used for ORIF of scaphoid fractures via the dorsal approach. B. Retracting the thumb and wrist extensor tendons radially and the finger extensor tendons ulnarly facilitates exposure of the underlying capsule. C. A limited capsulotomy should be performed to expose the proximal scaphoid and scapholunate ligament. (Copyright of Peter J.L. Jebson, MD.)
FRACTURE REDUCTION AND PROVISIONAL FIXATION
Distract the carpus manually via longitudinal traction on the index and long fingers.If the fracture is displaced, insert 0.045-inch Kirschner wire joysticks perpendicularly into the proximal and distal scaphoid fragments to assist in the reduction (TECH FIG 2A).The accuracy of the reduction can be determined by assessing congruency of the radioscaphoid and scaphocapitate articulations.When a satisfactory reduction has been achieved, obtain provisional fixation with parallel derotational 0.045-inch Kirschner wires.The first wire is inserted dorsal and ulnar to the central axis of the scaphoid, into the trapezium for enhanced stability.The second derotational wire may be inserted volar and radial to the anticipated central axis insertion site if more fixation is needed.The derotational wires must be placed such that they will not interfere with central axis guidewire placement, reaming, and screw insertion (TECH FIG 2B).
GUIDEWIRE PLACEMENT

SCREW INSERTION


TECH FIG 4 • A. Determining the appropriate screw length. B. Reaming with the cannulated reamer. C,D. Insertion of the screw. A-D: Top is distal, bottom is proximal, left is radial, and right is ulnar. (Copyright Peter J.L. Jebson, MD.)
Open Volar Approach
OPEN VOLAR APPROACH
EXPOSURE
Radially, deviate the wrist and palpate the scaphoid tubercle.Make a 3- to 4-cm incision centered over the scaphoid tubercle, directed distally toward the base of the thumb and proximally over the flexor carpi radialis (FCR) tendon sheath. If the superficial volar branch of the radial artery is encountered, cauterize it at the level of the wrist flexion crease.Open the FCR sheath, and retract the tendon ulnarly. Open the floor of the sheath distally to expose the underlying volar wrist capsule.Distally, develop the interval by splitting the origin of the thenar muscles in line with their fibers over the distal scaphoid and trapezium.Incise the capsule longitudinally, taking care to avoid damage to the underlying articular cartilage.Proximally, divide the thickened radiolunate and radioscaphocapitate ligaments to allow exposure of theproximal scaphoid pole.Identify the scaphotrapezial joint with a Freer elevator and bluntly expose it.Dissection over the radial aspect of the scaphoid is limited to avoid injury to the dorsal ridge vessel.Define and clear the fracture site by irrigation, sharp excision of periosteal flaps, and curetting of debris and hematoma.Assess the instability of the fracture by wrist manipulation.It is critical to identify any bone loss, as compression during screw placement can result in an iatrogenic malunion.
FRACTURE REDUCTION AND FIXATION
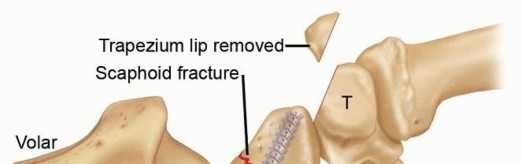
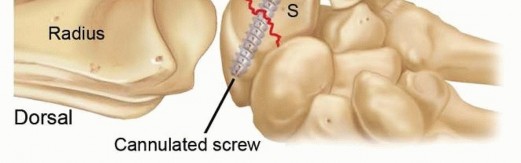
TECH FIG 5 • Accurate insertion of a screw via the volar approach usually requires partial resection or dorsal displacement of the volar trapezium to expose the distal scaphoid. The cannulated compression screw may be inserted using a freehand technique or a commercial device, which simultaneously facilitates fracture reduction and guidewire positioning.Fluoroscopy is invaluable during wire and screw insertion and to confirm accurate placement and fracture reduction as described earlier.Precisely repair the volar wrist capsule and radiolunate and radioscaphocapitate ligaments with permanentsuture.
PEARLS AND PITFALLS
Injury to thescaphoid blood supply1. Meticulous limited dissection of the capsule. Avoid any dissection on the dorsalridge of the scaphoid.Malpositioningof guidewire1. Pronate and flex wrist during the dorsal approach to allow appropriate trajectory.Confirm position on multiple views to ensure insertion in the central axis of the scaphoid.Screw position ▪ Select a screw that is 4 mm shorter than measured length unless fracturefragments are separated; in that case, choose a shorter screw.Reduction ofan unstable fracture1. Perpendicular Kirschner wire joysticks inserted into the proximal and distalscaphoid fragments are useful to obtain a reduction.2. Provisional derotational Kirschner wires placed before screw insertion can be used to stabilize fragments during screw insertion.3. Recognize comminution and bone loss to avoid inadvertent shortening or malreduction with screw compression.Small proximalpole fracture1. Use of a small screw (ie, mini-Acutrak 2) may be necessary to preventcomminution of the proximal fragment.2. Confirm central axis screw position, especially in the proximal pole.
