INTRODUCTION AND BIOMECHANICAL PRINCIPLES
Tibial plateau fractures represent a complex spectrum of intraarticular injuries that challenge the orthopedic surgeon to restore joint congruity, axial alignment, and mechanical stability while meticulously preserving the surrounding soft tissue envelope. The proximal tibia is critical for load transmission across the knee joint. Biomechanically, the medial plateau is concave, highly dense, and bears approximately 60% of the physiological load during the normal gait cycle. Conversely, the lateral plateau is convex, sits slightly higher, and is structurally less robust, making it significantly more susceptible to depression and split-depression fractures under axial and valgus loading.
The primary goals of Open Reduction and Internal Fixation (ORIF) of the tibial plateau are the anatomical restoration of the articular surface, the establishment of absolute stability for early range of motion, and the prevention of posttraumatic osteoarthritis. Modern osteosynthesis emphasizes a biological approach: minimizing periosteal stripping, utilizing indirect reduction techniques where feasible, and applying anatomically precontoured locking plates to provide rigid subchondral buttressing.
💡 Clinical Pearl: Soft Tissue Assessment
The timing of definitive ORIF is dictated entirely by the soft tissue envelope. In high-energy injuries, the "span, scan, and plan" protocol—utilizing a temporary joint-spanning external fixator and delayed definitive fixation (typically 7 to 14 days)—is mandatory to allow for the resolution of fracture blisters and the return of skin wrinkles.
PREOPERATIVE PLANNING AND IMAGING
Standard orthogonal radiographs (anteroposterior, lateral, and oblique views) are essential for initial evaluation. However, a preoperative computed tomography (CT) scan with 2D and 3D reconstructions is the gold standard and is mandatory for surgical planning. CT imaging precisely delineates the degree of articular depression, the presence of coronal shear fragments (particularly the posteromedial fragment), and the exact location of the fracture apex, which dictates the optimal placement of buttress plates.
SURGICAL APPROACHES TO THE TIBIAL PLATEAU
The Anterolateral Approach (Lateral Condyle)
For fractures of the lateral condyle (Schatzker Types I, II, and III), the anterolateral approach provides excellent exposure of the lateral articular surface and metaphysis.
- Positioning: Place the patient supine on a radiolucent operating table. A bump may be placed under the ipsilateral hip to correct natural external rotation. Apply a pneumatic tourniquet proximally, inflating it only after exsanguination, except in patients with severe soft tissue compromise or vascular injury.
- Incision: Make a straight or slightly curvilinear anterolateral incision. Begin 3 to 5 cm proximal to the joint line and extend distally below the inferior margin of the fracture site, coursing from just anterior to the lateral femoral epicondyle down to Gerdy’s tubercle. This trajectory avoids crossing the tibial crest, thereby minimizing wound dehiscence complications. Alternatively, a classic L-shaped incision may be utilized.
- Deep Dissection: Incise the fascia in line with the skin incision. Meticulously avoid undermining the soft tissue flaps to preserve the subdermal vascular plexus.
- Meniscal Management: To gain intraarticular exposure, perform a submeniscal arthrotomy. Incise the coronary (inframeniscotibial) ligament. Place nonabsorbable tagging sutures (e.g., No. 1 Ethibond) into the meniscocapsular junction and retract the meniscus superiorly.
⚠️ Surgical Warning: Meniscal Preservation
Never excise a torn or entrapped meniscus simply to improve visualization. Inspect and meticulously debride or repair any meniscal tears. Preserving the meniscus is paramount to distributing tibiofemoral contact stresses and preventing rapid-onset arthrosis.
The Posterolateral Approach
The standard anterolateral approach offers limited visualization of the posterior aspect of the lateral plateau. For isolated posterolateral shear fractures, a more extensile approach is required.
1. Extend the fascial incision along the insertion of the extensor musculature, continuing over the subcapital fibula.
2. Identify and meticulously protect the common peroneal nerve.
3. Perform a fibular neck osteotomy using an oscillating saw. This permits the superior retraction of the fibular head (along with the attached lateral collateral ligament and biceps femoris), granting direct access to the posterolateral plateau and the posterior tibial flare.
STEP-BY-STEP SURGICAL TECHNIQUE: REDUCTION AND FIXATION
Articular Elevation and Bone Grafting
Exposing the depressed articular fragments requires careful manipulation of the metaphyseal bone.
