DEFINITION
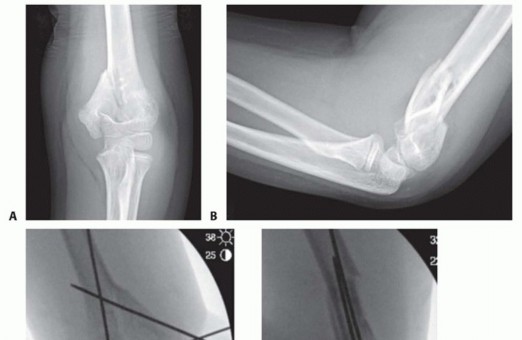
T-condylar fractures of the distal humerus in children and adolescents are relatively rare occurrences. They are thought to represent 2% of all pediatric elbow fractures.5The proposed mechanism is similar to that of pediatric supracondylar fractures but with a higher energy mechanism of injury.6 FIG 1 • A,B. An 8-year-old boy with T-condylar distal humerus fracture. C,D. Fixed with mini-open reduction with intercondylar screw compression and K-wire fixation of the distal humerus to the shaft. E,F. After hardware removal, the patient had 0 to 140 degrees range of motion with no pain.


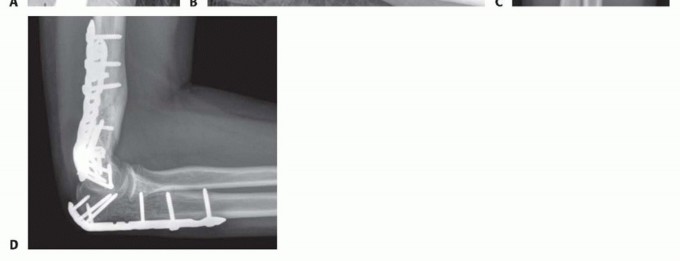
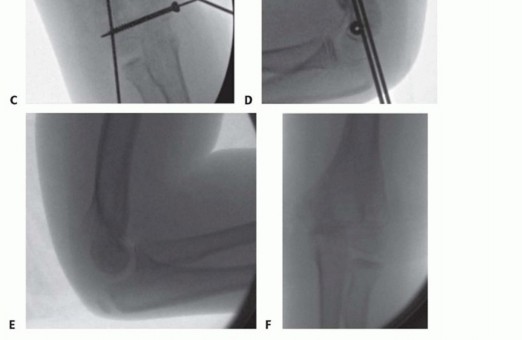
FIG 2 • A,B. A 15-year-old boy with type IIIA open distal humerus comminuted T-condylar humerus fracture. C,D. Three months following open reduction and internal fixation with olecranon osteotomy. Range of motion 0 to 140 degrees with no pain. Older children and young adolescents will often require an open approach. Comminution in the fossa may necessitate an olecranon osteotomy (FIG 2).Generally, pediatric fractures are less comminuted than adult fractures and may not require a full osteotomy.A Morrey slide approach is used in such a case where the triceps and ulnar periosteum are elevated off the ulna medially to expose the distal humerus without performing an osteotomy.3It was originally described to avoid olecranon osteotomies in cases where total elbow replacement would be a salvage operation.It can be useful in adolescents because the fractures are not as comminuted, but excellent visualization of the joint is desirable to provide anatomic reduction and restoration of elbow function. FIG 3 • A. A 13-year-old boy with a T-condylar humerus fracture with coronal split of the capitellum. B.


