Introduction & Epidemiology
Nonaccidental injury (NAI), also known as child physical abuse, represents a significant public health crisis with profound implications for pediatric patients, often presenting initially within orthopedic contexts. As academic orthopedic surgeons and educators, it is incumbent upon us to possess a refined understanding of NAI, its characteristic presentations, and the multidisciplinary responsibilities involved in its identification and management. While the global incidence is challenging to ascertain due to underreporting, estimates suggest millions of children worldwide are affected annually by physical abuse. In the United States, child protective services receive millions of referrals each year, a substantial percentage involving physical abuse, with infants and toddlers at highest risk. Fractures are the second most common manifestation of NAI, trailing only cutaneous injury, and are the most common cause of morbidity and mortality in abused infants.
The orthopedic surgeon's role extends beyond the immediate treatment of an injury; it critically involves identifying patterns of injury inconsistent with reported mechanisms, recognizing specific fracture types indicative of abuse, differentiating NAI from accidental trauma or medical conditions mimicking abuse, and initiating appropriate diagnostic and protective measures. A missed diagnosis of NAI carries a grave prognosis, with a significantly increased risk of recurrent injury and fatality. Conversely, an incorrect diagnosis can have devastating consequences for families. Therefore, meticulous evaluation, objective documentation, and collaborative care are paramount. This review aims to distill high-yield knowledge for orthopedic residents, fellows, and practicing surgeons on recognizing the red flags of NAI in pediatric patients.
Surgical Anatomy & Biomechanics
The biomechanics of NAI often involve direct impact, twisting, shaking, or crushing forces, leading to specific fracture patterns that warrant a high index of suspicion. Understanding the typical injury patterns in accidental trauma for different age groups is crucial for contrast. For instance, a clavicle fracture is common in neonates after difficult delivery or in older children from falls, but a femoral shaft fracture in a non-ambulatory infant is highly suspicious.
Characteristic Fracture Patterns Indicative of NAI
- Metaphyseal Corner Fractures (MCFs) / Bucket-Handle Fractures : These are considered pathognomonic for NAI, particularly in infants and young children. They result from shear and torsional forces applied to the physis, often from violent shaking or pulling of an extremity. The injury involves the primary spongiosa, leading to a small fragment avulsed from the metaphysis. Radiographically, they appear as a crescent-shaped or bucket-handle lucency parallel to the physis. Common locations include the distal femur, proximal tibia, and proximal/distal humerus. The biomechanical mechanism requires forces that exceed the strength of the developing physeal-metaphyseal junction, which is cartilaginous and relatively weak compared to ligaments in young children.
- Rib Fractures : Especially posterior and posterolateral rib fractures, multiple rib fractures, or fractures at different stages of healing. These are highly specific for NAI, resulting from anterior-posterior compression of the chest (squeezing) or direct impact. Due to the pliability of pediatric ribs and the protection offered by surrounding musculature, significant force is required to fracture them. Posterior rib fractures are particularly suspicious as they are difficult to sustain accidentally.
- Scapular Fractures, Sternal Fractures, Spinous Process Fractures : These are rare in accidental trauma in children, typically requiring high-energy mechanisms (e.g., motor vehicle collisions, falls from significant heights). Their presence in the absence of a convincing high-energy mechanism should raise strong suspicion for NAI.
- Long Bone Diaphyseal Spiral Fractures in Non-Ambulatory Infants : A spiral fracture of a long bone (e.g., tibia, femur, humerus) in a child who cannot walk or crawl independently suggests a rotational or twisting force, often consistent with pulling or twisting of a limb during abuse. While spiral fractures can occur accidentally in older, ambulatory children, their presence in an infant necessitates thorough investigation.
- Complex Skull Fractures or Depressed Skull Fractures : While linear skull fractures can occur accidentally, complex, comminuted, or depressed skull fractures, particularly those that cross suture lines or are associated with intracranial hemorrhage without a clear history, are highly suspicious.
- Vertebral Fractures : Compression fractures or spinous process fractures in young children, especially without a documented axial load injury or significant trauma, are uncommon and suggestive of NAI.
- Epiphyseal Separations : Traumatic epiphyseal separations, particularly Salter-Harris type I or II injuries, can be challenging to detect radiographically in very young children due to the cartilaginous nature of the epiphysis. These can occur due to shear or torsional forces across the growth plate, mechanisms common in NAI.
- Multiple Fractures in Various Stages of Healing : This is a cardinal sign of ongoing abuse. Radiographs may reveal both acute and healing fractures, indicating repeated traumatic events over time. This finding necessitates a full skeletal survey.
- Fractures Inconsistent with Developmental Stage : For example, a femur fracture in a pre-ambulatory infant who cannot yet roll over or crawl. The reported mechanism of a "fall" is often inconsistent with the physical capabilities of the child.
