DEFINITION
Arthritis between the radial styloid and the distal aspect of the scaphoid can lead to pain, weakness of grip, and limitation of motion. This arthritis can occur in the early stages of a variety of pathologic states of the radiocarpal joint.Radial styloidectomy is a technique that involves resection of the distalmost aspect of the articular surface of the distal radius.A radial styloidectomy can be performed as a distinct procedure via an open incision or by arthroscopic means. It is more commonly undertaken as an adjunct procedure with reconstructive or salvage procedures for scaphoid nonunions, carpal instabilities, Kienböck disease, or posttraumatic arthritis of theradiocarpal joint.10,22
ANATOMY
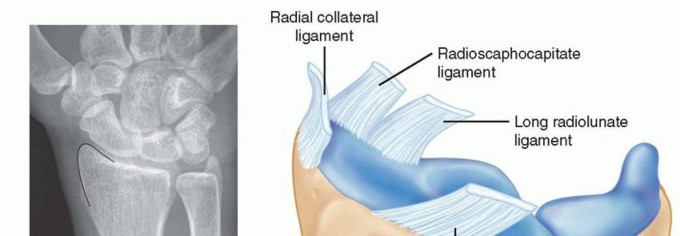
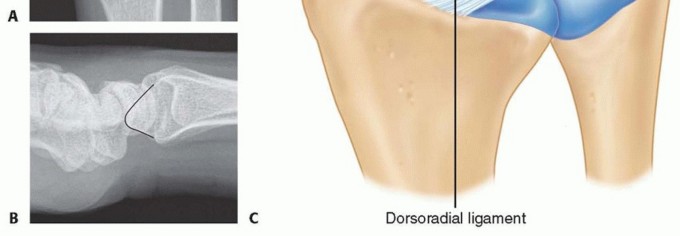
FIG 1 • A,B. The radial styloid outlined on a standard posteroanterior (PA) and lateral wrist radiograph. C. Palmar and dorsal extrinsic ligaments of the radiocarpal joint. Note the broad origin of the dorsoradial ligament. The RCL originates from the tip of the styloid. The RSC and LRL ligaments are separated by a well-defined sulcus readily seen arthroscopically.
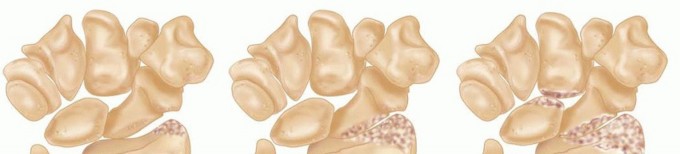
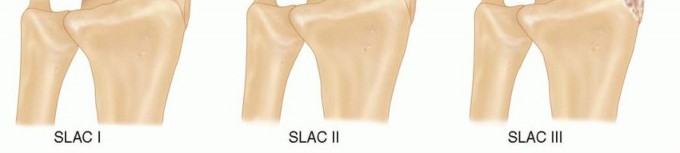
FIG 3 • Stages of arthritis with SLAC. SLAC I: degenerative changes are confined to the radial styloid. SLAC II: joint space narrowing of the entire radioscaphoid articulation. SLAC III: chondral changes in the radioscaphoid and capitolunate joint.