ANATOMY
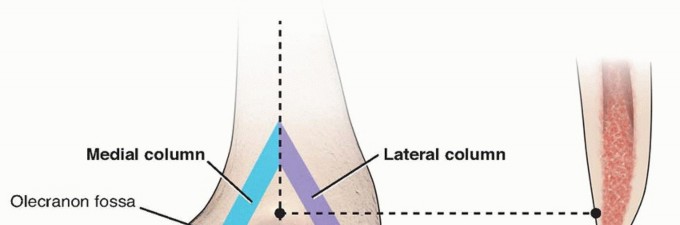
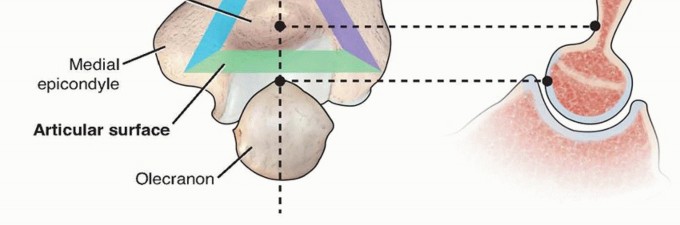
FIG 4• Triangle of stability concept. The mechanical properties of the distal humerus are based on a triangle of stability, comprising the medial and lateral columns and the articular surface. (Adapted from Bonczar MR, Rikli D, Ring D. Distal humerus 13-C1 open reduction; perpendicular [biplanar] plating. AO Foundation Web site. Available at:http://bit.ly/1wEegQS. Published June 21, 2007. Accessed November 1, 2013.) Posteromedially, the ulnar nerve travels through a groove in the distal humerus called thecubital tunnel. The nerve must be exposed along the medial border of the triceps down to the first motor branch, which pierces the flexor carpi ulnaris.The triceps covers the distal humerus and attaches to the proximal ulna at the olecranon process. The olecranon obscures the view of the distal humerus articular surface, with the elbow in extension. To visualize the fracture line with the Morrey slide, the elbow must be flexed past 90 degrees.Also important, the distal fracture fragments typically rotate with the apex anteriorly, which is important to remember when reducing the joint surface.
PATHOGENESIS
The mechanism of injury is a direct impact of the semilunar notch or coronoid process of the olecranon. Either of these structures can wedge into the trochlea, causing a split in the condyles.This most frequently occurs with a fall of the flexed elbow.
NATURAL HISTORY
The natural history of this fracture without anatomic restoration is characterized by stiffness, varus malunion, and chronic elbow dysfunction.
PATIENT HISTORY AND PHYSICAL FINDINGS
Mechanism of injury is important to obtain, higher energy injuries suggest an increased risk for compartment syndromeA careful neurovascular examination should be performed, with particular attention to the median, ulnar, and radial nerves.The limb should be inspected for open wounds. High-energy T-condylar fractures are often open injuries.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Quality anteroposterior (AP) internal and external oblique views can be useful if the diagnosis is in question.Traction views can often be useful in fractures where shortening is present, although children and adolescents will often tolerate these poorly.Computed tomography (CT) can be useful, but the coronal and sagittal reconstructions must be rendered in the plane of the joint or perpendicular to it (normal AP and lateral planes); otherwise, the information obtained will be difficult to interpret.Coronal fragments may be missed if high-quality imaging is not obtained (see FIG 3A).
DIFFERENTIAL DIAGNOSIS
T-condylar fractures must be differentiated from other fractures of the distal humerus in children and adolescents because the treatment will differ.High-quality radiographs are generally sufficient to make this diagnosis.A CT or traction views can be helpful if the diagnosis is in question or if a coronal shear fragment is suspected on plain radiographs.
NONOPERATIVE MANAGEMENT
Initial management includes a well-padded splint following adequate physical examination.If the injury is open, an intravenous (IV) first-generation cephalosporin should be administered as soon as the injury is identified. If there is excessive contamination, comminution, or soft tissue injury, IV gentamicin is also recommended.There is limited value in nonsurgical management with the exception of patients with nonfunctional upper limbs at baseline.P.72
SURGICAL MANAGEMENT
Open injuries should be addressed surgically within 24 hours; closed injuries may be addressed semielectively.Attention is given to the distal radius; “floating elbows,” in which both the distal humerus and distal radius and/or ulna are affected, are not uncommon. These injuries should be identified early, as they are at increased risk for compartment syndrome.The soft tissue envelope is an important consideration. Fracture blisters (see FIG 3B) can be present, which can compromise the sterility and the closure of the procedure.The vast majority of T-condylar humerus fractures require operative treatment. In younger children, a percutaneous or mini-open approach may be possible.In older children and adolescents, an open posterior approach offers direct visualization and anatomic reduction and fixation of fracture fragments.