Soft Tissue Indicators
Beyond skeletal injury, the presence of specific soft tissue injuries can be powerful red flags:
*
Bruising Patterns
: Bruises in non-ambulatory infants, bruises on the torso, ears, neck, or inner thighs are highly concerning. Patterned bruises (e.g., from an object like a belt buckle, handprint) are definitive signs of abuse.
*
Burns
: Especially "glove and stocking" pattern burns (immersion burns), geometrically shaped burns, or multiple burns in various stages of healing.
*
Oral Injuries
: Lacerations to the frenulum, gum injuries, or chipped teeth in infants who are not yet walking.
*
Ocular Injuries
: Retinal hemorrhages, often associated with abusive head trauma (shaken baby syndrome).
The interaction of these findings, particularly in combination, significantly increases the likelihood of NAI.

Indications & Contraindications
The indications and contraindications for intervention in NAI are not strictly surgical but rather diagnostic, investigative, and protective. For the orthopedic surgeon, the primary "indication" is a high index of suspicion that mandates a comprehensive assessment and multidisciplinary team involvement. There are no "contraindications" to considering NAI in a child with suspicious injuries; rather, there is a contraindication to not considering it when red flags are present.
Indications for NAI Suspicion and Comprehensive Investigation
- Injury Inconsistent with History : The most common red flag. Discrepancies between the reported mechanism and the severity or type of injury (e.g., a spiral femoral fracture from a "fall off the couch").
- Inconsistent or Evolving History : Caregivers provide conflicting accounts, or the history changes over time or among different caregivers.
- Delayed Presentation : Significant injuries (e.g., a grossly displaced fracture) for which medical attention is sought hours or days after the purported event.
- Caregiver Demeanor : Overly aggressive, indifferent, or inappropriately calm behavior; blaming the child; refusing to leave the child's bedside; or conversely, not visiting.
- Specific Fracture Patterns : As detailed in the "Surgical Anatomy & Biomechanics" section (e.g., MCFs, posterior rib fractures, multiple fractures at different healing stages).
- Bruises in Non-Ambulatory Infants : Any bruising in an infant who is not yet cruising or walking independently warrants investigation.
- Unusual Bruise Locations : Torso, ear, neck, inner thigh, groin, axilla.
- Patterned Bruises or Burns : Imprints of objects (e.g., belt, hand), immersion burns.
- Repeated Injuries : Frequent visits to the emergency department for seemingly minor injuries.
- Signs of Neglect : Poor hygiene, malnourishment, developmental delay.
- Sibling with Known NAI : A prior history of NAI in a sibling significantly increases the risk for other children in the household.
- Radiographic Findings : Periosteal reaction indicative of subacute trauma, specific fracture types, or multiple fractures of different ages.
Operative vs. Non-Operative Management of Orthopedic Injuries in the Context of NAI
The decision between operative and non-operative management for a specific orthopedic injury in a pediatric NAI patient generally follows standard pediatric orthopedic principles. However, the NAI context introduces critical additional considerations.
| Fracture Type / Injury Characteristic | Operative Indications (Standard Principles) | Non-Operative Indications (Standard Principles) | NAI-Specific Considerations & Modifications |
|---|---|---|---|
| Femur Fracture (Infant/Toddler) | Displaced, unstable, open fracture, associated vascular/nerve injury. | Stable, minimally displaced, <6 months (Pavlik), 6 mo-5 yr (spica cast). | High suspicion for NAI. Immediate skeletal survey, ophthalmologic exam, comprehensive medical evaluation. Consider non-operative (spica) for younger patients to minimize invasiveness, but ensure secure environment and compliance with cast care (e.g., hospital admission, temporary foster care). Meticulous documentation of injury characteristics. |
| Metaphyseal Corner Fracture (MCF) | Rare, only for severe articular involvement or growth plate disruption (uncommon). | Most are managed non-operatively (immobilization for comfort). | Pathognomonic for NAI. Requires full NAI protocol regardless of orthopedic management. Immobilization for comfort, but focus is on the NAI investigation and child safety. Bone scan often complements skeletal survey for occult fractures. |
| Rib Fractures | Extremely rare for orthopedic intervention, only for flail chest with respiratory compromise or specific internal organ injury requiring access. | Almost universally non-operative (pain management, respiratory support). | Highly specific for NAI, especially posterior. Full NAI protocol mandatory. Monitor respiratory status. Document number, location, and age of fractures. Search for other occult injuries (e.g., lung contusion). |
| Spiral Tibia Fracture (Toddler) | Grossly unstable, open fracture, significant soft tissue injury. | Stable, minimally displaced (long leg cast). | Consider NAI, especially if non-ambulatory or inconsistent history. This is the "toddler's fracture" when accidental, but always consider abuse if history inconsistent or child is too young to twist and fall. Full NAI protocol if suspicious. Ensure adequate cast surveillance. |
