Introduction to Axillary Nerve Neurotization
The restoration of shoulder function following a devastating upper trunk brachial plexus injury (C5-C6) or an isolated axillary nerve palsy remains one of the most challenging paradigms in peripheral nerve surgery. The axillary nerve is critical for shoulder abduction, flexion, and external rotation, primarily through its innervation of the deltoid and teres minor muscles. When spontaneous recovery is deemed unlikely based on clinical and electrodiagnostic evaluation, surgical intervention is mandated.
Historically, nerve grafting from the proximal spinal nerves to the distal axillary nerve was the standard of care. However, the prolonged distance for axonal regeneration often resulted in suboptimal motor recovery due to irreversible motor endplate degradation. The paradigm shifted significantly with the popularization of regional nerve transfers (neurotization), specifically the transfer of a redundant motor branch of the radial nerve (typically the branch to the medial or long head of the triceps) directly to the axillary nerve.
Pioneered and refined by Mackinnon and Colbert, this technique dramatically reduces the regenerative distance, allowing axons to reach the target motor endplates in a fraction of the time required for traditional grafting. This comprehensive guide details the surgical anatomy, indications, step-by-step operative technique, and postoperative protocols for the radial-to-axillary nerve transfer, alongside concurrent procedures for global shoulder reinnervation.
Surgical Anatomy and Biomechanics
A profound understanding of the posterior shoulder anatomy, specifically the quadrangular space and the triceps interval, is paramount for the safe and effective execution of this procedure.
The Axillary Nerve and the Quadrangular Space
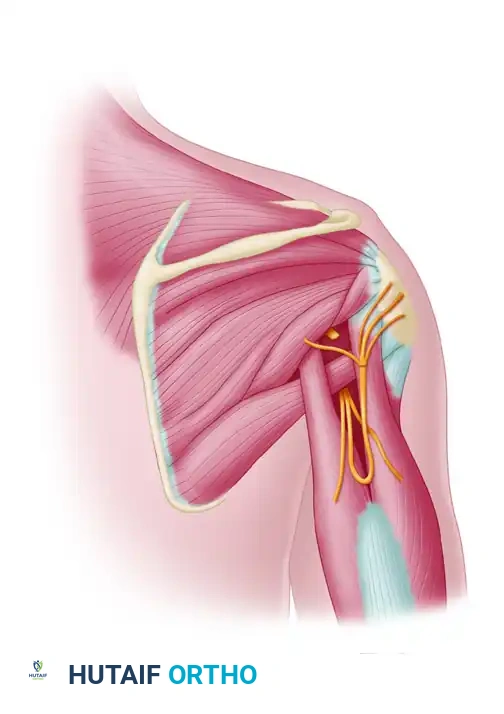
The axillary nerve arises from the posterior cord of the brachial plexus (C5, C6). It courses inferiorly and posteriorly to exit the axilla through the quadrangular space. The boundaries of this critical anatomical gateway are:
* Superior: Teres minor muscle (and the inferior capsule of the glenohumeral joint).
* Inferior: Teres major muscle.
* Medial: Long head of the triceps brachii.
* Lateral: Surgical neck of the humerus.
Within the quadrangular space, the axillary nerve travels alongside the posterior circumflex humeral artery and vein. Upon exiting the space, it divides into an anterior branch (supplying the anterior and middle deltoid) and a posterior branch (supplying the teres minor and posterior deltoid, and terminating as the superior lateral cutaneous nerve of the arm).
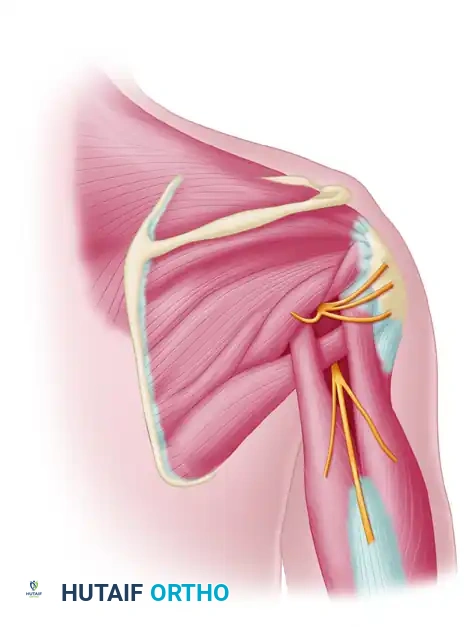
The Radial Nerve and Triceps Innervation
The radial nerve, the largest terminal branch of the posterior cord, provides multiple motor branches to the triceps brachii as it spirals around the posterior humerus. The triceps muscle is innervated by distinct branches to its long, lateral, and medial heads.
The branch to the medial head of the triceps is the preferred donor nerve for axillary neurotization. It is anatomically consistent, possesses a high density of motor axons, and its sacrifice does not result in a clinically significant loss of elbow extension power, as the long and lateral heads provide robust compensatory function.
