Open Reduction and Internal Fixation of Radial Head and Neck Fractures
DEFINITION
Radial head and neck fractures are the most common elbow fractures in adults representing 33% of elbow fractures.They may occur in isolation or with concurrent osseous, osteochondral, and/or ligamentous injuries.Management (which involves nonoperative, open reduction internal fixation [ORIF], fragment excision, radial head excision, or radial head replacement) is aimed at restoring motion or both motion and stability to the elbow and forearm, depending on the pattern of injury. This chapter focuses on the decision-making principles and operative techniques for ORIF of radial head and neck fractures.
ANATOMY AND BIOMECHANICS
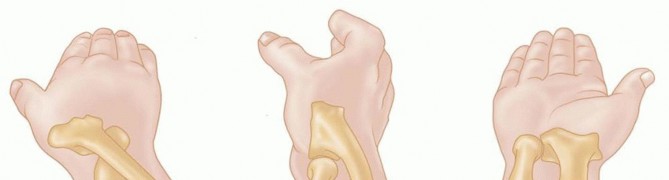
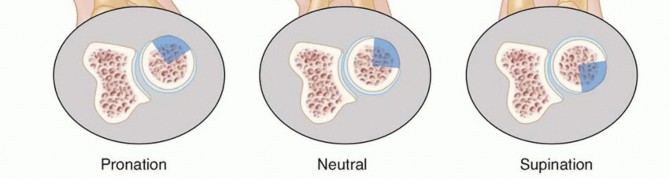
FIG 1 • The safe zone is a roughly 90-degree arc of the radial head that does not articulate with the ulna in the PRUJ with full supination and pronation. With the wrist in neutral rotation, the safe zone is anterolateral.


FIG 2 • A. The radial recurrent artery, a branch of the radial artery, provides the main blood supply to the radial head. B. In most cadaveric specimens, a branch of the radial recurrent penetrates the radial head in the safe zone. (From Yamaguchi K, Sweet FA, Bindra R, et al. The extraosseous and intraosseous arterial anatomy of the adult elbow. J Bone Joint Surg Am 1997;79[11]:1653-1662.)
PATHOGENESIS
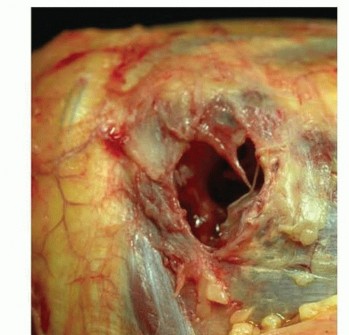
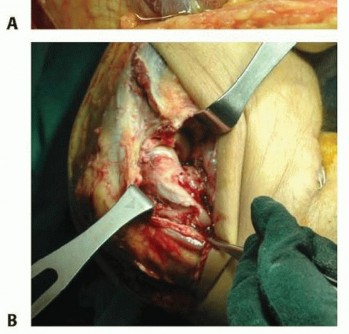
FIG 3 • Soft tissue injuries occur with unstable radial head fractures. Sample pictures showing (A) large capsular rupture and (B) avulsion of the lateral collateral ligament (LCL) and common extensor tendons from the lateral epicondyle.

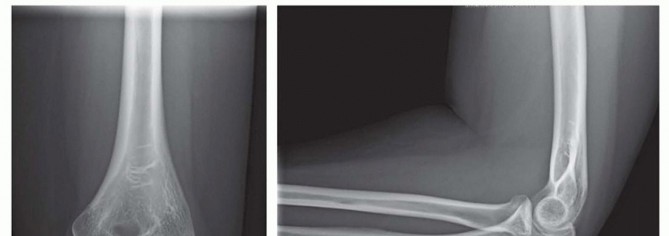
FIG 4 • AP x-ray showing a depressed articular fracture with impaction at the radial neck. This fracture pattern is highly suspicious for an Essex-Lopresti fracture. Radial head replacement is recommended. If ORIF is performed, the DRUJ should be stabilized to prevent instability.
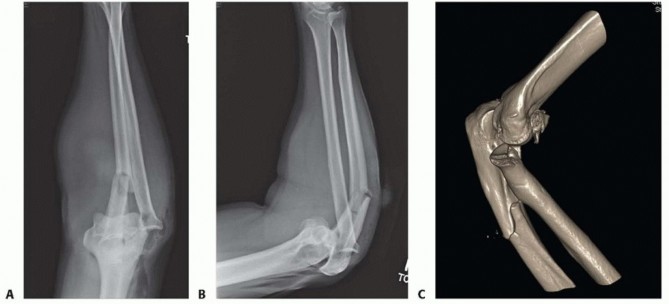
FIG 5 • A,B. AP and lateral x-ray showing a type II Monteggia fracture—posterior dislocation of radial head (or fracture) and proximal ulnar fracture with posterior angulation. C. CT scan clearly showing impaction fracture of the radial head that may not be appreciable on x-ray.
