DEFINITION
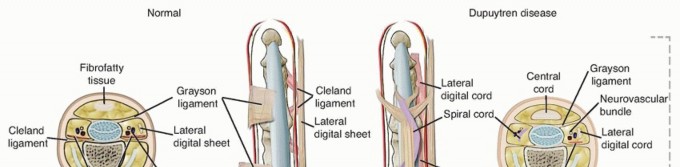
Dupuytren disease (DD) is a benign, generally painless, fibroproliferative disorder affecting the palmar fascia that often leads to progressive contractures of the fingers and thumb (FIG 1). These contractures can be severe having a significant impact on hand function.Although most estimates give the incidence of DD as 3% to 6% of Caucasians, some studies havereported rates as high as 42%.46 This would mean that as many as 13.5 to 27 million people in the United States and Europe could be affected.
ANATOMY




PATHOGENESIS
AZ19transcription factor gene increases the potency of TGF-β1.Multiple other proteins influence differentiation, growth, and contractility of myofibroblasts. These include platelet-derived growth factor (PDGF), fibroblast growth factor (FGF), epidermal growth factor (EGF), interleukin-1 (IL-1) tenascin and periostin (Tables 1 and 2).10,49
NATURAL HISTORY
DD progresses through three clinical stages15,42:Stage I : the proliferative or nodular stage. In this stage, patients have a nodule or nodules within the palmar fascia. The nodules are predominantly cellular, composed of peripheral, perivascular spindle-shaped hyperplastic fibroblasts with irregular hyperchromatic nuclei. The nodules tend to be vascular with reactivetissue around the periphery. There is no increase in collagen deposition. The hyperplastic cells disrupt the continuity of the normal palmar fascia. Table 1 Selected Genes and Proteins Upregulated in Dupuytren Disease From Black EM, Blazar PE. Dupuytren disease: an evolving understanding of an age-old disease. J Am Acad Orthop Surg 2011;19(12):746-757.A disintegrin and metalloproteinase domain (ADAM) 12 Alpha smooth muscle actin (α-SMA)β-1 integrinCadherin 11 (CDH11)Collagen I, collagen V, collagen VIII Contactin 1 (CNTN1)FibronectinHeat shock protein 47 (HSP47) LamininLeucine-rich repeat (LRR) domain-containing 17V-maf musculoaponeurotic fibrosarcoma oncogene homolog B (MafB) Periostin, osteoblast specific factor (POSTN)Postsynaptic density protein-95 (PSD-95) Tenascin CTissue inhibitor of metalloproteinase (TIMP-1) Transforming growth factor-β2 (TGF-β2) Zonula occludens-1 protein (ZO-1)Stage II : the involutional or active disease stage. In this stage, there is nodular thickening of the palmar fascia with the beginning of joint contracture. Fibroblasts align themselves along lines of stress. They become more mature and decrease in size and number. The predominate cell type is myofibroblast. There are definite cords composed of well-aligned, mature collagen fibers and few scattered cells.Stage III : the residual or advanced disease stage. In this stage, there are diffuse, thick fibrotic cords that become more contracted. The cords are predominantly collagen with few cells that are elongated and compressed by the collagen fibers. Cell types are both fibroblasts and myofibroblasts. Table 2 Selected Genes and Proteins Downregulated in Dupuytren Disease Chitinase 3-like protein 2 Collagen XVCornea-derived transcript 6 (CDT6) Cysteine dioxygenase 1 (CDO1) Matrix metallopeptidase 27 (MMP27) Matrix metalloproteinase-3 (MMP3) Superoxide dismutase (SOD) Superoxide dismutase 2 (SOD2)From Black EM, Blazar PE. Dupuytren disease: an evolving understanding of an age-old disease. J Am Acad Orthop Surg 2011;19(12):746-757.P.1210The progression of DD is unpredictable. Nodules may lay dormant for years without progression or canprogress rapidly over a matter of months.42 Reilly et al57 reported on 59 patients with Dupuytren nodules. Thirty of the 59 patients had developed a cord at an average of 8.7 years (range 6 to 15 years). However, by8.7 years only, 5 patients met the criteria for surgery and 7 patients had regressed.57
PATIENT HISTORY AND PHYSICAL FINDINGS



