Open Reduction and Internal Fixation of Fracture-Dislocations of the Elbow with Complex Instability
DEFINITION
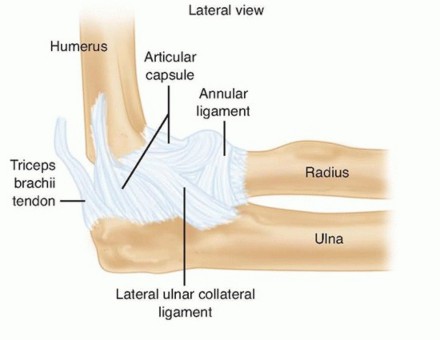
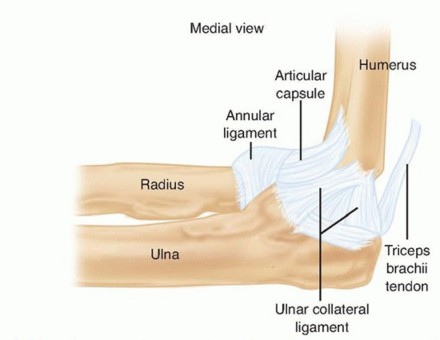
FIG 1 • The MCL and LCL complexes of the elbow. Note their points of attachment on the distal humerus and proximal ulna. The principle of treating fracture-dislocations of the elbow is to provide sufficient stability through reconstruction of bony and ligamentous restraints such that early motion (within 2 weeks postoperatively) can be instituted without recurrent instability.Failure to achieve this will result in either recurrent instability or severe stiffness after prolonged immobilization.
ANATOMY
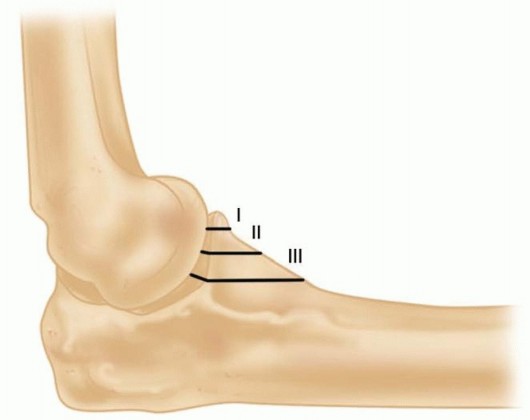
FIG 2 • Lateral view of the elbow depicting the different types of coronoid fractures.
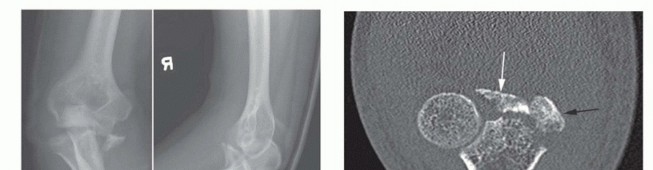
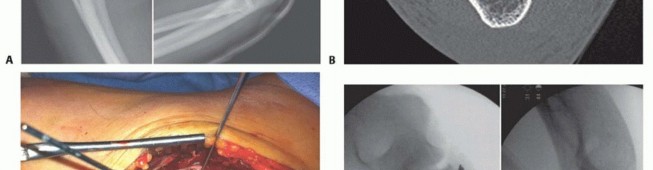
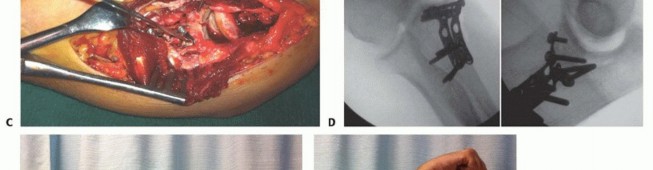

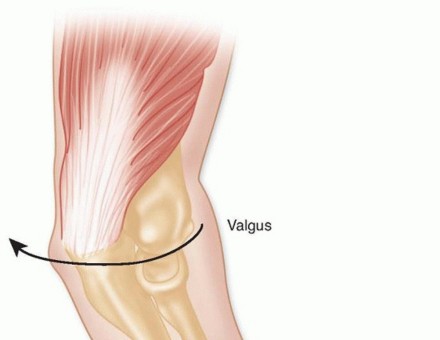
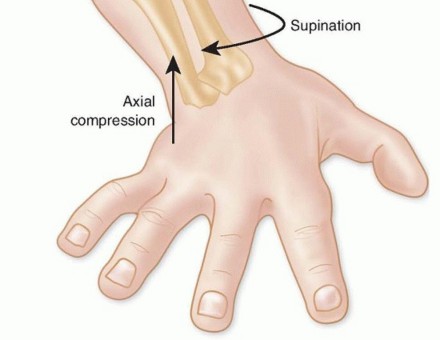
FIG 4 • Typical mechanism of elbow fracture-dislocation. Note the forces at play on the elbow.