NATURAL HISTORY
The original Mason classification was modified by Johnson, and then Morrey. Hotchkiss proposed that the classification system be used to provide guidance for treatment. It has poor intraobserver and interobserverreliability ( FIG 6).9
TYPE I FRACTURES
Nondisplaced and offer no block to pronation and supination on examination Represents approximately 82% of radial head fractures 18Nonoperative treatment generally results in good to excellent outcomes with minimal loss of motion or resultantarthrosis. 1,3,8,12Stiffness due to capsular contracture is the main reason for a poor outcome; however, it can often be managed successfully with physical therapy.
TYPE II FRACTURES
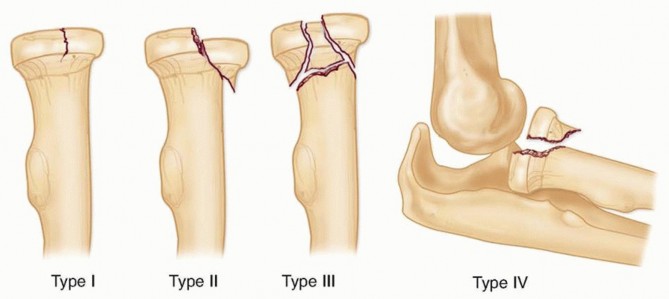
FIG 6 • The modified Mason classification for radial head fractures. Represents approximately 14% of radial head fractures 18Earlier studies suggested nonoperative treatment or radial head excision as the standard treatment, 13,19,20,23 but as knowledge and technology advanced, optimal treatment has become more controversial.Greater than 2 mm of displacement has often been cited as an indication for ORIF, but good results have been obtained in studies treating 2 to 5 mm of displacement nonoperatively. 1,12A mechanical block is the only clear indication for surgery.A recent meta-analysis 16 found successful nonoperative treatment in 80% compared to successful ORIFtreatment in 93% for stable Mason type II fractures; however, the authors concluded that there was insufficient evidence to recommend optimal treatment.Complications from nonoperative treatment such as painful clicking, nonunion, and arthrosis can be treated with radial head excision or arthroplasty; however, it is considered with modest increase in function. It has shown23% fair or poor results at 15 years of follow-up. 5P.166Delayed excision of the radial head after failed nonoperative management may be considered with modest increase in function; it has shown 23% fair or poor results at 15 years of follow-up. 5 Other studies suggested that there is no difference between delayed and primary excision.11
TYPE III FRACTURES
Comminuted or impacted articular fractures (see FIG 4) are optimally managed with prosthetic replacement. Represents approximately 3% of radial head fractures18Radial head arthroplasty or excision is considered when satisfactory reduction or stable fixation is not obtainedor in comminuted fractures because fixation of a radial head with more than three articular fragments is fraught with poor results. 22Results of excision are poor in patients with concomitant MCL, coronoid, or interosseous membrane injury.Radial head resection should be reserved for patients with low functional demands, limited life expectancy, or in the presence of infection, and when the surgeon has excluded elbow instability with a fluoroscopic examination.Radiographic, but usually clinically silent, degenerative changes such as cysts, sclerosis, and osteophytes occur radiographically in about 75% of elbows after radial head excision.There is also a demonstrable increase in ulnar variance at the wrist and increased carrying angle and a 10% to 20% loss of strength is expected.Radial head arthroplasty can provide radiocapitellar contact similar to the native radial head and thus resists valgus and posterior instability. Additionally, it resists proximal migration of the radius in response to axial loading. It facilitates uneventful healing of the MCL, interosseous ligaments, and DRUJ.
TYPE IV FRACTURES
Radial head fractures associated with elbow instability. The radial head should never be resected in the acute setting.Represents approximately 1% of radial head fractures 18Treatment involves immediate reduction of the elbow joint and treatment of the radial head fracture and associated bony injuries. Whether the radial head is fixed or replaced, it must be capable of bearing load immediately. If the radial head can be fixed, repair of the torn ligaments and application of a hinged fixator to protect the repaired radial head may be considered. Otherwise, satisfactory results have been obtained withradial head replacement without ligamentous repair. 10
PATIENT HISTORY AND PHYSICAL FINDINGS
HISTORY


FIG 7 • MCL injury with extensive medial ecchymosis.
