Open Reduction and Internal Fixation of Fractures of the Medial Epicondyle
DEFINITION
Trauma to the medial aspect of the elbow may cause a medial epicondyle fracture, which is an injury to the apophysis of the medial epicondyle.
ANATOMY
Medial epicondylar fractures involve the medial epicondylar apophysis on the posteromedial aspect of the elbow.The flexor-pronator muscle mass arises from this apophysis, including the palmaris longus, the flexor carpi ulnaris and radialis, the flexor digitorum superficialis, and one part of the pronator teres and the ulnar collateralligament ( FIG 1).3
PATHOGENESIS
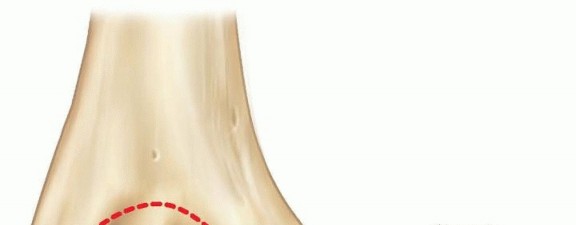
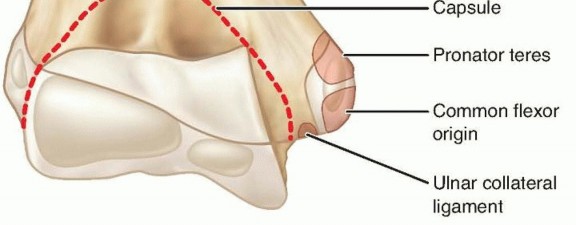
FIG 1 • Anatomic landmarks and site of muscle and ligament attachments on medial epicondyle.
NATURAL HISTORY
The outcome of medial epicondyle fractures is related to the amount of fracture displacement and also the demands placed on the elbow by the patient.Minimally displaced fractures treated nonoperatively generally do well, especially if the patient is not an athlete or if the fracture involves the patient's nondominant arm.Untreated displaced fractures may lead to chronic medial elbow instability and even recurrent elbow dislocations.Throwing athletes may have significant impairment in their sports activities. 9
PATIENT HISTORY AND PHYSICAL FINDINGS
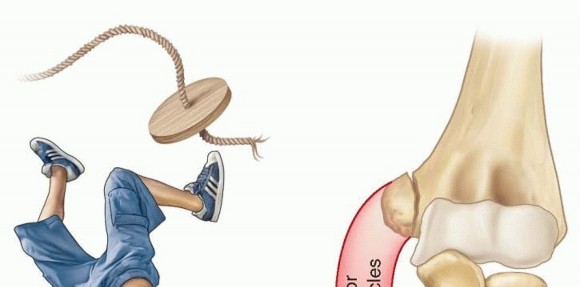
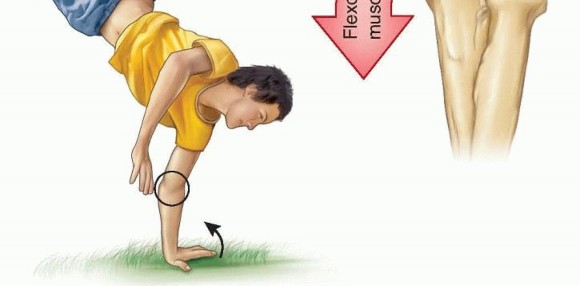
FIG 2 • A common mechanism of injury: a fall on an outstretched arm causing either a “pull-off” or a “push-off” avulsion of the medial epicondyle. P.58Assessment of medial elbow stability is often important in determining treatment.A positive valgus stress test confirms medial elbow instability. Persistence of medial elbow instability may cause significant elbow disability in athletes or those doing heavy labor.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Standard anteroposterior (AP) and lateral radiographs of the elbow are required, but oblique views are often helpful to visualize the medial epicondyle, which is on the posteromedial aspect of the distal humerus.Widening of the apophysis may be the only sign of injury, so comparison views of the unaffected elbow are often helpful to assess and determine subtle degrees of displacement.If there is radiographic absence of the medial epicondyle and suspected joint incarceration, an arthrogram, computed tomography (CT) scan, or magnetic resonance imaging (MRI) may occasionally be needed.