PATHOGENESIS
Fracture-dislocations of the elbow occur during falls onto an outstretched hand, falls from a height, motor vehicle accidents, or other high-energy trauma ( FIG 4).Typically, there is a hyperextension and valgus or varus stress applied to the pronated arm.
NATURAL HISTORY
Elbow dislocations with associated coronoid or radial head fractures have a poor natural history. These injuries are commonly treated with open reduction and surgical fixation, as redislocation or subluxation is likely with closed treatment.Treatment of the radial head fracture by excision alone in the context of an elbow dislocation has a high rate of failure due to recurrent instability and should be avoided.Problems of recurrent instability, arthrosis, and severe stiffness lead to poor functional results. 12
PATIENT HISTORY AND PHYSICAL FINDINGS
Fracture-dislocations of the elbow are acute and traumatic, so the history should be straightforward.It is not unusual for these injuries to occur with high-energy trauma, so a diligent search for other musculoskeletal and systemic injuries must accompany evaluation of the elbow. The ipsilateral shoulder and wrist should be evaluated.The evaluation and documentation of peripheral nerve and vascular function in the injured extremity is critical and should be performed before and after reduction maneuvers.
IMAGING AND OTHER DIAGNOSTIC STUDIES
High-quality plain radiographs in the anteroposterior (AP) and lateral plane should be obtained before and after closed reduction.Cast material can obscure bony detail after closed reduction.If there is any evidence of forearm or wrist pain associated with the elbow injury, these should be imaged as well.Computed tomography (CT) scans with reformatted images and three-dimensional (3-D) reconstructions are helpful in understanding the configuration of bony injuries (especially of the radial head and coronoid) and are helpful in treatment planning ( FIG 5).
DIFFERENTIAL DIAGNOSIS
Radial head or neck fractures without associated dislocationCoronoid fracture associated with posteromedial instability. The radial head is not fractured, making diagnosis more difficult.
NONOPERATIVE MANAGEMENT
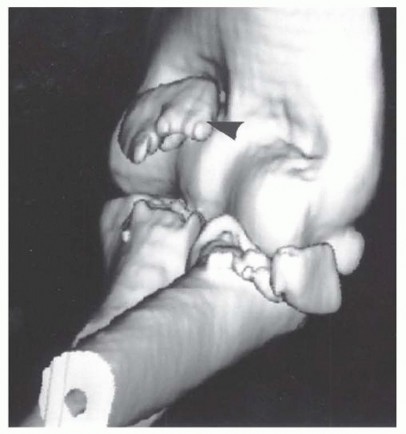
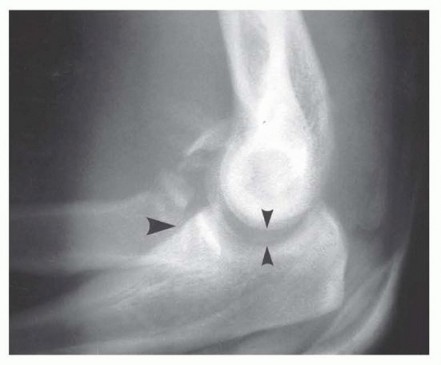
FIG 6 • Radiograph revealing nonconcentric reduction after closed reduction. Thesmall arrowshighlight the nonconcentric reduction of the ulnohumeral joint. (From Pugh DM, Wild LM, Schemitsch EH, et al. Standard surgical protocol to treat elbow dislocations with radial head and coronoid fractures. J Bone Joint Surg Am 2004;86A:1122-1130.)