PHYSICAL EXAMINATION
Physical examination should include neurovascular status, examination of the joint above (shoulder) and below (wrist), and examination of the skin to look for medial ecchymosis ( FIG 7), which may suggest injury to the MCL.A detailed examination of the elbow must include bony palpation of the medial and lateral epicondyles, olecranon process, DRUJ, and radial head as well as the squeeze test of the interosseous membrane and DRUJ to screen for potential longitudinal instability.Varus and valgus stress testing, with or without fluoroscopy, can indicate injury to the anterior band of the MCL or to the lateral ulnar collateral ligament, respectively.Range-of-motion and stress examinations are vital to proper decision making and may obviate the need for advanced imaging if performed correctly with adequate anesthesia. If omitted, this will lead to undiagnosed associated injuries and may result in flawed decision making.In the emergency department or office, adequate anesthesia may be obtained by aspirating hematoma, then injecting the elbow joint with 5 mL of local anesthetic and examining the elbow under fluoroscopy. This may be performed by the traditional lateral injection in the “soft spot” or posteriorly into theolecranon fossa ( FIG 8).25 A mechanical block is an indication for operative intervention.If operative intervention is clearly indicated, this examination can be performed under a general anesthetic, provided the surgeon and patient are prepared for a change in operative plan as dictated by the examination.Normal values are 0 to 145 degrees of flexion-extension, 85 degrees of supination, and 80 degrees of pronation. The examiner should check for a bony block to motion.
DIAGNOSTIC STUDIES
RADIOGRAPHY
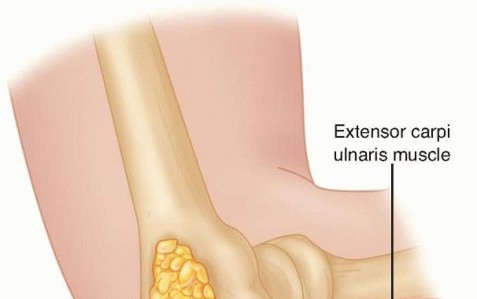
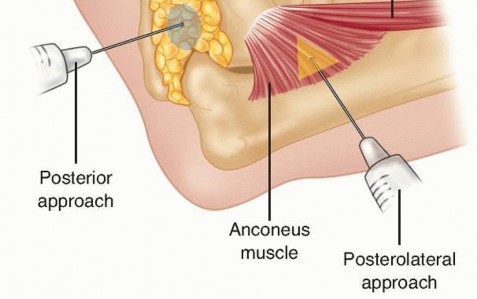
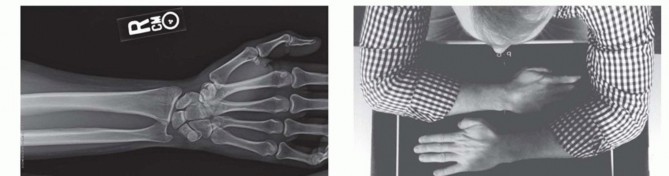
FIG 8 • The elbow joint can be aspirated and injected through the posterior and posterolateral approaches. They are equally effective and should be used based on soft tissue injury. If the examination reveals wrist or forearm tenderness, the examiner should have a low threshold for obtaining bilateral wrist posteroanterior (PA) views to rule out an Essex-Lopresti lesion. Alternatively, this can be done with a one cassette view to minimize radiation exposure ( FIG 9).
MAGNETIC RESONANCE IMAGING

COMPUTED TOMOGRAPHY
If decision is made for operative treatment, we routinely obtain a computed tomography (CT) scan to better understand the fracture pattern for preoperative planning, so that operative time is efficient and to minimize intraoperative surprises. Three-dimensional reconstructions provide further information not always easily appreciated on routine CT scans.