POSTOPERATIVE CARE
The patient is immobilized in a below-elbow volar splint and discharged to home with instructions on strict limb elevation and frequent digital range-of-motion exercises.At 2 weeks, the patient returns for suture removal. Range-of-motion exercises are begun, and a removable forearm-based thumb splint is worn. The splint is discontinued at 6 weeks postoperatively.If the fracture involves the proximal pole or if significant comminution was noted at surgery and there is concern regarding stability of the fixation, immobilization in a short-arm cast for 6 to 10 weeks is indicated. Typically, such fractures take longer to achieve union.After cast removal, a formal supervised therapy program is initiated to achieve satisfactory range of motion, strength, and function.Fracture healing is assessed at 2, 6, and 12 weeks postoperatively with plain radiography. Fracture union is defined as progressive obliteration of the fracture and clear trabeculation across the fracture site (FIG 2).If there is any question regarding fracture union, a CT scan is obtained at 3 months postoperatively or before the patient is allowed to return to unrestricted sporting activities.
OUTCOMES
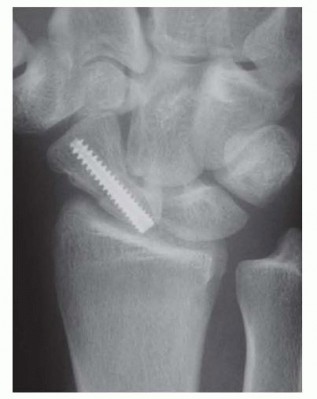
FIG 2 • A healed scaphoid waist fracture after ORIF via the dorsal approach. Although the screw may appear slightly long, both the proximal scaphoid and distal scaphoid are covered with hyaline cartilage not detected on diagnostic imaging. (Copyright Peter J.L. Jebson, MD.) A volar approach has traditionally been used for screw insertion. However, recent studies have raised potential concerns regarding eccentric screw placement and damage to the scaphotrapezial articulationwith this approach.29Our preferred technique for fixation of a scaphoid proximal pole or waist region fracture involves a limiteddorsal approach with compression screw fixation.19 The technique is simple and permits visualization of a reliable starting point for screw placement within the central axis of the scaphoid, offering a significant potential advantage over the volar approach. We recently reported our clinical experience in a consecutiveseries of nondisplaced scaphoid waist fractures.3
COMPLICATIONS
Postoperative wound infections are rare and can be prevented with routine preoperative antibiotic prophylaxis, thorough wound irrigation, and appropriate soft tissue management.Intraoperative technical problemsInadvertent bending or breakage of the guidewire can occur if the wrist is dorsiflexed with the wire in position or during drilling before screw insertion.Care should be taken to confirm that the screw is fully seated beneath the articular cartilage to avoid prominence and erosion of the distal radius articular surface. Similarly, failure to carefully judge accurate screw length intraoperatively can result in prominence within the scaphotrapezial articulation.Nonunion with or without AVN can occur despite compression screw fixation, particularly with a proximal pole or displaced waist fracture. Stripping of the dorsal ridge vasculature should be avoided. Supplemental cancellous bone graft from the distal radius may be used at the time of fixation of a displaced or comminuted fracture if desired.Other potential but rare complications Hypertrophic scarInjury to the dorsal branches of the superficial radial nerveDamage to the scaphotrapezial articulation Proximal pole fragment comminution
REFERENCES
- Adams BD, Blair WF, Reagan DS, et al. Technical factors related to Herbert screw fixation. J Hand Surg Am 1988;13(6):893-899.
- Amadio PC, Moran SL. Fractures of the carpal bones. In: Green D, Hotchkiss R, Pederson WC, eds. Green's Operative Hand Surgery, ed 5. Philadelphia: Churchill Livingstone, 2005:711-740.
- Bedi A, Jebson PJ, Hayden RJ, et al. Internal fixation of acute, nondisplaced scaphoid waist fractures via a limited dorsal approach: an assessment of radiographic and functional outcomes. J Hand Surg Am 2007;32(3):326-333.
- Burge P. Closed cast treatment of scaphoid fractures. Hand Clin 2001;17:541-552.