PREOPERATIVE PLANNING
High-quality AP and lateral radiographs are mandatory prior to surgery.Internal and external oblique views may be useful in identifying columnar comminution. CT scan can be useful in identifying coronal shear fragments.Method of fixation should be chosen by patient age, degree of displacement, and amount of comminution.Specialized distal humeral plating systems are available from several different manufacturers to allow either bicolumn or “90:90” plating.
POSITIONING
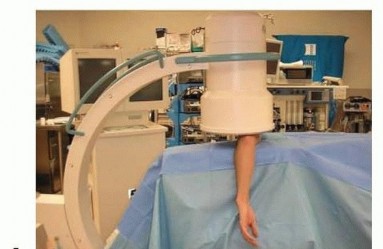

FIG 5 • A,B. Patient positioning for distal humerus fractures. (Courtesy of Samir Mehta, MD.) The contralateral arm is flexed at the shoulder and elbow to 90 degrees and placed on an arm board that is rotated so it is flush with the bed. This arm is then secured to the arm board.The operative arm is laid over a radiolucent arm board or paint roller so that the elbow is flexed 90 degrees (FIG 5).C-arm is brought in to assure that AP and lateral x-rays are adequate. The arm is then prepped and draped sterilely.A sterile tourniquet is used if one is desired.A “brain bag” is placed under the arm to be used to catch any blood or irrigant that comes from the field. The Bovie and suction are also placed in this bag for use.
APPROACH
As described in the following text. A posterior incision is used.
TECHNIQUES
EXPOSURE
MORREY SLIDE
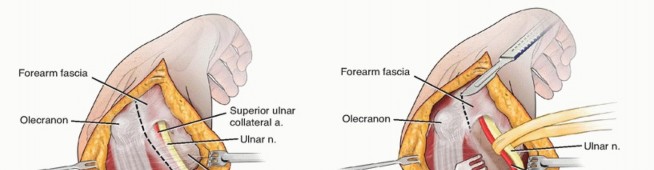
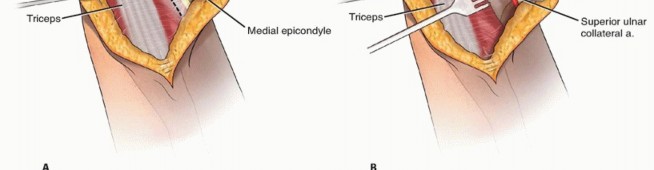
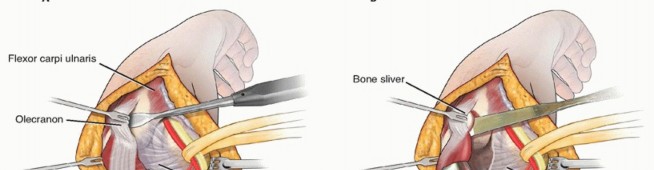
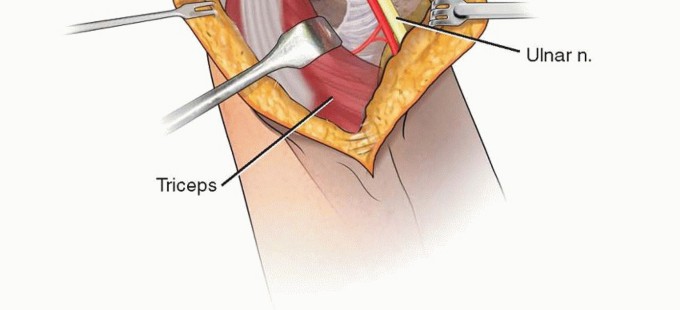
TECH FIG 1 • A. Superficial exposure. B. Elevation of the triceps off of the ulna. C. Medial periosteal flap being created. D. Morrey slide technique with bone wafer modification.(continued)


TECH FIG 1 •(continued)E. The tip of the olecranon can be resected if more joint visualization is required. Additionally, the anconeus can be subperiosteally reflected if access to the radial head is necessary in the case of a coronal capitellar split. (Adapted from Bryan RS, Morrey BF. Extensive posterior exposure of the elbow: a triceps-sparing approach. Clin Orthop Relat Res 1982;[166]:188-192.)