| Skull Fracture | Depressed fracture requiring elevation, ongoing intracranial hemorrhage requiring evacuation. | Linear, non-depressed, no intracranial bleed (observation). | High suspicion for NAI if complex, depressed, or with intracranial findings without convincing history. Detailed neurological assessment, neurosurgical consultation, forensic imaging (CT/MRI brain), ophthalmologic exam (retinal hemorrhages). NAI protocol. |
| Growth Plate Injuries | Unstable, displaced Salter-Harris types III-V, articular incongruity. | Stable Salter-Harris types I-II, minimally displaced. | Increased risk in NAI. Document meticulously for potential growth disturbance and long-term implications. Consider bone health issues (e.g., nutritional deficiencies often seen in neglect). Precise reduction and fixation are critical to minimize future deformity. |
| Multiple Fractures of Different Ages | Manage each fracture individually based on type/location. | Manage each fracture individually based on type/location. | Cardinal sign of NAI. Immediate and comprehensive NAI protocol. This indicates ongoing abuse. Focus on securing child's safety first and foremost. Orthopedic management must occur in a safe environment. Prognosis for healing may be affected by underlying neglect/malnutrition. |
| Open Fractures | Debridement, irrigation, stabilization (emergent). | N/A | Always raise NAI suspicion, especially if associated with suspicious soft tissue injuries or history. Meticulous wound care. Forensic photography of wound characteristics. High risk of infection and complications in NAI context due to potential delayed presentation or neglect. |
| Fracture with Associated Vascular/Nerve Injury | Emergent surgical repair/reconstruction. | N/A | NAI strongly suspected. Requires high-level trauma assessment in addition to NAI protocol. Document neurological deficits and vascular compromise meticulously for forensic purposes. Outcomes may be influenced by delayed presentation. |
Contraindications
While there are no contraindications to
considering
NAI, there are medical conditions that can
mimic
NAI and must be ruled out before a definitive diagnosis of abuse is made. These include:
*
Osteogenesis Imperfecta (OI)
: A group of genetic disorders causing bone fragility. Type I is the most common and often confused with NAI. Features include blue sclera, dentinogenesis imperfecta, and hearing loss. Fractures tend to be diaphyseal and transverse.
*
Rickets
: Vitamin D deficiency leading to osteomalacia and metaphyseal widening or fraying, potentially confused with healing MCFs.
*
Copper Deficiency / Menkes Disease
: Rare genetic disorder causing brittle hair, hypotonia, and severe growth retardation.
*
Scurvy
: Vitamin C deficiency causing subperiosteal hemorrhage and bone pain.
*
Congenital Syphilis
: Can cause osteochondritis and periostitis.
*
Leukemia or other Malignancies
: Can present with bone pain and pathological fractures.
*
Ehlers-Danlos Syndrome
: Connective tissue disorder causing joint hypermobility and skin fragility, rarely associated with spontaneous fractures.
*
Toddler's Fracture
: A non-displaced spiral fracture of the tibia in a walking toddler, typically an accidental injury from a low-energy twist.
A thorough medical workup, including a skeletal survey, specific lab tests (e.g., Vitamin D, calcium, phosphorus, alkaline phosphatase, copper levels, genetic testing for OI if indicated), and consultation with genetics or metabolic specialists, is crucial to differentiate NAI from these conditions. The presence of these medical conditions, however, does not preclude concurrent NAI.
Pre-Operative Planning & Patient Positioning
Pre-operative planning for an orthopedic injury in a pediatric patient suspected or confirmed to be a victim of NAI involves layers of considerations beyond typical surgical planning. The emphasis shifts from solely addressing the anatomical injury to ensuring the child's holistic safety, well-being, and proper legal/forensic documentation.
Comprehensive Pre-Operative Planning
- Multidisciplinary Team Activation : Immediately involve Child Protective Services (CPS), social work, hospital legal counsel, pediatrics (especially child abuse pediatricians), and potentially forensic photography specialists. This team approach is essential for coordinated care, investigation, and protection.
-
Detailed History and Physical Examination
:
- History : Obtain a thorough history from all involved caregivers separately . Document any inconsistencies verbatim. Do not be confrontational; rather, be empathetic and objective in data collection. Document the mechanism of injury, time of injury, presenting symptoms, and any previous injuries or medical conditions.
- Physical Exam : Document all visible injuries, including cutaneous findings (bruises, abrasions, burns, lacerations), their size, shape, color, and location. Use body diagrams. Take detailed photographs. Assess for non-orthopedic signs of abuse (e.g., abdominal tenderness, neurological changes, retinal hemorrhages requiring ophthalmology consult).