PATHOGENESIS AND NATURAL HISTORY
SCAPHOLUNATE INSTABILITY
Watson and Ballet21 reviewed radiographs of individuals with scapholunate dissociation to establish the sequential progression of arthritis in the scapholunate advanced collapse (SLAC) wrist (FIG 3).SLAC I: Degenerative changes are confined to the radial styloid area.SLAC II: Changes are characterized by joint space narrowing involving the entire radioscaphoid articulation. SLAC III: Changes involve additional arthritis between the capitate and lunate.Several authors have examined the mechanics of scapholunate dissociation in cadaver models and have demonstrated that scapholunate instability leads to a shift in the contact pressures from the proximal pole of scaphoid articulation with the radial articular surface toward the distal pole of the scaphoid with the dorsal lipof the radial styloid.7,8 The pathomechanics of these changes can occur even before the frank radiographic appearance of scapholunate diastasis is present (ie, static scapholunate instability). Prolonged exposure to these abnormal contact stresses leads to the predictable arthritic changes described earlier.P.969Scaphoid nonunionWith an unstable scaphoid fracture, the proximal pole of the scaphoid remains firmly fixed to and extends with the lunate through an intact scapholunate interosseous ligament. The distal pole adopts a flexed posture, which can then impinge on the radial styloid, leading to abnormal contact stresses and arthritic changes.The natural history of scaphoid nonunion has not been established by rigorous prospective analysis. Nonetheless, most surgeons believe that unstable scaphoid fractures result in abnormal carpal kinematics with a dorsal intercalated segment instability (DISI) deformity and subsequent arthritis (scaphoid nonunion advanced collapse [SNAC] wrist).Vender et al18 examined the radiographs of 64 patients with symptomatic scaphoid nonunions and showed a high frequency of degenerative changes that occurred in a predictable sequence similar to the findings of SLAC wrist. Initial degenerative changes were seen between the radial styloid and the distal fragment of the scaphoid nonunion. Changes then progressed to include the midcarpal joint with sparing of the proximalpole scaphoid and radiolunate articulation.18 Inoue and Sakuma9 reviewed 102 patients with scaphoid nonunions clinically and radiographically; they found that arthritis initially developed at the scaphoid-radial styloid articulation and subsequently the midcarpal joint. All patients had radiographic arthritis within 10 years of injury. They also demonstrated that although radiographic progression did not correlate with wrist pain, it did correlate with a decrease in grip strength and range of motion.Impingement after triscaphe (scaphoid-trapezoid-trapezium) fusionRogers and Watson14 reviewed 93 patients after triscaphe fusion and found a 33% incidence of painful impingement between the fusion mass and the radial styloid that resolved after limited radial styloidectomy. They hypothesized that the fixed scaphoid could no longer be accommodated in the fossa and impacted on the radial styloid.Proximal row carpectomyAlthough not all surgeons routinely perform a radial styloidectomy in the setting of a proximal row carpectomy, a recent cadaveric study demonstrated that radial deviation after proximal row carpectomy waslimited by impingement of the trapezoid on the radial styloid.6
PATIENT HISTORY AND PHYSICAL FINDINGS

IMAGING AND OTHER DIAGNOSTIC STUDIES

FIG 5 • Impingement of the flexed distal pole of the scaphoid nonunion against the radial styloid leading to arthritic changes. P.970Stress radiographs (clenched fist and radial-ulnar deviation posteroanterior) of the wrist can yield information concerning dynamic impingement between the scaphoid and the radial styloid.
DIFFERENTIAL DIAGNOSIS
De Quervain stenosing tenosynovitis: Tenderness usually extends along the extra-articular component of the radial styloid, proximally and radially over the first dorsal compartment. A positive Finkelstein test is highly suggestive of this disorder.Scaphoid-trapezoid-trapezium arthritis: focal tenderness in the distal ulnar aspect of the snuffbox under the extensor pollicis long tendon along the axis of the second metacarpalThumb carpometacarpal instability or arthritis: tenderness distal to the anatomic snuffbox that is worsened by loading of the thumb ray (carpometacarpal grind test)Scaphoid fracture: After an acute injury, advanced imaging (bone scan or magnetic resonance imaging [MRI]) may be required to rule out an acute scaphoid fracture.Preiser diseaseInflammatory arthritis (ie, rheumatoid arthritis, gout, pseudogout) Radial sensory neuritis or neuromaTenosynovitis of the extensor carpi radialis longus and brevisNot uncommonly, styloid impingement coexists with other diagnoses, especially basilar thumb arthritis and de Quervain stenosing tenosynovitis.
NONOPERATIVE MANAGEMENT
Individuals with chronic SLAC or SNAC wrist arthritis frequently present with acute pain after a recent injury.After obtaining an accurate medical history of prior injury and radiographic assessment, the chronicity of the problem is usually evident.In this situation, a course of conservative treatment with activity modification, nonsteroidal anti-inflammatory drugs, rest in a forearm-based thumb spica splint, and selective corticosteroid injection in the radial styloid area is appropriate.If the arthritic changes are truly isolated to the area of articulation between the scaphoid and the styloid, the surgeon may elect earlier operative intervention with the theoretical goal of slowing or preventing progressive symptomatic arthrosis and the need for a more extensive reconstructive procedure.