REDUCTION AND FIXATION
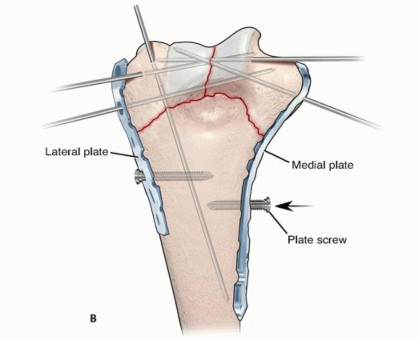
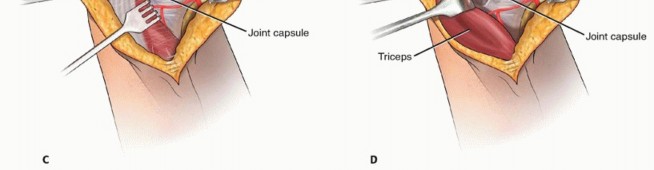
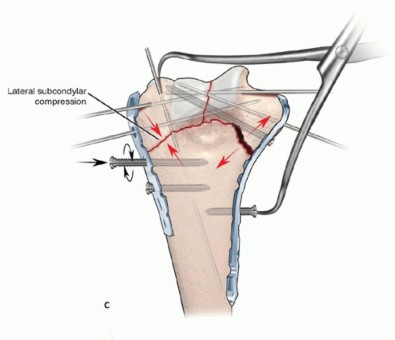
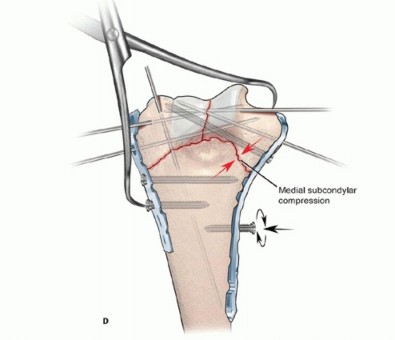
TECH FIG 2 • A. Fragments tend to be rotated anteriorly toward the midline. B. Plates are provisionally held on with Kirschner wires and shaft screws.(continued)
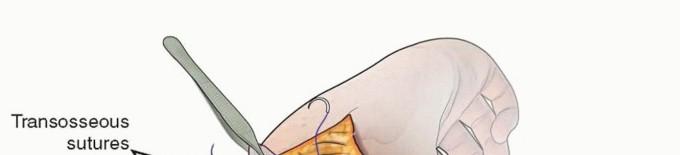

TECH FIG 3 • Transosseous sutures are used to repair the triceps to the olecranon. The defect in the fascia/periosteum unit is then repaired. (Adapted from Bryan RS, Morrey BF. Extensive posterior exposure of the elbow: a triceps-sparing approach. Clin Orthop Relat Res 1982;[166]:188-192.) The fascia/periosteum layer is carefully repaired to itself using heavy Vicryl suture. A 10F Jackson-Pratt drain is routinely placed.A subcutaneous loose closure of 2-0 Vicryl is then used.Last, the skin is closed with simple nylon stitches if the closure appears to be complex or if it is simple and loose, absorbable monofilament simple stitches may be placed, although the patient should be advised that they take several months to reabsorb and fall off.PEARLS AND PITFALLS
|Visualizing ▪ The C-arm should be brought in prior to draping to assure that adequate imaging the fracture can be obtained intraoperatively. A radiolucent arm board is quite helpful in this||regard.Preoperative ▪ A CT scan or traction x-rays can be helpful preoperatively to assess the degree planning of comminution or presence of coronal split fracture lines which could impedereduction at the time of surgery.Obtaining ▪ The articular block should be reconstructed first; in adolescents, there is the generally less comminution than in adults, so this block can generally bereduction reconstructed into one large fragment. After this fragment is reduced, the articular block can be reduced to the shaft segment.Preventing ▪ The goal of surgery is to provide a stable enough construct that immediate stiffness motion or, at the very least, motion within 3 weeks is possible. Often, adolescentsare nonadherent to self-therapy regimens, and frequent follow-up is necessary to prevent elbow stiffness or need for arthrolysis. Consider a continuous passive motion (CPM) postoperatively. Patients should be advised that usually 10 degrees of extension loss can be expected.Closure ▪ Closure with staples or nylon stitches is advised; remove every other day at 10-14 days. These will allow for wound care with early motion.Follow-up ▪ Follow-up once a week for 4-6 weeks for motion checks. Multiple x-rays are unnecessary, but monitoring the early motion is essential.|------P.78
POSTOPERATIVE CARE