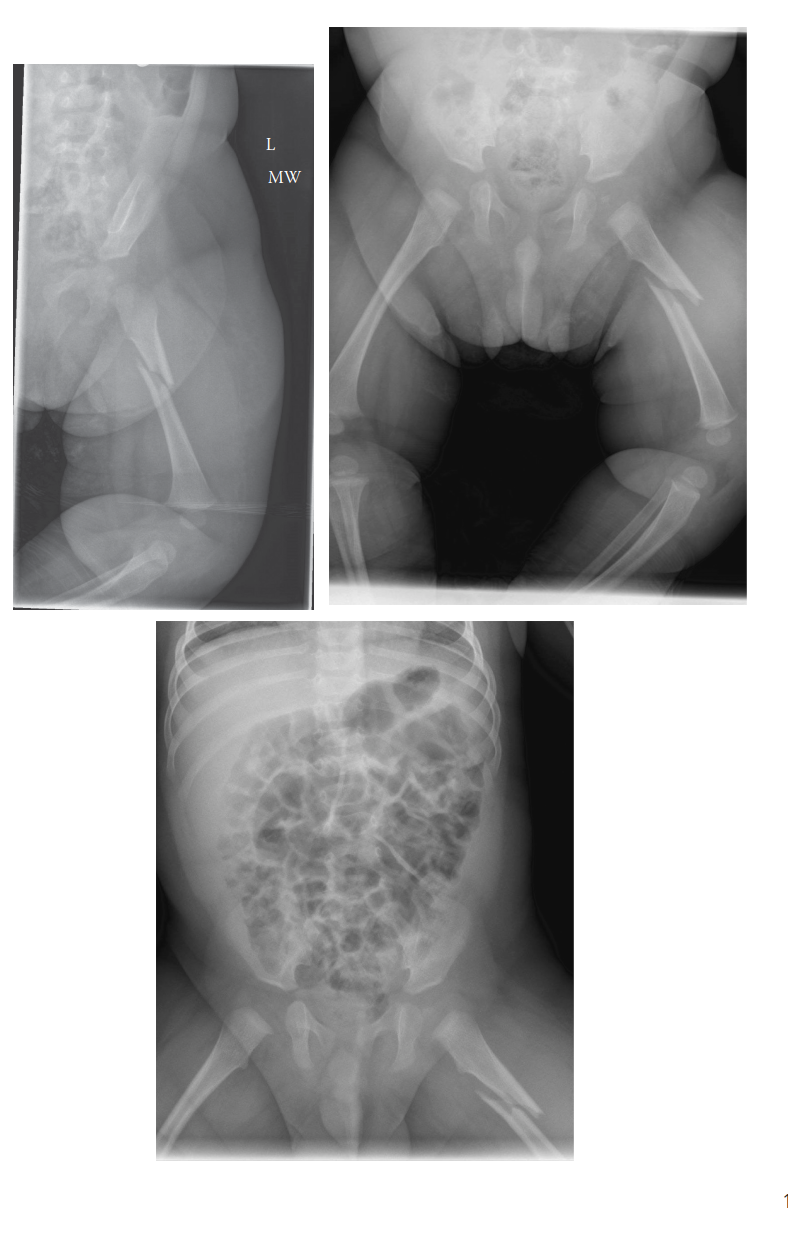
- Skeletal Survey : This is mandatory for any child under the age of two with suspicious fractures, and often recommended for children up to five years old with any high-suspicion fracture. It must be a complete series of radiographs covering all bones (skull, chest, spine, pelvis, bilateral upper and lower extremities), specifically looking for occult fractures, fractures of different ages, and characteristic NAI patterns. A follow-up skeletal survey at 2-3 weeks may be indicated to identify healing fractures that were not visible acutely.
-
Adjunctive Imaging
:
- Bone Scan (Technetium-99m Methylene Diphosphonate) : Can detect occult fractures, particularly rib fractures, metaphyseal fractures, and soft tissue injuries, which may not be visible on plain radiographs acutely. However, it may miss skull fractures and early MCFs.
- Computed Tomography (CT) : For skull fractures, intracranial injuries (subdural hematoma, epidural hematoma, contusions).
- Magnetic Resonance Imaging (MRI) : For spinal injuries, soft tissue damage, and more detailed assessment of intracranial injuries, especially in suspected abusive head trauma.
-
Laboratory Workup
: Rule out medical mimics of NAI. This typically includes:
- Complete Blood Count (CBC)
- Coagulation panel (PT/PTT/INR)
- Comprehensive Metabolic Panel (CMP)
- Calcium, phosphorus, alkaline phosphatase
- Vitamin D levels
- Genetic testing for Osteogenesis Imperfecta (e.g., COL1A1/COL1A2) if clinically indicated after initial workup.
- Forensic Documentation : All findings (history, physical exam, imaging, lab results) must be meticulously documented in the medical record. Use clear, objective language, avoiding judgmental terms. Ensure all necessary reports (e.g., CPS referral, police report) are filed according to institutional and state guidelines. Photographs should be high-quality, timestamped, and part of the legal record.
- Surgical Consent : Consent should be obtained from the legal guardian(s). In situations where NAI is strongly suspected, and CPS has removed the child from parental custody, CPS or a court-appointed guardian may provide consent. This must be clarified prior to any invasive procedure.
- Psychological Support : Prepare the child for surgery with age-appropriate psychological support (e.g., child life specialists). Acknowledge potential distress related to separation from caregivers, even abusive ones.