DIFFERENTIAL DIAGNOSIS
Simple elbow dislocation Distal humerus fracture Olecranon fracture Septic elbow
NONOPERATIVE MANAGEMENT
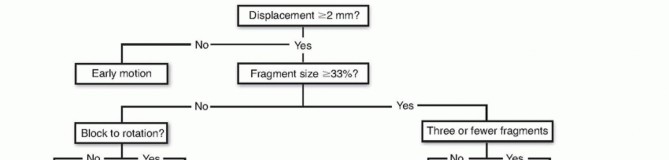
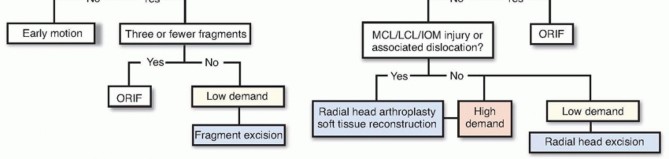
FIG 10 • Treatment algorithm for radial head fractures. If there is a blockage or instability, excision, fixation, or arthroplasty is recommended based on patient factors and instability.A recent report regarding the long-term results of nonoperative management (similar to that described) of 49 patients with radial head fractures encompassing over 30% of the joint surface and displaced 2 to 5 mm revealed that 81% of patients had no subjective complaints and minimal loss of motion versus the uninjuredextremity. Only one patient had daily pain. 1
SURGICAL MANAGEMENT
PREOPERATIVE PLANNING
It is essential to review all imaging and perform thorough history, physical, and fluoroscopic examinations before making an incision.The presence of instability or associated fractures warrants a more extensile approach.
POSITIONING
Positioning depends on the planned approach and the surgeon's preference.We prefer the patient supine with the affected extremity brought across the chest over a bump to allow access to the posterolateral elbow.A sterile tourniquet is placed high on the arm.
APPROACH
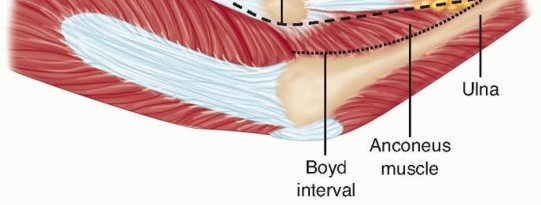
FIG 11 • Surgical intervals for the Boyd approach and the Kocher approach. P.169
TECHNIQUES
KOCHER APPROACH




TECH FIG 1 • Kocher approach. A. The skin incision proceeds distally from the posterolateral aspect of the lateral epicondyle to the posterior aspect of the proximal radius. B. Full-thickness flaps are made and the fascial interval between the extensor carpi ulnaris and anconeus muscles is identified. C. With longitudinal incision of the fascia and blunt division of the muscles, the joint capsule is evident. D. The capsule is longitudinally incised, and the fascia is tagged with figure-8 stitches for later anatomic repair.

TECH FIG 2 • Modified Wrightington approach. A. Make an 8-cm longitudinal incision at the junction of the ulna and anconeus starting about four fingerbreadths distal to the olecranon and extending 2 cm proximal to the olecranon.(continued)
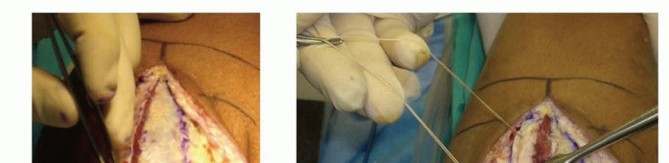
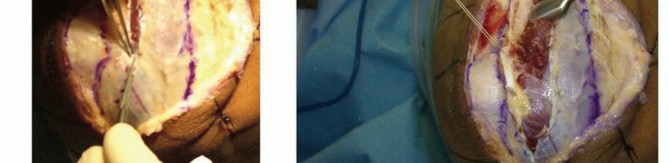
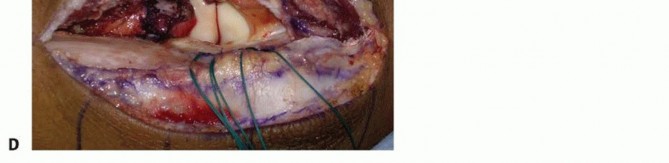
TECH FIG 2 •(continued)B. The interval between the ulna and anconeus is incised sharply, with care taken not to violate the periosteum or muscle to minimize the risk of proximal radioulnar synostosis. C. Blunt elevation of the anconeus is crucial to avoid damaging the capsule or lateral ligament complex. D. The capsule and lateral ligament complex are tagged during the approach to facilitate final repair with suture anchors.
FRACTURE INSPECTION AND PREPARATION
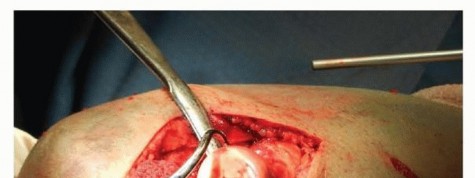

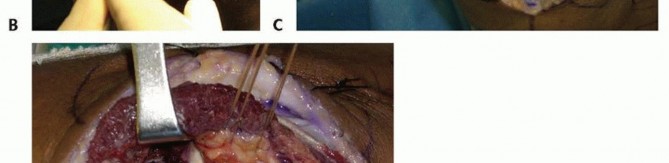
TECH FIG 3 • The modified Wrightington approach allows for full visualization of the radial head and fracture by subluxing the radial head posteriorly out of the joint.