- Fracture Exposure: For longitudinal split-depression fractures, elevate the origin of the extensor muscles from the anterolateral condyle extraperiosteally. Retract the lateral split fragment outward (hinging it open like a book) to expose the central articular depression. Alternatively, create a small cortical window distal to the depression to preserve the lateral wall's integrity.
- Elevation: Insert a curved bone tamp or periosteal elevator through the cortical window or fracture line, positioning it deep to the depressed subchondral bone.
- Reduction: Apply slow, meticulous, and directed upward pressure to elevate the articular fragments and the compressed cancellous bone en masse to the level of the native joint line.
- Defect Augmentation: Elevation creates a significant metaphyseal void. This cavity must be densely packed with a structural bone graft or substitute to prevent postoperative subsidence. While autogenous iliac crest bone graft remains a viable option, injectable calcium phosphate or calcium sulfate bone cements are highly preferred. Calcium phosphate offers superior immediate compressive strength, acting as an internal structural buttress.
Definitive Osteosynthesis
- Temporary Fixation: Once the articular surface is anatomically reduced (verified via direct visualization and fluoroscopy), secure the fragments temporarily with multiple 1.6-mm or 2.0-mm Kirschner wires.
- Subchondral Rafting: Place multiple 3.5-mm or 4.0-mm fully threaded screws in a "raft" configuration immediately distal to the subchondral bone to support the elevated articular segments.
- Plate Application: Apply a precontoured periarticular locking or non-locking plate to the anterolateral tibia. For simple lateral condylar fractures (Schatzker I & II) in young patients with good bone stock, a 3.5-mm non-locking buttress construct is often sufficient. In osteoporotic bone, locking technology is mandatory.
- Closure: Reattach the meniscus to the coronary ligament using the previously placed tagging sutures. If the iliotibial band was reflected from Gerdy's tubercle, repair it securely with heavy nonabsorbable sutures.
MEDIAL CONDYLE AND POSTEROMEDIAL APPROACH
Fractures of the medial tibial plateau (Schatzker IV) are high-energy injuries often involving a coronal shear component. These require a distinct surgical strategy, as anteromedial plating provides insufficient biomechanical support for posteromedial fragments.

- Incision: Mark the skin incision with indelible ink just posterior and parallel to the posteromedial border of the tibia.
- Dissection: Divide the skin and subcutaneous tissues sharply. Mobilize the inferior border of the pes anserinus anteriorly and retract the medial head of the gastrocnemius posteriorly.
- Plate Positioning: The fundamental goal is to create a stable buttress construct. The plate must be positioned directly over the apex of the fracture distally to counteract the vertical shear forces.
- Fixation: Apply a precontoured posteromedial buttress plate (often an under-contoured 3.5-mm T-plate or specific posteromedial locking plate). Secure the proximal segment with cancellous or unicortical locking screws to avoid penetrating the joint or interfering with lateral-sided hardware, and use standard cortical screws distally.

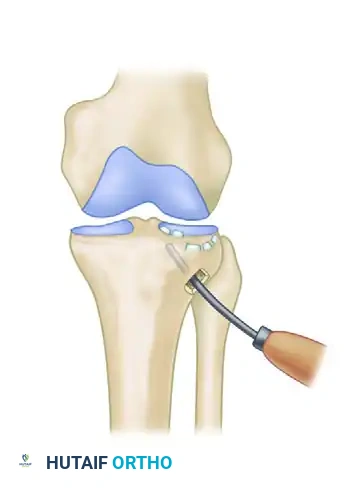
ARTHROSCOPICALLY ASSISTED REDUCTION AND INTERNAL FIXATION (ARIF)
Arthroscopically assisted techniques are increasingly utilized for Schatzker I, II, and III fractures. ARIF minimizes soft tissue morbidity, provides unparalleled illumination and magnification of the articular surface, and allows for the concurrent management of intraarticular pathology.
ARIF Technique
- Place the extremity in a thigh holder and establish standard arthroscopic portals (typically an anterolateral portal placed slightly higher, approximately 2 cm above the joint line).
- Evacuate the hemarthrosis through thorough lavage.
- Fluid Management: Use a dry arthroscopic technique or gravity flow without a high-pressure pump. Extravasation of fluid through the metaphyseal fracture lines into the calf compartments carries a severe risk of iatrogenic compartment syndrome.
- Manage any meniscal entrapment using an arthroscopic probe, lifting the meniscus out of the fracture cleft.