DIFFERENTIAL DIAGNOSIS
Medial condylar fracturesSupracondylar fractures Elbow dislocation
NONOPERATIVE MANAGEMENT
Smith in 1950 became a strong advocate of nonoperative management of this injury, pointing out that the fracture involved an apophysis rather than a physis and thus future growth was not compromised. He also documented that imperfect reduction or even nonunion was not automatically associated with a poor outcomein terms of elbow function and strength. 3A more recent study from Sweden where all patients were treated nonoperatively showed 96% good to excellent results. Over 60% of the patients had a fibrous union or nonunion. 3Two studies have compared nonoperative and operative treatment. Bede and associates 1 found that nonoperative treatment had better outcomes than operative treatment.Farsetti and coworkers 5 demonstrated similar results of nonoperative treatment and open reduction and internal fixation (ORIF) with Kirschner wires in displaced fractures.Indications for nonoperative management of medial epicondyle fractures include patients who do not place high physical demands on their elbows and most nondominant elbows.Nonoperative treatment encompasses splinting for 5 to 7 days or until acute soft tissue swelling resolves and then early active range of motion starting as soon as possible after the injury.Physical therapy may be required if range of motion is slow to return, but passive stretch may cause more injury and should be avoided.
SURGICAL MANAGEMENT

FIG 3 • Injury film. The medial epicondylar fragment is displaced and located in the joint.
PREOPERATIVE PLANNING
Careful review of radiographs is done to assess the elbow joint for reduction and to assess the amount of displacement of the medical epicondylar fracture ( FIG 3). Recent research indicates plain radiography mayunderestimate the actual displacement of medical epicondyle fractures based on imaging by CT scans. 4A complete assessment of neurovascular status of the upper extremity is performed, with particular attention to the ulnar nerve examination.A valgus stress test is performed to assess for medial elbow instability, typically under sedation or anesthesia.
POSITIONING

FIG 4 • Arm positioning and approach to the medial epicondyle, with the ulnar nerve course marked out. P.59
TECHNIQUES
Open Reduction and Internal Fixation with Cannulated Screw
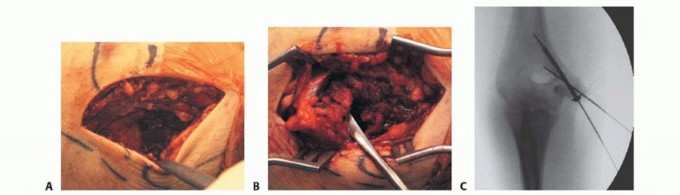
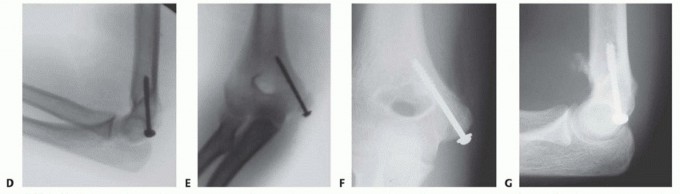
TECH FIG 1 • A. Incision with ulnar nerve identified. B. The fracture fragment is mobilized. C. Fluoroscopic image showing two pins spanning the fracture fragment for rotational stability. D,E. Cannulated screw fixation shown fluoroscopically. F,G. Radiographs showing healed fracture.
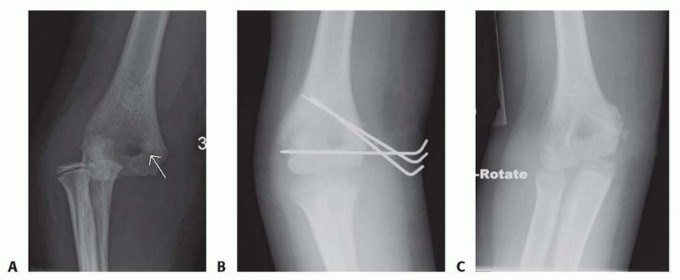
TECH FIG 2 • A. AP radiograph of an almost 8-year-old boy with an elbow fracture-dislocation and a displaced medial epicondyle fracture;arrowidentifies the fracture fragment. B. Because of the small size of the fragment, K-wire fixation was selected to stabilize the fracture fragment. C. Follow-up radiograph at 7 weeks postoperatively. (Courtesy of Felicity Fishman, MD.)This would involve sutures placed directly in the tendinous tissue and secured to the periosteum adjacent to the bed from which the epicondyle was avulsed.K-wires may be used as a means of fixation in the presence of comminution or if the epicondyle fragment is too small for a screw ( TECH FIG 2).2. Extraction of Medial Epicondyle from Elbow Joint: Roberts TechniqueA valgus stress is applied to the elbow with the forearm supinated. The wrist and fingers are dorsiflexed.As the position is reached, the fragment should be dislodged from the joint.This technique is most effective in the first 24 hours after the injury, before much muscle spasm occurs. 3Postoperative ▪ Medial epicondyle fracture fragment should be fixed with a cannulated screw ifstiffness possible rather than pins to have rigid fixation permitting early motion. Elbow motion is encouraged as soon as possible.Recognition1.The surgeon must beware of a medial epicondyle that is absent on radiography:It may be trapped in the joint.Loss ofextension1.The surgeon must document radiographically that the internal fixation is not inthe olecranon fossa, where it may block elbow extension.