REDUCTION AND PROVISIONAL FIXATION
FIXATION



TECH FIG 4 • Tenaculum clamps and 0.062-inch Kirschner wires are placed outside the zone of planned definitive fixation to provisionally hold the reduction. Two Biotrak screws are inserted for definitive fixation while the fracture is held reduced.
Closure
Any releases or injury to the annular ligament or lateral ulnar collateral ligament must be repaired anatomically. Drill holes with transosseous sutures are a proven method, but most authors now use suture anchors with reproducible results.
Skin closure is performed in standard fashion with drains at the surgeon's discretion.
CLOSURE
PEARLS AND PITFALLS
Protection of ▪ Pronation of the forearm moves the posterior interosseous nerve away from thethe posterior operative field during posterior approaches. interosseous ▪ Dissection should remain subperiosteally. nerveComminution ▪ We have a low threshold for excision or arthroplasty in the setting of comminution.1.A fluoroscopy unit should be available for examination under anesthesia beforeExamination1.A thorough fluoroscopic examination is the most important factor in deciding whattreatment is appropriate. To obtain a true lateral view, we recommend abducting the arm and externally rotating the shoulder while placing the elbow on the image intensifier.1.Prosthetic radial head replacement should be discussed with the patient as anoption and should be available in the room should the fracture prove to be comminuted.2.A hinged external fixator should be available if instability may be an issue.Hardwaresterile preparation.Fluoroscopy
POSTOPERATIVE CARE
The elbow is immobilized in a splint for 7 to 10 days.Serial x-rays are obtained to detect any loss of reduction at immediate postoperative, 2 weeks, 6 weeks, and 3 months, until healing is achieved ( FIG 12).Active range of motion is allowed as soon as tolerable. Supervised therapy may be considered if the patient is not making adequate progress.Associated injuries may call for more protected range of motion.Light activities of daily living are allowed at 2 weeks, with increased weight bearing at 6 weeks.
OUTCOMES
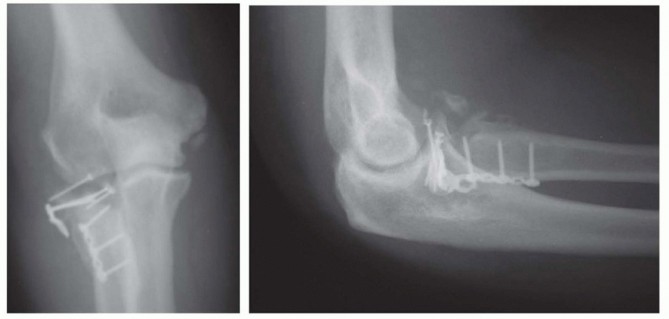
The results of ORIF depend both on host factors such as the type of fracture, smoking, compliance, level of physical demand as well as surgical and rehabilitation protocols.In uncomplicated fractures, over 90% satisfactory results can be expected.Complications and resultant secondary procedures will be more likely in cases with undiagnosed instability and associated injury.P.172 FIG 12 • Postoperative x-rays showing anatomic reduction of the radial head fracture. The Biotrak screws are radiolucent. Note that anchor holes are seen at the crista supinatoris where the lateral ulnar collateral ligament (LUCL) and annular ligament complex are repaired.

COMPLICATIONS


FIG 13 • A. Oblique radiograph demonstrating prominent hardware limiting forearm rotation. B. Arthroscopic view in the lateral gutter demonstrating hardware impingement at the PRUJ.Early and late instability from missed or failed treatment of associated injuriesThe rate of avascular necrosis is about 10%, significantly higher in displaced fractures. This is expected given that the radial recurrent artery inserts in the safe zone where hardware is placed. This is generally clinically silent.Loss of reduction Nonunion ( FIG 14)P.173 FIG 14 • ORIF of radial neck fracture that went on to nonunion and avascular necrosis.
REFERENCES
- Akesson T, Herbertsson P, Josefsson PO, et al. Primary nonoperative treatment of moderately displaced two-part fractures of the radial head. J Bone Joint Surg Am 2006;88(9):1909-1914.