- Elevate the depressed fragments through a percutaneous metaphyseal window using a cannulated impactor guided by an ACL tibial drill guide.
- Confirm anatomical reduction arthroscopically and secure the construct with percutaneously placed 3.5-mm subchondral screws or a minimally invasive plate osteosynthesis (MIPO) technique.
💡 Clinical Pearl: ARIF Limitations
While ARIF is excellent for joint visualization, it is less suitable for severely comminuted bicondylar fractures or highly osteoporotic bone where extensive buttress plating and direct metaphyseal void filling are required.
MANAGEMENT OF CONCOMITANT LIGAMENTOUS INJURIES
Tibial plateau fractures are frequently associated with significant soft tissue disruptions. Ligamentous injuries occur in 4% to 33% of all plateau fractures, and the incidence skyrockets to 60% in fracture-dislocations. Unrecognized ligamentous laxity is a primary driver of poor long-term functional outcomes and accelerated posttraumatic arthritis, even in the presence of a perfectly healed fracture.
Incidence and Diagnosis
- Medial Collateral Ligament (MCL): The most commonly injured ligament, typically associated with local depression or split fractures of the lateral condyle (Schatzker II) due to the valgus deforming force.
- Meniscal Tears: Present in approximately 20% of cases, most frequently associated with medial plateau injuries (Schatzker IV).
- Cruciate Ligaments: Anterior Cruciate Ligament (ACL) injuries occur in roughly 10% of cases.
- Diagnosis: Preoperative MRI is highly sensitive but often impractical in the acute trauma setting. Intraoperative stress examination under anesthesia (EUA) following rigid fracture fixation is mandatory. Residual joint laxity after anatomical bony reduction confirms a concomitant ligamentous injury.
Treatment Algorithms for Ligamentous Trauma
- Tibial Eminence Avulsions: If the intercondylar eminence is fractured and displaced, it must be anatomically reduced and secured during the ORIF procedure. Fixation is achieved using heavy nonabsorbable sutures passed through transosseous tibial tunnels or a small-fragment cannulated screw if the bone fragment is sufficiently large.
- MCL Tears: Acute midsubstance tears of the MCL generally heal well with nonoperative management (hinged knee bracing). Acute surgical repair of the MCL is rarely indicated, as the extensive surgical exposure required significantly increases the risk of postoperative arthrofibrosis and knee stiffness.
- ACL Tears: Midsubstance ACL ruptures are typically managed nonoperatively in the acute setting. Delayed arthroscopic reconstruction is performed only if symptomatic instability persists after complete fracture consolidation and rehabilitation.
COMMINUTED BICONDYLAR FRACTURES (SCHATZKER V & VI)
Bicondylar fractures represent the most severe end of the spectrum. Historically, extensive single-incision exposures (e.g., the Mercedes-Benz incision) with massive dual plating led to catastrophic wound necrosis and deep infection rates exceeding 30%.
Modern management dictates a tissue-preserving approach:
1. Staged Protocol: Immediate spanning external fixation followed by delayed ORIF.
2. Dual Incision Technique: Utilizing separate anterolateral and posteromedial incisions with a wide skin bridge (minimum 7 cm) to preserve vascularity.
3. Fixation Strategy: The more comminuted condyle (often the medial side) is rigidly fixed with a buttress plate. The less involved condyle can then be stabilized with smaller implants, such as an antiglide plate, cannulated screws, or a fine-wire circular external fixator (Ilizarov/Taylor Spatial Frame) in cases of extreme comminution or compromised soft tissues.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative protocol must balance the need for early joint mobilization to nourish the articular cartilage with the necessity of protecting the osteosynthesis construct.
- Immobilization: The knee is placed in a hinged knee brace locked in extension immediately postoperatively.
- Early Motion: At 24 to 48 hours postoperatively, continuous passive motion (CPM) or active-assisted range of motion (ROM) exercises are initiated. Early motion prevents intraarticular adhesions and promotes cartilage healing. Exception: If extensive meniscal repair or collateral ligament repair was performed, motion may be delayed or restricted for 3 to 4 weeks.
- Weight-Bearing: Strict non-weight-bearing (NWB) or toe-touch weight-bearing (TTWB) is enforced for 10 to 12 weeks. Premature weight-bearing is the leading cause of construct failure and articular subsidence.
- Progression: Progressive weight-bearing is initiated only after radiographic evidence of bridging callus and clinical absence of pain at the fracture site, typically advancing to full weight-bearing by 16 weeks.