SURGICAL MANAGEMENT
Isolated radial styloidectomy is a limited procedure to treat the early stage of progressive posttraumatic arthritis.It cannot be expected to prevent its pathologic progression.It can also be employed as a temporizing solution in a lowdemand individual or in a patient unfit or unwilling to undertake a more extensive procedure and postoperative rehabilitative course.In that instance, patient expectations with respect to motion and pain relief must be assiduously managed.Arthroscopic radial styloidectomy has the theoretical advantages of being minimally invasive and allowing more precise control of the level of bony resection to minimize injury to the palmar radiocarpal ligaments. In addition, arthroscopic evaluation of the radiocarpal and midcarpal joints can allow for diagnosis and treatmentof concomitant intra-articular pathology.22
PREOPERATIVE PLANNING
Precise radiographic assessment and patient selection are critical in ensuring a good outcome. The surgeon must review all radiographic studies and the severity, characteristics, and nature of the patient's symptoms and physical findings.In some cases, final staging of the severity of articular degeneration can be made only by direct visualization with diagnostic wrist arthroscopy (FIG 6). In situations where there is incompetency of the RSC ligament (eg, rheumatoid arthritis, gout, pseudogout) radial styloidectomy may be contraindicated in that it might cause ulnar translocation of the carpus. An isolated radial styloidectomy or a more extensive reconstructive procedure can be done at the time of arthroscopy or at a later time, after the implications of the arthroscopic findings are discussed with the patient.
POSITIONING
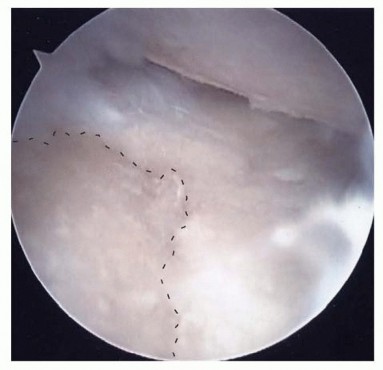
FIG 6• Arthroscopic findings of full-thickness cartilage loss in the entire scaphoid facet (dashed line) and proximal pole of the scaphoid as viewed from the dorsal 3-4 portal. These degenerative changes were not readily apparent on plain radiographs. An isolated radial styloidectomy cannot be expected to confer pain relief in this instance.P.971Alternatively, the hand can be suspended via finger traps using a nonsterile overhead traction boom (ie, an arthroscopic shoulder holder); with this method, the wrist traction tower will not be an impediment to intraoperative fluoroscopic assessment (FIG 7).
APPROACH




FIG 7 • An alternative arthroscopic setup can be useful. A nonsterile overhead traction boom (an arthroscopic shoulder holder) is used from the contralateral side of the operating room table to suspend the limb via finger traps with countertraction provided by a strap on the arm. With this method, the fluoroscopic images of the wrist can be obtained without being obscured by the arthroscopic wrist tower.
TECHNIQUES
OPEN RADIAL STYLOIDECTOMY




TECH FIG 1 • Open radial styloidectomy. A. A 2- to 3-cm oblique skin incision is made between the first and second extensor compartments. Note the branches of the radial sensory and lateral antebrachial cutaneous nerves. B. The first dorsal compartment is then opened.(continued)




TECH FIG 1 •(continued)C. The radial styloid is extraperiosteally exposed by sharp dissection. D. An osteotome is used to resect the distal 3 to 4 mm of radial styloid. The osteotome should be angled perpendicular to the joint surface. E. The resected radial styloid is removed. F,G. Preoperative and postoperative PA radiographs of the wrist with early SNAC undergoing open radial styloidectomy. (Courtesy of Dr. John J. Fernandez.)