SURGICAL MANAGEMENT
The goals of surgery are to obtain and maintain a concentric and stable reduction of the ulnohumeral and radiocapitellar joint such that early motion within a flexion-extension arc of 30 to 130 degrees can be initiated. Early motion is key (within 2 weeks postoperatively) to avoid elbow stiffness and resultant poor function.Management of elbow dislocations with associated radial head and coronoid fractures should follow an established protocol ( Table 1) that has produced reliable results.10The radial head is an important secondary stabilizer of the elbow to valgus stress and posterior instability. 9It is also a longitudinal stabilizer of the forearm to proximal translation.If fractured in this setting, it must be fixed or replaced, as radial head excision leads to recurrent instability and unacceptable results. 12
PREOPERATIVE PLANNING
Before surgery, the surgeon must ensure that the proper equipment and implants are available.Coronoid tip fractures are fixed with small fragment or cannulated screws of appropriate size. In the setting of small fragments (ie, type 1) that are not amendable to screw fixation, sutures through the anterior capsule around the fragment can be used instead. Large coronoid fragments such as anteromedial facet fragments should be fixed with a minifragment plate and screws in buttress fashion. Table 1 Treatment Protocol for Elbow Dislocation with Associated Radial Head and Coronoid Fractures
STEP ACTION
1
Fix the coronoid fracture.
2
Fix or replace the radial head.
3
Repair the LCL.
4
Assess elbow stability within 30-130 degrees of flexion-extension with the forearm in fullpronation.
5
If the elbow remains unstable, consider fixing the MCL.
6
Failing this, apply a hinged external fixator to maintain concentric reduction and allow forearly motion.Radial head and neck fracture fixation is accomplished with screws alone or small fragment plates and screws. We often use countersunk Herbert screws or countersunk minifragment screws to fix articular head fragments.If the radial head fragment is comminuted with more than three fragments, the surgeon must be prepared for radial head replacement. A metallic, modular radial head implant system should be available if primaryosteosynthesis cannot be achieved.An image intensifier is helpful during surgery. Films confirming concentric reduction and the proper positioning of implanted hardware should always be obtained before leaving the operating room.In rare instances in which bony and ligamentous repair fails to restore sufficient elbow stability, dynamic hinged external fixation is used.This is a highly specialized technique that may not be appropriate for all surgeons.In the event that a dynamic fixator is not an option, a static external fixation should be applied and patient must be referred to an upper extremity surgeon for further management.
POSITIONING
Most commonly, the patient is positioned supine on the operating table under general anesthesia.The operative limb is supported on a hand table, and a tourniquet is applied to the upper arm before preparation and draping ( FIG 7).Alternatively, the lateral decubitus position can be used with the operative limb supported by a padded bolster.This position is used if hinged fixation is deemed likely.A posterior skin incision can also be used in this position, with creation of full-thickness flaps to access both medial and lateral sides.
APPROACH


FIG 7 • Patient positioned supine with hand table.


TECHNIQUES
LATERAL EXPOSURE


TECH FIG 1 • Lateral approach. In this case, the radial neck was fractured and the head has been removed. An excellent view of the coronoid is achieved. Here, a type I coronoid fracture is present.