🔪 Surgical Pearl: Donor Nerve Selection
While the branch to the medial head of the triceps is the classic donor, the branch to the long head may also be utilized depending on the specific branching pattern encountered intraoperatively and the required length for a tension-free coaptation. Preoperative clinical examination must confirm intact triceps function (MRC Grade 5) prior to selecting the radial nerve as a donor.
Preoperative Evaluation and Indications
Clinical Assessment
Patients typically present with profound weakness or complete paralysis of shoulder abduction and external rotation. Atrophy of the deltoid contour is often visible. A meticulous neurological examination must be performed to assess the integrity of potential donor nerves. Normal triceps strength (radial nerve, C7) is an absolute prerequisite for this specific transfer.
Electrodiagnostic Studies
Electromyography (EMG) and Nerve Conduction Studies (NCS) are essential. They confirm the diagnosis, localize the lesion (preganglionic vs. postganglionic), and establish a baseline. Serial EMGs over 3 to 6 months that show no nascent motor unit potentials in the deltoid strongly indicate the need for surgical exploration.
Timing of Surgery
Time is the most critical variable in peripheral nerve surgery. Motor endplates undergo irreversible fibrosis and degeneration if denervated for prolonged periods. Nerve transfers should ideally be performed between 3 and 6 months post-injury. Procedures attempted after 12 to 18 months yield significantly inferior functional outcomes.
Patient Positioning and Preparation
- Positioning: Place the patient in the prone position. Ensure all bony prominences are meticulously padded. The head should be supported in a neutral position using a specialized foam headrest or Mayfield tongs if concurrent cervical spine access is required (rare for this specific distal transfer).
- Arm Placement: The operative arm is draped free to allow for full mobility, passive range of motion, and intraoperative manipulation. It is typically rested on a radiolucent arm board.
- Anesthesia: General anesthesia is required. Crucially, long-acting paralytic agents must be avoided after induction to allow for intraoperative nerve stimulation.
Surgical Technique: Step-by-Step
1. Incision and Superficial Exposure
Make a longitudinal incision on the posterior aspect of the shoulder. The incision should begin at a point overlying the quadrangular space at the posterior border of the deltoid muscle and extend distally to the midposterior interval between the lateral and long heads of the triceps.
Carry the dissection sharply through the subcutaneous tissue down to the investing fascia of the triceps and deltoid muscles. Maintain meticulous hemostasis to ensure a clear microsurgical field later in the procedure.
2. Deep Dissection and Identification of the Quadrangular Space
Open the interval between the long and lateral heads of the triceps. This exposes the radial nerve and its accompanying profunda brachii vessels running on the posterior surface of the humerus within the spiral groove.
Retract the posterior border of the deltoid muscle superiorly and laterally. This maneuver is critical for visualizing the quadrangular space.
⚠️ Surgical Warning: The Cutaneous Branch
Often, the superior lateral cutaneous branch of the axillary nerve courses superficially and deep to the deltoid muscle. Identifying this sensory branch and tracing it proximally is a highly reliable method for locating the main trunk of the axillary nerve as it exits the quadrangular space.
Identify the transversely oriented tendinous portion of the teres major muscle, which is located deep to the long head of the triceps. This structure serves as the primary inferior anatomical landmark for the quadrangular space.

3. Identification of the Recipient Axillary Nerve
Using blunt dissection, explore the region superior to the teres major muscle. The axillary nerve will be found exiting the quadrangular space just superior to the posterior circumflex humeral vessels.
Once identified, use a handheld sterile nerve stimulator (typically set at 0.5 to 2.0 mA) to stimulate the axillary nerve. This step is mandatory to definitively confirm the lack of motor function and validate the indication for neurotization.
4. Identification and Preparation of the Donor Radial Nerve Branch
Return your attention to the exposed radial nerve in the triceps interval. Carefully dissect the epineurium to identify the individual motor branches.
Identify the nerve branch to the medial head of the triceps. This is a distinct branch that runs adjacent to the main trunk of the radial nerve. Use the nerve stimulator to confirm its identity; stimulation should elicit a robust, isolated contraction of the medial head of the triceps.
Once confirmed, trace the branch to the medial head as far distally as possible into the muscle belly to maximize donor nerve length. Divide the branch at its most distal point. Carefully neurolyse and isolate the donor nerve proximally up to the inferior border of the teres major muscle, ensuring it can be transposed superiorly without tethering.
5. Preparation of the Recipient Nerve
Sharply divide the proximal portion of the axillary nerve as it exits the quadrangular space. The transection should include the component branching to the teres minor muscle to ensure the entire distal axillary nerve trunk is available for coaptation.
Examine the cross-section of the distal axillary nerve under the operating microscope. Healthy fascicles should pout from the epineurium. If extensive intraneural fibrosis (scarring) is present, serial sectioning distally is required until healthy fascicular architecture is reached.
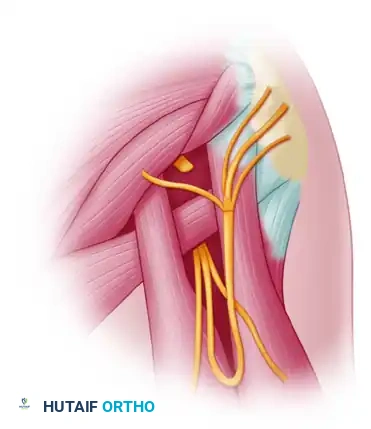
6. Microsurgical Coaptation
Transpose the proximal segment of the medial triceps nerve (donor) to meet the distal segment of the axillary nerve (recipient).