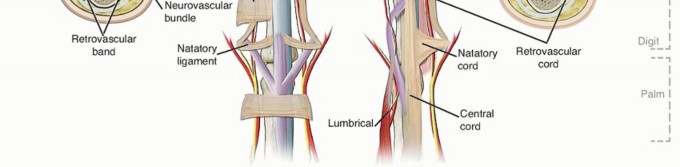
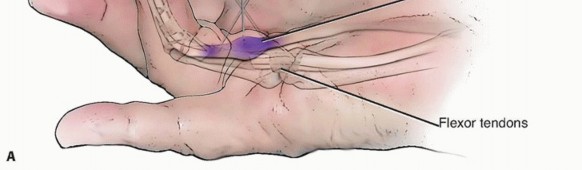
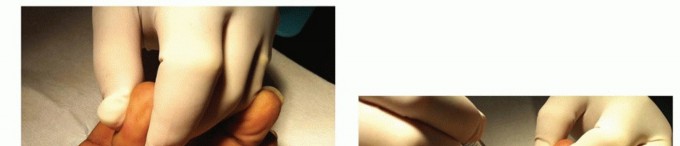
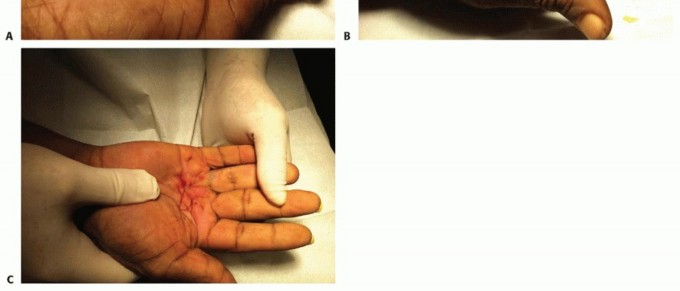
DD is associated with a number of medical conditions including diabetes mellitus,3,13 HIV11 frozen shoulder, a high lipid profile,29 and epilepsy.2It has also been associated with lifestyle risk factors including smoking, alcoholism,12,24,25 manual labor,41 hand and wrist trauma,40 and the use of vibratory tools.64DD usually begins as painless nodules in the palm. The most common finger involved is the ring finger (60.7%), followed by the small finger (51%), the middle finger (22.5%), the thumb (7.0%), and the index finger(5.8%). The thumb web can also be involved resulting in an adduction contracture (FIG 3A).55Early in the disease, patients may note thickening of the skin with pitting or dimpling. This may progress to cords that can ultimately lead to contracture of the metacarpophalangeal (MP) and PIP joints (FIG 3B).DD usually begins with one finger but often progresses to others (FIG 3C).DD can also occur in ectopic locations such as over the dorsum of the PIP joints (Garrod nodes), in the feet (Lederhose disease), and in the penis (Peyronie disease).30Five factors have been identified that indicate a DD diathesis. They include onset younger than age 50 years, bilateral involvement, ectopic lesions, male gender, and a positive family history.30,33P.1211Patients with a DD diathesis have a more aggressive disease with higher rates of recurrence.The “fasciodesis” maneuver is useful for predicting minimum gain in PIP motion after percutaneous needle fasciotomy (PNF).Flex the MP joint to 90 degrees.Measure the extension gain at the PIP joint.20Tubiana classified DD based on total passive extension deficit (TPED) of the MP, PIP, and distal interphalangeal (DIP) joints (Table 3).65
IMAGING AND OTHER DIAGNOSTIC STUDIES
In most instances, radiographic imaging is not necessary to adequately evaluate DD. The only time one might consider imaging is if there is a concern for some other pathology such as significant osteoarthritis or neoplasm. If these are suspected, then appropriate imaging studies could be ordered.
DIFFERENTIAL DIAGNOSIS
The differential diagnosis of DD is well covered in the chapter on Surgical Treatment of Dupuytren's Disease.
NONOPERATIVE MANAGEMENT
In the past, a number of nonoperative treatments for DD have met with limited success. These include physical therapy, splinting, dimethylsulfoxide injections, topical vitamins A and E, gamma interferon injections,radiation, and the calcium channel blockers such as nifedipine and verapamil.56In 1971, Hueston33 performed what he referred to asenzymatic fasciotomy.He injected patients with a mixture of trypsin, hyaluronidase, and lidocaine, followed by a forcible extension maneuver. He was able toobtain full extension of all fingers 15 minutes following injection.33 Table 3 Tubiana Grades of Dupuytren Disease Based on Total Passive Extension Deficit Grade I0-45 degreesGrade II45-90 degreesGrade III90-135 degreesGrade IV ≥135 degreesWhen McCarthy43 studied the long-term results, however, he found that seven of nine patients had developed recurrence within 2 to 3 years.Injection of triamcinolone acetonide directly into the DD nodules resulted in regression in 97% of patients. The average number of injections was 3.2. There was a 50% recurrence rate between 1 and 3 years after the last injection, however.38
COLLAGENASE _CLOSTRIDIUM HISTOLYTICUM_(XIAFLEX)
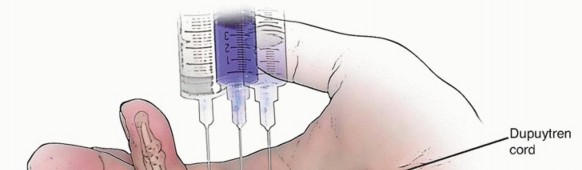
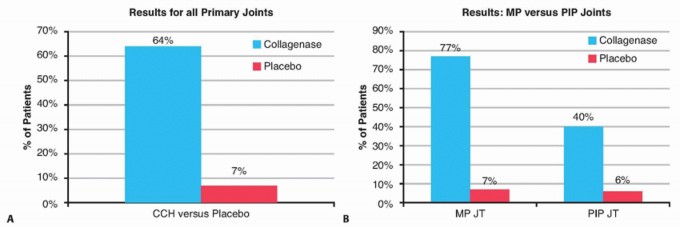
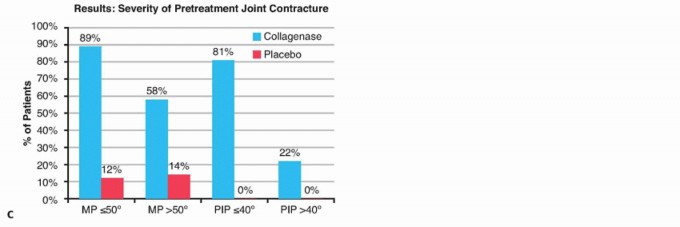
In 2009, Hurst et al34 reported the results of the multicenter collagenase option for reduction of Dupuytren (CORD) I study. This was a double blind, placebo-controlled study in which they injected Dupuytren cords with0.58 mg collagenaseClostridium histolyticum(CCH) (Xiaflex).34Xiaflex is a mixture of two synergistic collagenases that tend to rapidly degrade type I and type III collagens.61
INDICATIONS FOR TREATMENT
A palpable cord with an MP or PIP joint contracture of 20 degrees or more
CONTRAINDICATIONS
Patients who are intolerant of pain are poor candidates.The drug is expensive and patients with multiple cords may face months of treatment and a great deal of expense.A history of sensitivity to CCH.Patients who have been on anticoagulants other than low-dose aspirin within 7 days of CCH injection Contractures associated with huge nodules are not good candidates for collagenase.
PREOPERATIVE PLANNING
Give the patient take-home information describing common side effects and risks. Be sure to obtain insurance preauthorization if required.Identify the primary cord for treatment.Identify secondary and tertiary joints for later treatment.
TECHNIQUE
INJECTION28****