Open Reduction and Internal Fixation of Coronoid Fracture
Open Reduction and Internal Fixation of Coronoid Fracture
TYPE I CORONOID FRACTURES

TECH FIG 2 • Suture fixation of a type I coronoid fracture. The suture is passed through the anterior capsule above the coronoid. Its ends will be passed through the proximal ulna and tied over the dorsal surface. This type of fixation is used if the coronoid fragment is too small to accept a screw. (From McKee MD, Pugh DM, Wild LM, et al. Standard surgical protocol to treat elbow dislocation with radial head and coronoid fractures. J Bone Joint Surg Am 2005;87[suppl 1, pt 1]:22-32.) The suture ends can be retrieved through the drill holes using an eyeleted Kirschner wire, a Keith needle, or a suture retriever. Types II and III Coronoid Fractures



TECH FIG 3 • Coronoid fracture held reduced with Kirschner wire. (From McKee MD, Pugh DM, Wild LM, et al. Standard surgical protocol to treat elbow dislocation with radial head and coronoid fractures. J Bone Joint Surg Am 2005;87[suppl 1, pt1]:22-32.) Coronoid fractures that are comminuted may be difficult to treat. Typically, the largest fragment with articular cartilage is fixed.If screw fixation is not possible or access is difficult due to an intact radial head, the coronoid can be accessed through a medial approach, as described in the following text. Medial Approach for Coronoid Fracture
FIXATION
The medial approach can also be used in situations where surgical fixation of type II or type III coronoid is not possible due to an intact radial head.The medial approach can be used for surgical fixation of anteromedial facet fractures of the coronoid.These fractures should be surgically fixed via a medial approach, by use of plate and screws. The plate is placed along the anterior aspect of the coronoid, buttressing the fragments from displacement.The medial approach is outlined in the following text.A medial incision along the supracondylar ridge is used. The ulnar nerve is identified and protected.The common flexor origin is split to gain access to the coronoid on the proximal ulna.From the medial side, a minifragment plate can be used in a buttress or spring fashion to secure a comminuted fracture.2. Radial Head or Neck FractureRadial head fracture is addressed after treatment of the coronoid injury because once the head is fixed or replaced, access to the coronoid from the lateral approach is limited.The decision to fix a radial head is largely based on the fracture configuration. If fracture comminution islimited such that the head is in two or three fragments, reduction and fixation is usually possible.Fractures that are comminuted (with more than three fracture fragments) or with articular surface damage require replacement.Expose the head and neck as necessary for fracture reduction and fixation by extending the Kocher interval.P.201The posterior interosseous nerve is at risk during more distal radial neck exposures. Its distance from the operative site can be maximized by keeping the forearm in full pronation. If fixation extending down the radial neck is planned, it is prudent to expose the posterior interosseous nerve and protect it. Open Reduction and Internal Fixation of Radial Head Fractures For radial head fragments, reduce and hold the fragment to the intact head with a pointed reduction clamp.We secure the fragments with Herbert screws. The fragments can be held temporarily with a 2-mm Kirschner wire and then replaced with a Herbert screw. Similar countersunk minifragment screws may be used or headless differential pitch compression screws.If the screw is inserted through articular cartilage, its head must be countersunk. Radial neck fractures, once reduced, can be held provisionally with a Kirschner wire. Definitive fixation is with a small fragment T-plate over the “safe zone” ( TECH FIG 4).Care is taken to not injure the posterior interosseous nerve while exposing the shaft or by trapping it under the plate distally.If the radial head cannot be reconstructed, it should be replaced (see in the following text).
RADIAL HEAD REPLACEMENT
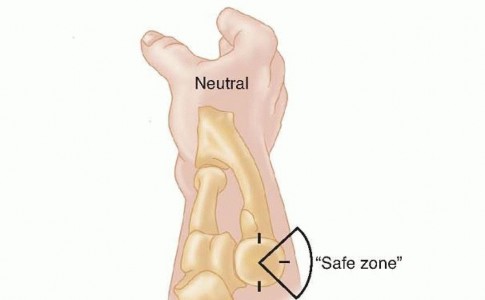
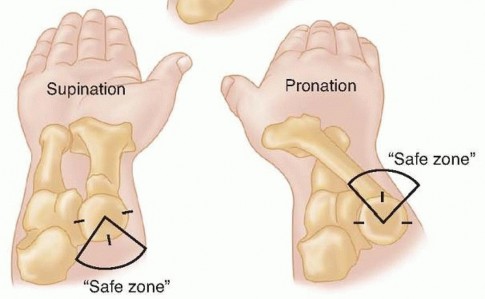
TECH FIG 4 • The safe zone for plating radial neck fractures. The 90-degree arc outlined does not articulate with the proximal ulna throughout the full range of forearm rotation. Plating a radial neck fracture in this zone will not interfere with rotation.


TECH FIG 5 • Radial head implant. An appropriately sized radial head implant has been inserted. It is held reduced with the forearm in full pronation. Note the anatomic alignment with the capitellum.