- Chen AC, Chao EK, Hung SS, et al. Percutaneous screw fixation for unstable scaphoid fractures. J Trauma 2005;59:184-187.
- Dias JJ, Taylor M, Thompson J, et al. Radiographic signs of union of scaphoid fractures. An analysis of inter-observer agreement and reproducibility. J Bone Joint Surg Br 1988;70(2):299-301.
- Dodds SD, Panjabi MM, Slade JF III. Screw fixation of scaphoid fractures: a biomechanical assessment of screw length and screw augmentation. J Hand Surg Am 2006;31(3):405-413.
- Gelberman RH, Menon J. The vascularity of the scaphoid bone. J Hand Surg Am 1980;5(5):508-513.
- Gelberman RH, Wolock BS, Siegel DB. Fractures and non-unions of the carpal scaphoid. J Bone Joint Surg Am 1989;71A:1560-1565.
- Gellman H, Caputo RJ, Carter V, et al. Comparison of short and long thumb-spica casts for non-displaced fractures of the carpal scaphoid. J Bone Joint Surg Am 1989;71(3):354-357.
- Heinzelmann AD, Archer G, Bindra RR. Anthropometry of the human scaphoid. J Hand Surg Am 2007;32(7):1005-1008.
- Horii E, Nakamura R, Watanabe K, et al. Scaphoid fracture as a “puncher's fracture.” J Orthop Trauma 1994;8:107-110.
- Jørgsholm P, Thomsen NO, Björkman A, et al. The incidence of intrinsic and extrinsic ligament injuries in scaphoid waist fractures. J Hand Surg Am 2010;35(3):368-374.
- Kerluke L, McCabe SJ. Nonunion of the scaphoid: a critical analysis of recent natural history studies. J Hand Surg Am 1993;18(1):1-3.
- Kozin SH. Incidence, mechanism, and natural history of scaphoid fractures. Hand Clin 2001;17:515-524.
- Kukla C, Gaebler C, Breitenseher MJ, et al. Occult fractures of the scaphoid. The diagnostic usefulness and indirect economic repercussions of radiography versus magnetic resonance scanning. J Hand Surg Br 1997;22(6):810-813.
- Leslie IJ, Dickson RA. The fractured carpal scaphoid. Natural history and factors influencing outcome. J Bone Joint Surg Br 1981; 63-B(2):225-230.
- Mack GR, Bosse MJ, Gelberman RH, et al. The natural history of scaphoid nonunion. J Bone Joint Surg Am 1984;66(4):504-509.
- Martus J, Bedi A, Jebson PJL. Cannulated variable pitch compression screw fixation of scaphoid fractures using a limited dorsal approach. Tech Hand Up Extrem Surg 2005;9:202-206.
- Ritchie JV, Munter DW. Emergency department evaluation and treatment of wrist injuries. Emerg Med Clin North Am 1999;17: 823-842.
- Ruby LK, Stinson J, Belsky MR. The natural history of scaphoid non-union. A review of fifty-five cases. J Bone Joint Surg Am 1985;67(3):428-432.
- Schädel-Höpfner M, Junge A, Böhringer G. Scapholunate ligament injury occurring with scaphoid fracture—a rare coincidence? J Hand Surg Br 2005;30:137-142.
- Thavarajah D, Syed T, Shah Y, et al. Does scaphoid bone bruising lead to occult fractures? A prospectivestudy of 50 patients. Injury 2011;42:1303-1306.P.347
- Thomsen L, Falcone MO. Lesions of the scapholunate ligament associated with minimally displaced or non-displaced fractures of the scaphoid waist. Which incidence? Chir Main 2012;31:234-238.
- Trumble TE, Clarke T, Kreder HJ. Non-union of the scaphoid: treatment with cannulated screws compared with treatment with Herbert screws. J Bone Joint Surg Am 1996;78(12):1829-1837.
- Trumble TE, Gilbert M, Murray LW, et al. Displaced scaphoid fractures treated with open reduction and internal fixation with a cannulated screw. J Bone Joint Surg Am 2000;82(5):633-641.
- Waizenegger M, Wastie ML, Barton NJ, et al. Scintigraphy in the evaluation of the “clinical” scaphoid fracture. J Hand Surg Br 1994;19(6):750-753.
- Wong TC, Yip TH, Wu WC. Carpal ligament injuries with acute scaphoid fractures: a combined wrist injury. J Hand Surg Br 2005;30: 415-418.
- Yip HS, Wu WC, Chang RY, et al. Percutaneous cannulated screw fixation of acute scaphoid waist fracture. J Hand Surg Br 2002; 27(1):42-46.