- Operating Room Environment : Maintain a secure and calm environment. Consider limiting access to the OR to essential personnel. Ensure all necessary equipment for the planned orthopedic procedure is available, anticipating potential issues like poor bone quality.
Patient Positioning
Patient positioning for orthopedic procedures in NAI cases largely follows standard protocols for the specific fracture type and location. However, specific considerations include:
*
Gentle Handling
: Due to potential for widespread injuries, bone fragility, or pain, extreme care must be taken during transfer and positioning.
*
Documentation of Pre-existing Injuries
: Before draping, ensure all pre-existing external injuries (bruises, abrasions) are clearly documented and, if possible, photographed.
*
Temperature Regulation
: Young children are prone to hypothermia, which can be exacerbated by NAI (e.g., poor nutritional status, prolonged exposure). Meticulous attention to warming devices is essential.
*
Anesthetic Considerations
: Pediatric anesthesia consultation is crucial, considering potential for complex medical comorbidities, dehydration, or occult head/abdominal injuries.
Detailed Surgical Approach / Technique
When orthopedic surgery is required for an NAI-related fracture, the approach and technique must reflect both standard pediatric orthopedic principles and the unique context of NAI. The focus is on meticulous execution, durable fixation, and minimizing complications in patients who may have underlying vulnerabilities or be at risk for non-compliance with post-operative care.
Principles of Surgical Management for NAI-Related Fractures
- Stable and Durable Fixation : Given the potential for delayed healing (due to neglect, poor nutrition, or underlying bone health issues) and the imperative to facilitate early mobilization for developmental purposes, robust fixation is paramount. The goal is to achieve an anatomical or near-anatomical reduction and provide stability that will withstand early activity and potential challenges in post-operative supervision.
- Minimally Invasive Approaches : Whenever feasible, utilize percutaneous pinning, flexible intramedullary nailing, or other minimally invasive techniques. This reduces soft tissue stripping, minimizes surgical trauma, and may lead to faster healing and better cosmesis. However, the decision should always prioritize stable fixation over minimal invasiveness if stability is compromised.
-
Appropriate Implant Choice
:
- K-wires : Useful for physeal injuries (e.g., Salter-Harris fractures), metaphyseal fractures, or small bone fractures. They offer stability with minimal surgical footprint.
- Flexible Intramedullary Nails (e.g., Fassier-Duval, Nancy nails) : Excellent for diaphyseal long bone fractures (femur, tibia, humerus) in older infants and young children, allowing for controlled motion and remodeling.
- Plates and Screws : Reserved for complex fractures, articular involvement, or situations requiring absolute stability (e.g., forearm fractures, specific tibial fractures). Care must be taken to choose appropriate size and material.
- External Fixation : May be indicated for open fractures, severe soft tissue compromise, or complex multi-fragmentary fractures, especially where long-term cast care is a concern in an unsafe environment.
- Consideration of Bone Quality : Patients with NAI may have osteopenia due to neglect, poor nutrition, or prolonged immobility. Implants should be chosen and placed carefully to ensure adequate purchase and avoid iatrogenic fracture.
- Meticulous Documentation During Surgery : Intraoperative photographs of the reduced fracture, implant placement, and any unexpected findings (e.g., signs of previous trauma, unusual bone characteristics) are critical for forensic purposes and future reference.
- Bone Biopsy (Selective Use) : In very specific cases, if there is persistent strong suspicion of NAI despite negative workup for medical mimics, or if the fracture pattern is highly atypical, a bone biopsy may be considered. This is controversial and requires careful discussion with the multidisciplinary team, as its utility in definitively diagnosing abuse or ruling out specific genetic conditions can be limited and carries inherent risks. It is typically reserved for research or highly ambiguous cases where genetic testing is non-diagnostic.
Examples of Surgical Techniques for Common NAI-Related Fractures
-
Femur Fractures in Infants/Toddlers
:
- <6 months (or up to 10-12 kg) : Often managed non-operatively with a Pavlik harness or spica cast. Surgical intervention is rare unless there's an open fracture, neurovascular compromise, or irreducible displacement. NAI consideration : Non-operative management relies heavily on caregiver compliance. If the child's safety cannot be assured, hospital admission or temporary removal from the home for cast care may be necessary.
- 6 months to 5 years : Flexible intramedullary nailing is often preferred for displaced or unstable diaphyseal fractures. This allows for early mobilization and potentially shorter hospital stays.
-
Technique (Flexible IMN)
:
- Patient positioned supine on a fracture table or radiolucent table.
- Entry points: usually retrograde from the distal metaphysis (medial and lateral aspects) or antegrade from the proximal greater trochanteric region.
- Two nails, pre-bent into a C-shape, are advanced across the fracture site under fluoroscopic guidance.
- Reduction is achieved either closed or via a limited open approach.
- The nails are left prominent under the skin to facilitate easy removal.