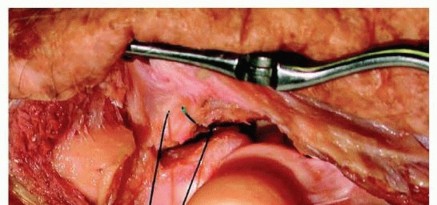
TECH FIG 6 • A. Elbow instability associated with deficient LCL. Without repair of the LCL, the radial head subluxes into a posterolateral position with forearm supination. Note that the radial head and capitellum are no longer in normal alignment. B. The LCL is held by the forceps. It is a distinct structure easily identified in this acutely injured elbow. C. Sutures passed for LCL repair. Using a drill, Kirschner wire, or pointed towel clip, make holes in the distal lateral humerus above the epicondyle.Pass the suture through the holes and into the lateral ligament such that it will tighten on tying the sutures.At least two, preferably three, sutures through bone are required. Pass, cut, and snap all of the sutures ( TECH FIG 6C).Ensure that the elbow is now held in 90 degrees of flexion and full forearm pronation. Incorporate the more superficial common extensor origin in the repair.Tie the sutures once they have all been passed and then close the lateral wound in layers.2. Persistent InstabilityOn occasion, repair of the coronoid, radial head, and LCL from the lateral approach is insufficient to restore elbow stability such that early motion may be initiated.In these cases, further efforts must be made to obtain such stability.Repair of the MCL through a separate medial incision is one option if a lateral approach has been used for coronoid and radial head fracture fixation.A deep approach to the medial aspect of the elbow puts the ulnar nerve at risk, and it must be identified and protected during the procedure.Usually, the MCL is torn in its midsubstance. Suture repair of this is often unsatisfying. Using a graft to replace the MCL is not recommended in the acute injury setting.If elbow stability remains insufficient, applying a hinged fixator is the final option. 6If the hinge is not available or the surgeon is not familiar with its use, a static fixator can be applied to maintain elbow reduction.
HINGED EXTERNAL FIXATION
The application of a hinged external fixator is not as commonly required now that the primary structures for elbow stability, and their repair, are more thoroughly understood.Application of the hinged fixator starts with the insertion of a guide pin through the center of elbow rotation.Insert the pin from medial to lateral starting at the medial epicondyle through a small incision and protect the ulnar nerve. The pin should be directed through the center of the capitellum.Insert two half-pins in the humerus above the elbow through small open incisions over the posterior surface by bluntly spreading the triceps fibers.Insert two half-pins in the ulna over its subcutaneous border dorsally.After pin insertion, the elbow is held reduced while the frame is assembled around it.The hinge slides over the guide pin on either side of the elbow. Three-quarter rings are attached proximal and distal to the elbow.Attach the pins to the rings and tighten all parts of the hinged fixator.Verify that the elbow remains reduced in the frame through 30 to 130 degrees of motion. The forearm is maintained in pronation to protect the lateral ligament repair.Lock the elbow at 90 degrees in the hinge for the initial postoperative course.Obtain plain radiographs in the operating room before the conclusion of the procedure.P.203
POSTOPERATIVE CARE
The injured elbow is placed in a well-padded plaster splint at 90 degrees of flexion and full pronation. The
PEARLS AND PITFALLS
Indications1.Elbow dislocations with associated fractures of the coronoid or radial headmust be recognized as complex dislocations. They usually require surgical treatment.Goals oftreatment1.The goals are to obtain a concentric reduction with sufficient elbow stabilitysuch that early range of motion is possible and to avoid persistent instability, elbow stiffness, and arthritis.Coronoidfractures1.Repair of coronoid fractures is technically demanding but necessary forsuccessful treatment.Radial head1.The surgeon should be prepared to replace the radial head if necessary with ametal, modular prosthesis. ▪ Excision alone is not an option.Lateralligaments1.Repair of the lateral ligaments is important to impart the necessary stability forearly motion and to avoid late posterolateral rotatory instability.Physiotherapy ▪ It is important to emphasize to the patient the need to be diligent withrehabilitation and exercises, as this will have a great effect on the end result.1.Immobilization beyond 2 weeks should be avoided.patient is given a sling for comfort.AP and lateral radiographs are obtained in the operating room to ensure congruent reduction and verify hardware placement.The patient may be discharged home on the same day after receiving adequate analgesia and prophylactic antibiotics.We do not routinely give prophylaxis for heterotopic ossification unless the patient has a concomitant head injury: In this case, indomethacin 25 mg three times a day is prescribed with a cytoprotective agent for 3 weeks.The patient returns to our clinic at 7 to 10 days postoperatively for staple removal. The splint is typically removed at this point.Range-of-motion exercises are initiated at this time under the supervision of a physiotherapist.Active and active-assisted flexion-extension between 30 and 130 degrees and forearm rotation with the elbow at 90 degrees of flexion is initiated.A lightweight resting splint is made for the injured elbow that is removed for hygiene and physiotherapy.The patient returns at 4, 8, and 12 weeks after surgery for clinical review with plain radiographs. Thereafter, the interval of clinic visits is widened, but we follow our patients out to 2 years.At 4 weeks, we allow unrestricted range of motion and at 8 weeks, unrestricted strengthening. Evidence of fracture union is usually present between 6 and 8 weeks.Progress with range of motion can be slow and frustrating for the patient but does not plateau until 1 year of follow-up.