PEARLS AND PITFALLS
POSTOPERATIVE CARE
Postoperative management after open reduction of medial epicondyle fractures depends on the type and stability of the fixation of the epicondylar fragment.For ORIF with screws, initial splinting for 3 to 5 days in about 50 to 60 degrees of flexion is recommended, followed by early active range of motion.Some authors recommend a removable brace preventing valgus stress but permitting full flexion and extension for 4 weeks. 2In one recent series on young athletes with this injury repaired with screw fixation, active range of motion out of the brace continued from weeks 5 to 8 postoperatively. At 8 weeks, noncontact sports were allowed, andreturn to full activity was possible at 12 weeks after surgery. 2P.61
OUTCOMES
Eight adolescent athletes undergoing ORIF with screw fixation for this fracture had excellent results with no residual valgus instability and full return to all sports. One patient had a loss of 5 degrees ofhyperextension, but all other patients had recovery of full range of motion. 2In another series, 21 of 23 patients treated operatively had recovery of full movement, whereas only 14 of 20 patients treated nonoperatively had full range of motion. 10A recent series of operative treatment and early motion in 25 patients with displaced fractures showed good to excellent results in all patients. 9Similarly, another study of competitive athletes found excellent results in 20 patients, 6 treated nonoperatively and 14 operatively. All overhead athletes were able to return to their sport. 7,8
COMPLICATIONS
Failure to diagnose joint entrapment of the medial epicondyle fracture Ulnar nerve dysfunctionLoss of range of motion NonunionMyositis ossificans
REFERENCES
- Bede WB, Lefebvre AR, Rosman MA. Fractures of the medial humeral epicondyle in children. Can J Surg 1975;18:137-142.
- Case SL, Hennrikus WL. Surgical treatment of displaced medial epicondyle fractures in adolescent athletes. Am J Sports Med 1997;25: 682-686.
- Chambers HG, Wilkins KE. Medial apophyseal fractures. In: Rockwood CA, Wilkins KE, Beaty JH, eds. Fractures in Children, ed 6. Philadelphia: Lippincott-Raven, 1996:800-819.
- Edmonds EW. How displaced are “nondisplaced” fractures of the medial humeral epicondyle in children? Results of a three-dimensional computed tomography analysis. J Bone Joint Surg Am 2010;92(17):2785-2791.
- Farsetti P, Potenza V, Caterini R, et al. Long-term results of treatment of fractures of the medial humeral epicondyle in children. J Bone Joint Surg Am 2001;83-A(9):1299-1305.
- Glotzbecker MP, Shore B, Matheney T, et al. Alternative technique for open reduction and fixation of displaced pediatric medial epicondyle fractures. J Child Orthop 2012;6:105-109.
- Gottschalk HP, Eisner E, Hosalkar, HS. Medial epicondyle fractures in the pediatric population. J Am Acad Orthop Surg 2012;20:223-232.
- Lawrence JT, Patel NM, Macknin MD, et al. Return to competitive sports after medial epicondyle fractures in adolescent athletes. Am J Sports Med 2013;41:1152-1157.
- Lee HH, Shen HC, Chang JH, et al. Operative treatment of displaced medial epicondyle fractures in children and adolescents. J Shoulder Elbow Surg 2005;14:178-185.
- Wilson NI, Ingram R, Rymaszewski L, et al. Treatment of fractures of the medial epicondyle of the humerus. Injury 1988;19:342-344.