- Internervous planes : Typically percutaneous or through muscle bellies (vastus lateralis/medialis for distal entry, gluteus medius for proximal entry) with minimal stripping.
-
Humeral Shaft Fractures
:
- Non-operative management (coaptation splint, hanging arm cast) is common due to excellent remodeling potential.
- Surgical fixation (flexible IMN, plating) may be indicated for open fractures, neurovascular injury, irreducible displacement, or severely angulated fractures in older children.
- NAI consideration : The history of mechanism needs careful scrutiny, especially in non-ambulatory infants.
-
Forearm Fractures (Radius/Ulna)
:
- Operative fixation (flexible IMN for diaphyseal, K-wires for physeal/metaphyseal) is often required for displaced or unstable fractures to preserve pronation/supination.
- NAI consideration : Assess for concurrent ulna fractures ("nightstick fracture") which can be a direct defensive injury. The presence of these combined with other suspicious findings should trigger NAI evaluation.
- Approach : Typically small incisions over the dorsal or volar aspects of the radius/ulna for pinning or plating.
Other Considerations
- Orthopedic Management of Rib Fractures : These are almost exclusively managed non-operatively, focusing on pain control and respiratory support. The orthopedic surgeon's primary role here is diagnostic confirmation and meticulous documentation for the NAI investigation.
- Physeal Injuries : When operative, precision in reduction and fixation (e.g., smooth K-wires crossing the physis minimally) is vital to prevent growth arrest or angular deformity. Follow-up for growth plate monitoring is critical.
Complications & Management
Complications in NAI cases can arise from the orthopedic injury itself, the NAI diagnosis, or the complex social and legal context. Orthopedic surgeons must be prepared to manage both the physical sequelae and navigate the ethical and legal challenges.
NAI-Specific Complications
-
Recurrence of NAI
: The most devastating complication. If a child returns to an unsafe environment, the risk of repeat injury or fatality is extremely high (up to 50% re-injury rate, 10% mortality).
- Incidence : High if primary NAI factors are not addressed.
- Salvage Strategy : Strict adherence to CPS guidelines, advocating for child's safety (temporary removal from home, foster care, parental supervision plans), continuous communication with social work and legal teams.
-
Long-Term Developmental and Psychological Sequelae
: Children who experience NAI often suffer from developmental delays, cognitive impairments, behavioral problems, PTSD, depression, and anxiety, impacting their entire lives.
- Incidence : Very high, varying with severity and duration of abuse.
- Salvage Strategy : Long-term multidisciplinary follow-up with child development specialists, psychologists, psychiatrists, and early intervention programs. Orthopedic surgeons can refer.
-
Legal/Ethical Dilemmas for the Surgeon
: Includes being subpoenaed to testify in court, facing allegations of misdiagnosis, or navigating conflicts of interest between patient and parental rights.
- Incidence : Moderate to high in confirmed NAI cases.
- Salvage Strategy : Meticulous documentation, objective reporting, seeking legal counsel for the institution, understanding local child abuse reporting laws, peer review of complex cases.
-
Misdiagnosis/Delayed Diagnosis of NAI
: Failure to identify NAI when present, or mistakenly diagnosing NAI when another condition exists.
- Incidence : Moderate, due to complexity and mimics.
- Salvage Strategy : Adherence to NAI diagnostic protocols (skeletal survey, multidisciplinary consults, lab workup), maintaining a high index of suspicion, continuous education, seeking second opinions.
-
Non-Compliance with Follow-up or Rehabilitation
: Caregivers may not adhere to appointments or rehabilitation protocols, risking poor orthopedic outcomes.
- Incidence : Moderate.
- Salvage Strategy : Close communication with social work/CPS to ensure compliance, flexible scheduling, home health referrals, clear communication of consequences of non-compliance.
Orthopedic Complications in NAI Context
These complications are common to orthopedic trauma but may be exacerbated in NAI patients due to factors like neglect, poor nutrition, or delayed presentation.