OUTCOMES
Following the protocol outlined for fracture-dislocations of the elbow should yield satisfactory functional results.Pugh et al 10 reported the results of this treatment protocol for 36 elbows at 34 months.The flexion-extension arc averaged 112 degrees and rotation 136 degrees.Fifteen patients had excellent results, 13 good, 7 fair, and 1 poor as measured by the Mayo Elbow Performance Score.Eight patients had a complication requiring reoperation.
COMPLICATIONS
The most likely complication after treatment is unacceptable elbow stiffness with a resultant nonfunctional range of motion.An acceptable range is 30 to 130 degrees of flexion.At about 1 year after surgery, once motion has plateaued, patients are candidates for release with hardware removal if they are not happy with their range of motion and the flexion-extension arc is less than 100 degrees.This is done through the lateral approach with an anterior and posterior capsulectomy plus manipulation under anesthesia.A radial head implant in place can be downsized to improve motion, but it should not be simply removed. The lateral ligament complex is preserved.In our series, this was necessary in 11% of cases. 10Synostosis around the elbow is another possible cause of rotational forearm stiffness.A resection can be planned to improve motion.CT scanning preoperatively helps to define the extent of the lesion. Resection is technically demanding.Superficial and deep wound infection is possible after repair. Immediate and aggressive treatment is recommended with antibiotics initially and irrigation with débridement if rapid improvement is not seen.Persistent instability is rare but may occur despite best efforts at repair. Formal ligament reconstruction can be helpful in this setting.Posttraumatic arthritis may be a long-term problem.
REFERENCES
- Cage DJ, Abrams RA, Callahan JJ, et al. Soft tissue attachments of the ulnar coronoid process. An anatomic study with radiographic correlation. Clin Orthop Relat Res 1995;(320):154-158.
- Doornberg JN, Linzel DS, Zurakowski D, et al. Reference points for radial head prosthesis size. J Hand Surg 2006;31(1):53-57.
- Doornberg JN, Ring DC. Fracture of the anteromedial facet of the coronoid process. J Bone Joint Surg Am 2006;88(10):2216-2224.P.204
- Frank SG, Grewal R, Johnson J, et al. Determination of correct implant size in radial head arthroplasty to avoid overlengthening. J Bone Joint Surg Am 2009;91:1738-1746.
- Mason ML. Some observations on fractures of the head of the radius with a review of one hundred cases. Br J Surg 1954;42:123-132.
- McKee MD, Bowden SH, King GJ, et al. Management of recurrent, complex instability of the elbow with a hinged external fixator. J Bone Joint Surg Br 1998;80(6):1031-1036.
- McKee MD, Schemitsch EH, Sala MJ, et al. The pathoanatomy of lateral ligamentous disruption in complex elbow instability. J Shoulder Elbow Surg 2003;12:391-396.
- Moro JK, Werier J, MacDermid JC, et al. Arthroplasty with a metal radial head for unreconstructable fractures of the radial head. J Bone Joint Surg Am 2001;83-A(8):1201-1211.
- Morrey BF, Tanaka S, An KN. Valgus stability of the elbow. A definition of primary and secondaryconstraints. Clin Orthop Relat Res 1991;(265):187-195.
- Pugh DM, Wild LM, Schemitsch EH, et al. Standard surgical protocol to treat elbow dislocations with radial head and coronoid fractures. J Bone Joint Surg Am 2004;86A:1122-1130.
- Regan W, Morrey B. Fractures of the coronoid process of the ulna. J Bone Joint Surg Am 1989;71:1248-1254.
- Ring D, Jupiter JB, Zilberfarb J. Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84-A(4):547-551.