- Amis AA, Miller JH. The mechanisms of elbow fractures: an investigation using impact tests in vitro. Injury 1995;26:163-168.
- Antuna SA, Sánchez-Márquez JM, Barco R. Long-term results of radial head resection following isolated radial head fractures in patients younger than forty years old. J Bone Joint Surg Am 2010;92:558-566.
- Boyd HB. Surgical exposure of the ulna and proximal third of the radius through one incision. Surg Gynecol Obstet 1940;71:86-88.
- Broberg MA, Morrey BF. Results of delayed excision of the radial head after fracture. J Bone Joint Surg Am 1986;68(5):669-674.
- Broberg MA, Morrey BF. Results of treatment of fracture-elbow dislocations of the elbow and intraarticular fractures. Clin Orthop Relat Res 1989;246:126-130.
- Caputo AE, Mazzocca AD, Sontoro VM. The nonarticulating portion of the radial head: anatomic and clinical correlations for internal fixation. J Hand Surg Am 1998;23(6):1082-1090.
- Esser RD, Davis S, Taavao T. Fractures of the radial head treated by internal fixation: late results in 26 cases. J Orthop Trauma 1995;9: 318-323.
- Essex-Lopresti P. Fractures of the radial head with distal radioulnar dislocation. J Bone Joint Surg Br 1951;33(2):244-250.
- Harrington IJ, Tountas AA. Replacement of the radial head in the treatment of unstable elbow fractures. Injury 1981;12(5):405-412.
- Herbertsson P, Josefsson PO, Hasserius R, et al. Fractures of the radial head and neck treated with radial head excision. J Bone Joint Surg Am 2004;86-A(9):1925-1930.
- Herbertsson P, Josefsson PO, Hasserius R, et al. Uncomplicated Mason type-II and III fractures of the radial head and neck in adults. A long-term follow-up study. J Bone Joint Surg Am 2004;86-A(3):569-574.
- Hotchkiss RN. Fractures and dislocations of the elbow. In: Rockwood CA Jr, Green DP, eds. Fractures in Adults, ed 4. Philadelphia: Lippincott-Raven, 1996:929-1024.
- Itamura JM, Roidis NT, Chong AK, et al. Computed tomography study of radial head morphology. J Shoulder Elbow Surg 2008; 17(2):347-354.
- Itamura J, Roidis N, Mirzayan R, et al. Radial head fractures: MRI evaluation of associated injuries. J Shoulder Elbow Surg 2005;14(4): 421-424.
- Kaas L, Struijs PA, Ring D, et al. Treatment of Mason type II radial head fractures without associated fractures or elbow dislocation: a systematic review. J Hand Surg Am 2012;37(7):1416-1421.
- Kaas L, van Riet RP, Turkenburg JL, et al. Magnetic resonance imaging in radial head fractures: most associated injuries are not clinically relevant. J Shoulder Elbow Surg 2011;20(8):1282-1288.
- Kovar FM, Jaindl M, Thalhammer G, et al. Incidence and analysis of radial head and neck fractures. World J Orthop 2013;4(2):80-84.
- McKee MD, Jupiter JB. Trauma to the adult elbow and fractures of the distal humerus. In: Browner BD, Jupiter JR, Levine AM, et al, eds. Skeletal Trauma, ed 2. Philadelphia: WB Saunders, 1998:1455-1522.
- Morrey BF. Radial head fracture. In: Morrey BF, ed. The Elbow and Its Disorders, ed 3. Philadelphia: WB Saunders, 2000:341-364.
- Morrey BF, An KN, Stormont TJ. Force transmission through the radial head. J Bone Joint Surg Am 1988;70(2):250-256.
- Ring D, Quintero J, Jupiter JB. Open reduction and internal fixation of fractures of the radial head. J Bone Joint Surg Am 2002; 84-A(10):1811-1815.
- Roidis NT, Papadakis SA, Rigopoulos N, et al. Current concepts and controversies in the management of radial head fractures. Orthopedics 2006;29(10):904-916.
- Stanley JK, Penn DS, Wasseem M. Exposure of the head of the radius using the Wrightington approach. J Bone Joint Surg Br 2006; 88(9):1178-1182.
- Tang CW, Skaggs DL, Kay RM. Elbow aspiration and arthrogram: an alternative method. Am J Orthop 2001;30:256.
- Yamaguchi K, Sweet FA, Bindra R, et al. The extraosseous and intraosseous arterial anatomy of the adult elbow. J Bone Joint Surg Am 1997;79(11):1653-1662.