| Complication | Incidence (Qualitative) | Salvage Strategy |
|---|---|---|
| Delayed Union / Nonunion | Moderate | Incidence possibly higher due to nutritional deficiencies, underlying metabolic bone issues (if undiagnosed), or poor follow-up/immobilization in abusive environments. Aggressive nutritional support (dietary consultation), optimization of vitamin D/calcium, prolonged immobilization, revision surgery with bone grafting or more stable fixation. Close communication with social work/CPS to ensure compliance with immobilization and follow-up. |
| Malunion | Moderate | Can be more challenging to manage due to potential for non-compliance with cast changes or early weight-bearing/activity against advice. Aggressive physical therapy, bracing. Corrective osteotomy in cases of significant functional impairment or unacceptable cosmetic deformity. Careful consideration of growth plate involvement and potential for progressive angular deformity, requiring early intervention. |
| Infection (Surgical Site) | Low to Moderate | Standard infection prophylaxis. Increased risk with open fractures, delayed presentation, and compromised nutritional status. Aggressive debridement, appropriate antibiotic coverage (often broad-spectrum initially), wound care. May require serial debridements. Close monitoring for signs of systemic infection, especially if child is immunocompromised from neglect. |
| Growth Plate Arrest / Deformity | Moderate | Higher risk with physeal injuries, especially Salter-Harris types III-V or those with significant crush/vascular compromise. Meticulous reduction and fixation of physeal fractures. Regular follow-up with serial radiographs to monitor growth. Physis-sparing fixation. Guided growth procedures (hemiepiphysiodesis) or corrective osteotomies for developing angular deformities. Consider the long-term implications for limb length discrepancy. |
| Neurovascular Injury | Low | Potential for delayed recognition if child cannot verbalize symptoms or is subject to neglect. Careful pre-operative neurovascular assessment. Intraoperative monitoring. Immediate surgical exploration and repair. Post-operative neurovascular checks. Document all findings thoroughly, as these can be critical in forensic investigations and impact long-term function. |
| Compartment Syndrome | Low | Risk in high-energy trauma, especially with tibia/forearm fractures. May be missed if child is non-verbal or neglected. High index of suspicion. Frequent clinical assessments. Emergent fasciotomy. Requires close monitoring in hospital. |
| Stiffness / Contracture | Moderate | Potential for limited range of motion if prolonged immobilization or inadequate rehabilitation, especially in the context of limited caregiver engagement. Aggressive physical and occupational therapy. Dynamic or static progressive splinting. Consider manipulation under anesthesia or tenolysis/capsulotomy in refractory cases, carefully weighing risks and benefits given the patient's age and overall situation. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation for a pediatric NAI patient is uniquely challenging, as it must simultaneously address physical recovery, developmental needs, and the overarching need for a safe and nurturing environment. The rehabilitation protocol must be individualized, highly adaptable, and integrated within the multidisciplinary care plan.
Core Principles
- Safety First : The primary goal is to ensure the child is rehabilitating in a physically and emotionally safe environment. This often involves close collaboration with CPS, social work, and legal guardians (if different from biological parents). Rehabilitation in a hospital setting or certified foster care may be necessary initially.
-
Multidisciplinary Approach
: Effective rehabilitation requires a highly coordinated team, including:
- Orthopedic Surgeon : Oversees fracture healing and orthopedic recovery.
- Physical Therapist (PT) : Focuses on gross motor skills, strength, balance, gait, and range of motion.
- Occupational Therapist (OT) : Addresses fine motor skills, activities of daily living (ADLs), sensory integration, and assistive devices.
- Child Life Specialist : Provides emotional support, play therapy, and helps children cope with hospitalization, procedures, and pain.
- Social Worker/CPS : Monitors home environment, facilitates resources, and ensures compliance with follow-up.
- Child Abuse Pediatrician/Medical Doctor : Manages overall medical health, pain, and developmental progress.
- Psychologist/Psychiatrist : Addresses trauma-related psychological and behavioral issues.
- Age-Appropriate and Developmentally Sensitive : Rehabilitation goals and interventions must align with the child's developmental stage. For infants, early gross motor development and parent-child bonding (with safe caregivers) are crucial. For older children, regaining functional independence and addressing emotional well-being become more prominent.
- Gradual Progression : Progress must be carefully monitored. Be vigilant for signs of pain, non-compliance, or re-injury. Weight-bearing status, range of motion, and activity levels are advanced based on fracture healing, clinical tolerance, and the safety of the environment.
- Addressing Co-morbidities : NAI often co-occurs with neglect, leading to malnutrition, developmental delays, and chronic pain. Rehabilitation needs to factor these in, often requiring nutritional support, cognitive stimulation, and pain management strategies.
Phased Rehabilitation Strategy
Phase 1: Acute Healing & Protection (Hospitalization)
*
Focus
: Pain control, initial immobilization, wound care (if operative), basic range of motion (non-affected joints).
*
Activities
:
* Positioning for comfort and healing.
* Gentle passive or active-assisted range of motion of non-immobilized joints.
* Respiratory therapy to prevent complications, especially in children with chest injuries.
* Early mobilization with assistance as tolerated (e.g., in bed, wheelchair).
* Child life engagement for play and coping.
*
NAI Considerations
: Strict adherence to safety plan; constant monitoring in a secure hospital environment. Daily multidisciplinary team meetings to coordinate care and discharge planning.
Phase 2: Subacute Recovery & Functional Restoration (Inpatient/Outpatient Depending on Safety)
*
Focus
: Progressive weight-bearing (if appropriate), strengthening, regaining full range of motion, addressing developmental milestones.
*
Activities
:
* Initiate active range of motion and strengthening exercises.
* Gait training with assistive devices (walker, crutches) as bone healing allows.
* Balance and coordination exercises.
* Occupational therapy for fine motor skills and ADLs.
* Speech therapy if developmental delays are present.
* Psychological counseling for trauma.