Coleman et al16 reported on injecting cords affecting two joints in the same hand at one sitting. Although there was an increased incidence of some adverse events, few were serious and the authors concluded it was safe to perform.16Each cord can be injected up to three times at 30-day intervals.1. ManipulationThe day following the injection, patients return for manipulation. Manipulation may be safely performed up to 7 days following injection without negatively affecting the results (TECH FIG 4).28,37Prior to manipulation, perform a wrist or digital nerve block with 1% lidocaine.The wrist is flexed and moderate passive extension is applied to the involved digit for 10 to 20 seconds. If manipulating the PIP joint, the MP joint is flexed.Often, a “pop” or tearing noise is heard as the cord breaks. Some cords rupture spontaneously.Up to three attempts at 5- to 10-minute intervals can be made.If unsuccessful after three attempts, the patient should be instructed to return in 30 days for another injection. P.1214
PEARLS AND PITFALLS


POSTOPERATIVE CARE
Following the injection of CCH, a light compressive dressing is applied. Patients are told to remove the dressing either that evening or the next day.Although some authors do not prescribe pain medication, I prefer to give patients a prescription for a few narcotic pain pills for the first few days.Patients are advised to avoid heavy use of their hand until the next day.Following manipulation, patients are given a home exercise program and a night splint that holds the fingers in extension. They are told to wear the splint at night for 3 to 4 months.For severe PIP joint contractures (≥40 degrees), patients are given a dynamic extension splint and told to wear it full time for 3 to 4 months except for bathing and exercise.Patients are advised to avoid heavy use of their hand until pain-free.
OUTCOMES