A well-padded posterior splint in about 70 degrees of flexion is placed, and a sling applied.The patient is kept in house for 24 to 48 hours; the drain is pulled when less than 20 mL of drainage per shift is recorded.In open fractures, antibiotics are given for 48 hours. In closed fractures, antibiotics are stopped after 24 hours.Patients are sent home in a posterior splint which is removed five times a day for active and active-assisted range of motion (30 repetitions each session). They may also shower at this point.The patient is seen back in 2 weeks for a wound check.At 6 weeks, all immobilization is removed, and the patient is started on home low load prolonged stretching exercises and formal physical therapy.No gym or sports are allowed for 3 months or until the maximum range of motion (or full range of motion) has occurred and physical therapy has cleared the patient for activity.
OUTCOMES
Re et al6 reported a series of T-condylar humerus fractures in children and adolescents and reported that the Bernard Morrey approach resulted in significantly better motion than the more traditional triceps-splitting approach. This group also reported that early motion resulted in better final flexion and earlierfunctional range of motion than when range of motion was delayed.Beck et al1 reported on 26 children and adolescents who had T-condylar fractures who were operatively treated. Approximately, one-third had elbow stiffness at final follow-up. Early range of motion resulted in earlier return to motion.
COMPLICATIONS
Stiffness is quite common in T-condylar humerus fractures; preventing stiffness can be achieved by adequate stabilization to allow early motion.Symptomatic hardware is common; in adolescents, we do not routinely remove hardware unless the patient complains of it.Infection is more common in open injuries but still quite rare.Nerve injuries are generally neurapraxias and resolve spontaneously in 3 to 6 months.
REFERENCES
- Beck NA, Ganley TJ, McKay S, et al. T-condylar fractures of the distal humerus in children: does early motion affect final range of motion? J Child Orthop 2014;8:161-165.
- Bonczar MR, Rikli D, Ring D. Distal humerus 13-C1 Open reduction; perpendicular (biplanar) plating. AO Foundation Web site. Available at:http://bit.ly/1wEegQS. Published June 21, 2007. Accessed November 11, 2013.
- Bryan RS, Morrey BF. Extensive posterior exposure of the elbow. A triceps-sparing approach. Clin Orthop Relat Res 1982;(166):188-192.
- Green DP, Hotchkiss RN, Pederson WC; Dr. D. Sergeant Pepper Memorial Fund. Green's Operative Hand Surgery, ed 4. New York: Churchill Livingstone, 1999.
- Maylahn DJ, Fahey JJ. Fractures of the elbow in children: review of three hundred consecutive cases. J Am Med Assoc 1958;166:220-228.
- Re PR, Waters PM, Hresko T. T-condylar fractures of the distal humerus in children and adolescents. J Pediatr Orthop 1999;19:313-318.