*
NAI Considerations
: If the child is discharged, the safety plan must be robust. Home visits by social work/PT/OT may be necessary to assess environment and ensure compliance. Education of caregivers (safe ones) on exercise programs and developmental stimulation. Monitor for signs of non-compliance, regression, or new injuries.
Phase 3: Long-Term Integration & Maintenance
*
Focus
: Full return to age-appropriate activities, monitoring for long-term complications (growth deformities, psychological sequelae), ensuring ongoing support.
*
Activities
:
* Sport-specific training or recreational activities.
* Ongoing psychological therapy as needed.
* Regular follow-up orthopedic visits to monitor fracture healing, implant removal (if necessary), and growth plate status.
* Developmental surveillance.
*
NAI Considerations
: Long-term follow-up with the child abuse pediatrician. Continued support from social services to ensure child remains in a safe, stable environment. Advocacy for the child's educational and social needs.
Summary of Key Literature / Guidelines
The recognition and management of NAI are supported by a substantial body of literature and numerous professional guidelines. Orthopedic surgeons must be familiar with these resources to provide optimal care and fulfill their medico-legal obligations.
Essential Guidelines and Position Statements
-
American Academy of Pediatrics (AAP) Clinical Report: The Evaluation of Suspected Child Physical Abuse (2015, reaffirmed 2019)
: This is a cornerstone document providing comprehensive guidance on the clinical evaluation of suspected child physical abuse. Key recommendations include:
- Mandatory skeletal survey for children <2 years with suspected abuse, and consideration for children up to 5 years.
- Ophthalmologic examination for retinal hemorrhages in suspected abusive head trauma.
- Head CT or MRI for suspected head trauma.
- Specific laboratory studies to rule out medical mimics.
- Importance of multidisciplinary team involvement (child abuse pediatrician, social worker, law enforcement).
-
American Academy of Orthopaedic Surgeons (AAOS) Position Statement: Child Abuse and Neglect (2018)
: This statement highlights the orthopedic surgeon's ethical and professional responsibility to recognize and report suspected child abuse. It emphasizes:
- The unique position of orthopedic surgeons as primary care providers for musculoskeletal injuries.
- The obligation to pursue a diligent diagnostic evaluation.
- The importance of interdisciplinary collaboration.
- The need for adequate training in NAI for orthopedic residents and practicing surgeons.
-
Radiological Society of North America (RSNA) / American College of Radiology (ACR) Appropriateness Criteria
: Provide evidence-based recommendations for imaging in suspected child abuse, detailing when specific imaging modalities (plain radiographs, CT, MRI, bone scan) are appropriate.
- Skeletal Survey : The gold standard for detecting fractures in NAI, especially occult and healing fractures.
- Bone Scan : Useful adjunct for identifying subtle rib fractures, metaphyseal lesions, or diaphyseal injuries not apparent on plain films, especially in children <1 year. However, it can miss skull fractures and some epiphyseal injuries.
- Child Abuse Prevention and Treatment Act (CAPTA) : Federal legislation in the United States that provides funding and guidance to states for child protective services and mandates reporting of child abuse and neglect. All healthcare professionals are mandated reporters.
- World Health Organization (WHO) Guidelines for the Prevention and Management of Child Maltreatment : Provides global perspectives and strategies for addressing child maltreatment, including physical abuse.
Key Literature Areas
- Epidemiology and Risk Factors : Studies identifying the incidence of NAI, particularly fracture patterns, and demographic risk factors (age, socioeconomic status, substance abuse in caregivers).
-
Specific Fracture Patterns
: Research detailing the specificity and sensitivity of metaphyseal corner fractures, posterior rib fractures, and other characteristic injuries for NAI.
- Specificity of MCFs : Highly specific, approaching 90-95% for NAI in the absence of a plausible accidental mechanism.
- Specificity of Posterior Rib Fractures : Also highly specific for NAI due to the forces required.
- Differentiation from Medical Mimics : Literature focusing on clinical and radiographic differentiation of NAI from osteogenesis imperfecta, rickets, and other metabolic bone diseases. Emphasizes the importance of genetic testing and biochemical workup in equivocal cases.
- Forensic Radiology : Articles on optimal techniques for skeletal surveys, interpretation of fracture dating, and the role of advanced imaging in forensic investigations.
- Long-Term Outcomes : Studies tracking the physical, psychological, and developmental outcomes of children who have experienced NAI, highlighting the critical need for early intervention and long-term support.
- Surgeon's Role and Reporting : Articles discussing the ethical dilemmas, legal responsibilities, and practical aspects of reporting suspected NAI for orthopedic surgeons.
In conclusion, the orthopedic surgeon serves as a critical frontline identifier of NAI. A comprehensive understanding of characteristic injury patterns, rigorous diagnostic protocols, and active participation in multidisciplinary teams are not just best practices, but ethical imperatives to protect vulnerable pediatric patients from recurrent harm. Continuous education and a high index of suspicion are indispensable tools in this vital mission.