COMPLICATIONS4,51,52****






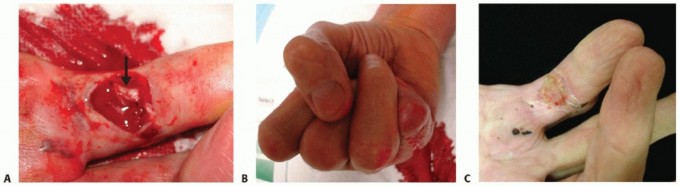
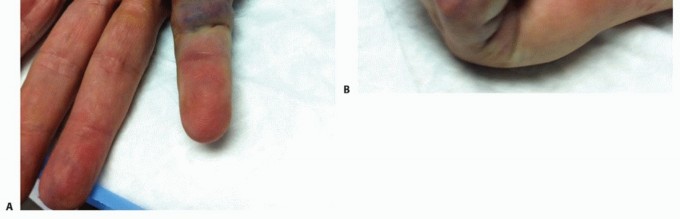
Drug ineffective (6.1%)Extremity pain (4.6)%Lymphadenopathy (elbow/axilla) (3.1%) (FIG 10A,B) Hematoma (2.8%)Injection site pain (2.7%)Injection site hematoma (2.8%) (FIG 11A,B) Flexor tendon rupture (0.05%)Ring finger MP joint (four reports) Little finger MP joint (five reports) Little finger PIP joint (eight reports)Complex regional pain syndrome (CRPS) (two reports) A2 pulley injury (one report)Stretch neurapraxia (one report) Flexor pulley injury (one report)Loss of a well-established skin graft (one report)62 Pruritus or localized rash
SURGICAL MANAGEMENT
Sir Astley Cooper originally performed percutaneous fasciotomy in 1822 using a bistoury later known as aCooper knife. The procedure came to be known asCooper fasciotomy.18,36,66In 1979, two French rheumatologists, Lermusiaux and Debeyre,39 popularized using a 25-gauge needle to perform PNF.
INDICATIONS FOR TREATMENT18,20****


P.1218
CONTRAINDICATIONS20****
Large, bulky ill-defined cord (relative) Patients without a distinct, palpable cord19 Recurrent cord after surgery (relative)Patients unable to tolerate local proceduresA cord that allows for full passive finger extension Uncooperative or mentally impaired patients Nodules without cordsLong-standing PIP flexion contractures (relative) Deep lateral cordsContractures resulting from insufficient skin or postsurgical scarring
PREOPERATIVE PLANNING

POSITIONING
The patient is supine with the hand resting on a hand table.A 2-inch thick pad of folded towels is placed behind the hand to facilitate MP extension.19 The hand is draped with sterile drapes.
APPROACH