🔪 Surgical Pearl: Tension-Free Repair
The most critical factor in nerve repair is a completely tension-free coaptation. If tension exists, the limb must be repositioned, or further proximal neurolysis of the donor nerve must be performed. If tension cannot be relieved, an interpositional nerve graft (e.g., sural nerve) must be used, though this significantly downgrades the expected outcome.
Under the operating microscope, perform an epineurial repair using interrupted 9-0 or 8-0 nylon sutures. Typically, 4 to 6 sutures are sufficient to align the fascicles and secure the epineurium. Fibrin glue may be applied circumferentially around the repair site to augment the coaptation and prevent axonal escape.
Comprehensive Shoulder Reinnervation: Concurrent Suprascapular Nerve Transfer
In cases of upper trunk (C5-C6) brachial plexus injuries, restoring the axillary nerve alone is insufficient for functional shoulder abduction. The suprascapular nerve, which innervates the supraspinatus and infraspinatus muscles, must also be reconstructed to initiate abduction and provide dynamic glenohumeral stability.
The most common concurrent procedure is the transfer of the distal Spinal Accessory Nerve (CN XI) to the Suprascapular Nerve.
Technique for Accessory to Suprascapular Transfer
- Approach: Extend the surgical field superiorly. Use blunt dissection and a nerve stimulator at a deep level to the trapezius muscle, working in a longitudinal direction to identify the spinal accessory nerve.
- Identification: Once the accessory nerve is identified and confirmed intact by stimulation (eliciting trapezius contraction), dissect it as far distally or inferiorly as possible.
- Suprascapular Nerve Exposure: Identify the suprascapular nerve as it courses toward the suprascapular notch.
- Preparation: Adequate dissection of both the suprascapular and accessory nerves allows for a direct transfer. Divide the suprascapular nerve proximally (near its origin from the upper trunk) and the accessory nerve distally.
- Coaptation: Suture the proximal end of the accessory nerve to the distal end of the suprascapular nerve with interrupted 9-0 nylon under an operating microscope. This tension-free repair rarely requires a nerve graft if mobilized correctly.
Note: Entrapment of the suprascapular nerve can also occur distally at the spinoglenoid notch, affecting only the infraspinatus fossa. Electrodiagnostic studies are helpful in confirming the exact level of the lesion prior to surgical planning.
Postoperative Care and Rehabilitation Protocol
The success of a nerve transfer relies heavily on meticulous postoperative protection and specialized neurological rehabilitation.
Phase I: Protection (Weeks 0-2)
- Immobilization: The patient is placed in a shoulder immobilizer or sling postoperatively. The primary goal is to prevent shoulder abduction and external rotation, which could place catastrophic tension on the axillary nerve repair.
- Elbow Management: Care is taken to allow gentle, intermittent elbow range of motion. This prevents elbow stiffness and mitigates ulnar nerve irritation, while ensuring no traction is transmitted to the triceps donor site.
Phase II: Passive and Active-Assisted ROM (Weeks 2-6)
- Shoulder ROM: Gentle, passive shoulder range of motion exercises are initiated at 2 weeks to prevent adhesive capsulitis. Abduction is strictly limited to 45 degrees initially, gradually increasing based on the surgeon's assessment of repair tension.
- Avoidance: Active triceps extension against resistance is avoided to protect the donor nerve stump.
Phase III: Motor Reeducation and Strengthening (Months 3+)
- Cortical Plasticity: Because a nerve that previously extended the elbow (triceps) is now connected to a muscle that abducts the shoulder (deltoid), the patient must undergo motor reeducation. Patients are instructed to "think about extending the elbow" while attempting to abduct the shoulder.
- Strengthening: True strengthening exercises are delayed until clinical or electromyographic evidence of deltoid (and supraspinatus, if concurrent transfer was performed) function returns. This typically begins between 4 to 6 months postoperatively.
- Over time, through neuroplasticity, the brain remaps the motor cortex, and the patient will be able to abduct the shoulder spontaneously without consciously firing the triceps.
Complications and Pitfalls
- Failure of Axonal Regeneration: The most devastating complication is a lack of motor recovery. This can occur due to delayed surgical intervention (fibrosed motor endplates), tension at the repair site, or severe proximal injury extending further distally than anticipated.
- Triceps Weakness: While the long and lateral heads usually compensate, some patients may experience a transient or mild permanent decrease in peak elbow extension torque. This must be discussed during preoperative informed consent.
- Neuroma Formation: A painful neuroma can form at the coaptation site if axonal escape occurs, highlighting the importance of meticulous microsurgical technique and the potential use of fibrin glue or nerve wraps.
- Joint Stiffness: Prolonged immobilization can lead to severe glenohumeral stiffness. A delicate balance between protecting the nerve repair and initiating early passive motion is required.