ARTHROSCOPIC STYLOIDECTOMY
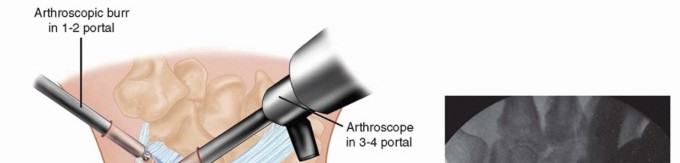

TECH FIG 2 • Arthroscopic radial styloidectomy. A.The arthroscopic burr is in the 1-2 portal and the arthroscope is in the 3-4 portal. B. Fluoroscopic image obtained during arthroscopic radial styloidectomy for scapholunate instability and secondary degeneration. Note the disruption of the line of Gilula in the proximal carpal row.
PEARLS AND PITFALLS
|Indications ▪ A complete history and physical examination emphasizing clinical staging is essential. The final decision to proceed with styloidectomy may require staging arthroscopy.Insufficient or ▪ Arthroscopic visualization of the RSC ligament to prevent significant injury excessive styloid and to assure its competencyresection ▪ Using the diameter of the burr as a gauge for the amount of bone resected1. Intraoperative fluoroscopic evaluationPoor ▪ Convert from arthroscopic to open procedure. arthroscopicvisualization|
POSTOPERATIVE CARE
If the radial styloidectomy is performed concomitantly with another reconstructive procedure (PRC, four-corner arthrodesis, scaphoid bone grafting and fixation), the rehabilitation is dictated by the requirements of that additional procedure.After either open or arthroscopic radial styloidectomy, the postoperative dressing and sutures are removed in 7 to 10 days. Early active, active-assisted, and passive motion is initiated under the guidance of a hand therapist. Usually, a removable splint is used initially for patient comfort. As the patient's symptoms permit, graded strengthening and unrestricted activities are allowed.
OUTCOMES
Barnard and Stubbins1 first described a radial styloidectomy as part of an operative treatment strategy for scaphoid nonunion in 14 patients in 1948. They thought that the styloidectomy removed impingement, enhanced exposure of the scaphoid, and provided material for bone grafting from the same operative field. Since that time, there have been no series of outcomes in the indexed English literature for outcomes after isolated open radial styloidectomy. Several reports of radial styloidectomy performed with open reduction and internal fixation of scaphoid nonunion or with triscaphe fusion have demonstratedgood pain relief but no significant improvement in range of motion.14,21Ruch et al15 were the first to describe the use of an arthroscopic radial styloidectomy in the treatment ofavascular necrosis of the proximal pole following scaphoid nonunion. Page et al13 presented their experience with the arthroscopic technique in 22 patients to the European Federation of National Associations of Orthopaedics and Traumatology in 2003. In short-term follow-up, they reported 75% goodand satisfactory results. Levadoux and Cognet11 reviewed their results in 12 patients with SLAC I and SLAC II arthritic changes with average follow-up of 39 months. They showed an 18% increase in grip strength and high patient satisfaction; 80 % of their patients experienced complete relief of their wristpain. Birman et al5 performed arthroscopic radial styloidectomy combined with arthroscopic débridement and selective anterior and posterior interosseous neurectomies in advanced SLAC wrist (II and III) in an effort to delay or avoid salvage procedures in eight wrists. At an average of 28 months post procedure, they had maintained good motion and had a 71% satisfaction rate. The authors, however, did caution that this is best thought of as an intermediate procedure to relieve pain and preserve motion.P.974Radial styloidectomy is most often performed as a limited procedure to address posttraumatic arthritis of the wrist early in its pathogenesis. Although it can provide long-lasting symptomatic relief, it cannot be expected to halt the progression of the arthritis. A successful radial styloidectomy could be one in which a more extensive reconstructive procedure was delayed by several years.
COMPLICATIONS
Incomplete resection leading to persistent painExcessive resection leading to extrinsic ligament incompetence and wrist instability with ulnartranslocationNerve injury to the terminal branches of the radial sensory nerve or lateral antebrachial cutaneous nerve ArthrofibrosisInfectionComplex regional pain syndrome
REFERENCES
- Barnard L, Stubbins SG. Styloidectomy of the radius in the surgical treatment of nonunion of the carpal navicular: a preliminary report. J Bone Joint Surg Am 1948;30(1):98-102.
- Beldner S, Zlotolow DA, Melone CP Jr, et al. Anatomy of the lateral antebrachial cutaneous and superficial radial nerve in the forearm: a cadaver and clinical study. J Hand Surg Am 2005;30(6):1226-1230.
- Berger RA. The ligaments of the wrist. A current overview of anatomy with considerations of their potential functions. Hand Clin 1997;13:63-82.
- Berger RA, Landsmeer JM. The palmar radiocarpal ligaments: a study of adult and fetal human wrist joints. J Hand Surg Am 1990;15(6):847-854.
- Birman MV, Danoff JR, Rosenwasser MP. Arthroscopic wrist debridement and radial styloidectomy for late stage scapholunate advanced collapse wrist. Presented at the Arthroscopy Association of North America annual meeting, Orlando, FL, May 2012.
- Blankenhorn BD, Pfaeffle HJ, Tang P, et al. Carpal kinematics after proximal row carpectomy. J Hand Surg Am 2007;32(1):37-46.
- Blevens AD, Light TR, Jablonsky WS, et al. Radiocarpal articular contact characteristics with scaphoid instability. J Hand Surg Am 1989;14(5):781-790.
- Burgess RC. The effect of rotatory subluxation of the scaphoid on radio-scaphoid contact. J Hand Surg Am 1987;12(5 pt 1):771-774.
- Inoue G, Sakuma M. The natural history of scaphoid non-union. Radiographical and clinical analysis in 102 cases. Arch Orthop Trauma Surg 1996;115:1-4.
- Kalainov DM, Cohen MS, Sweet S. Radial styloidectomy. In: Geissler WB, ed. Wrist Arthroscopy. New York: Springer-Verlag, 2005:134-138.
- Levadoux M, Cognet JM. Arthroscopic styloidectomy [in French]. Chir Main 2006;25(suppl 1):S197-S201.
- Nakamura T, Cooney WP III, Lui WH, et al. Radial styloidectomy: a biomechanical study on the stability of the wrist. J Hand Surg Am 2001;26(1):85-93.
- Page RS, Waseem M, Stanley JK. Clinical outcome of arthroscopic radial styloidectomy. J Bone Joint Surg Br 2004;86B:280.
- Rogers WD, Watson HK. Radial styloid impingement after triscaphe arthrodesis. J Hand Surg Am 1989;14(2 pt 1):297-301.
- Ruch DS, Chang DS, Poehling GG. The arthroscopic treatment of avascular necrosis of the proximal pole following scaphoid nonunion. Arthroscopy 1998;14:747-752.
- Siegel DB, Gelberman RH. Radial styloidectomy: an anatomical study with special reference to radiocarpal intracapsular ligamentous morphology. J Hand Surg Am 1991;16(1):40-44.
- Slutsky DJ. Wrist arthroscopy. In: Wolfe SW, Pederson WC, Hotchkiss RN, et al, eds. Green's Operative Hand Surgery. Philadelphia: Elsevier, 2011:709-741.
- Vender MI, Watson HK, Wiener BD, et al. Degenerative change in symptomatic scaphoid nonunion. J Hand Surg Am 1987;12(4):514-519.
- Viegas SF, Patterson RM, Ward K. Extrinsic wrist ligaments in the pathomechanics of ulnar translation instability. J Hand Surg Am 1995;20(2):312-318.
- Viegas SF, Yamaguchi S, Boyd NL, et al. The dorsal ligaments of the wrist: anatomy, mechanical properties, and function. J Hand Surg Am 1999;24(3):456-468.
- Watson HK, Ballet FL. The SLAC wrist: scapholunate advanced collapse pattern of degenerative arthritis. J Hand Surg Am 1984;9(3):358-365.
- Yao J, Osterman AL. Arthroscopic techniques for wrist arthritis (radial styloidectomy and proximal pole hamate excision). Hand Clin 2005;21:519-526.