TECHNIQUE
COLLAGENASE INJECTION

Alternately, use the needle in a sawing motion.With either technique, there should be a grating feeling. If a grating is not felt, change the needle and move to another portal.Following the perforations, the finger is firmly but gently extended while stabilizing the hand. Frequently, a pop is heard as the cord breaks (TECH FIG 5C).Flex the wrist and ask the patient to actively extend the finger during the manipulation maneuver. Extend the finger and palpate for a residual cord.Repeat the procedure as necessary until full extension is achieved, the remaining cord is no longer palpable, or further treatment would put the neurovascular bundles at risk.A local or wrist block may be helpful if the manipulation is too painful.Injecting triamcinolone acetonide (TA) into the portals and nodules following release may be helpful.McMillan and Bidhammer45 reported significantly improved correction of deformity at 6 months in patients who received TA injection postoperatively.P.1220
PEARLS AND PITFALLS
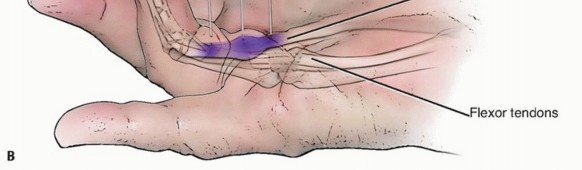
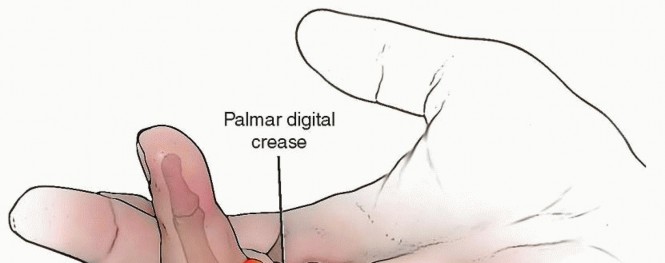
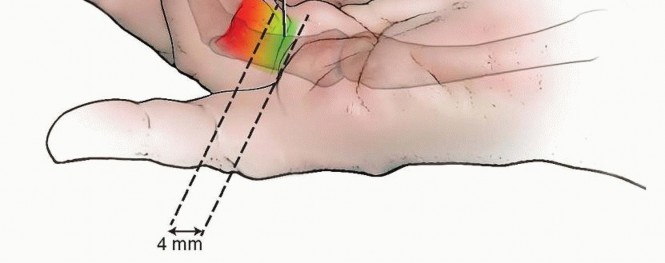
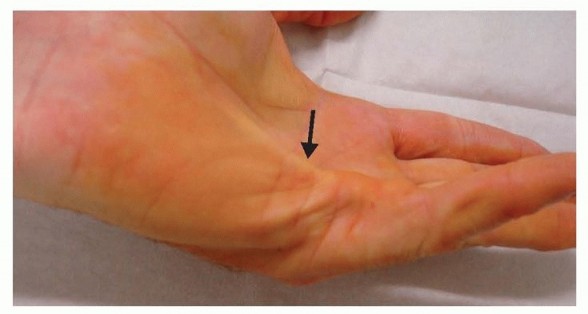
A spiral nerve can be predicted with 90% reliability if there is a soft, pulpy mass of skin lying between the distal palmar crease and the proximal finger crease.60If this soft, pulpy mass is present, perform the fasciotomy proximally at the level of the transverse fibers only.20Patients will report a strong electrical shock sensation if the nerve is touched.If the fingertip becomes numb from the use of local anesthetic, move to a more proximal portal.19Traction on the skin or nodule is safer than pulling on the fingertips. The flexor tendons should remain relaxed.Repeatedly check for nerve or tendon involvement during the procedure.Change to a fresh needle and new portal if you no longer feel a grating sensation.
POSTOPERATIVE CARE
A Band-Aid or light dressing covers the wound for 24 hours. Ice and elevate the hand for 48 hours.Avoid strenuous gripping for 1 week.Skin tears are treated with a light dressing and local wound care until healed. Patients are instructed to avoid painful activity.Postoperative therapy is rarely necessary. A night splint is worn for 1 month.47
OUTCOMES
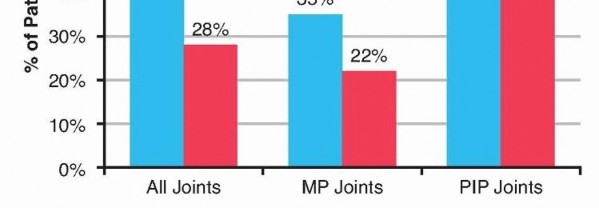
Patients with diseases such as rheumatoid arthritis, and diabetes, anticoagulant therapy or a history of previous CRPS are bad prognostic factors for treatment.Foucher reported follow-up at 3.2 years.21,22 MP joint motion improved by 79%PIP motion improved by 65%Recurrence of DD occurred in 58% of patients and 24% required additional treatment.PNF has been compared to limited fasciectomy (LF).66TPED improved 63% in the PNF group and 79% in the LF group.LF recovery took from 21 to 58 days. Most PNF patients are using their hands optimally within 1 week. Poor outcomes are reported in patients with Tubiana stage III and IV DD.Pess et al54 reported initial correction of contractures of 99% at the MP joint and 89% at the PIP joint with PNF. Final follow-up was a minimum of 3 years and the correction was maintained in 72% of the MPjoints and 31% of the PIP joints.54Five-year follow-up recurrence rates have been reported to be 84.9% for PNF compared to 20.9% for LF.67Comparison of PNF and collagenase demonstrate similar clinical outcomes in the short term.48Cost analysis comparing LF, PNF, and CCH demonstrate LF is not cost effective. PNF is cost effective if the success rate is high. CCH is cost effective if the cost per injection is significantly less than currently priced in the United States.8,14,17,59
COMPLICATIONS
Vascular injury Nerve laceration InfectionSkin tears Paresthesias CRPS type IIncreased postoperative pain requiring analgesics False aneurysm63FDP injury (0.05%)63
REFERENCES
- Anthony SG, Lozano-Calderon SA, Simmons BP, et al. Gender ratio of Dupuytren's disease in the modernU.S. population. Hand 2008; 3(2):87-90.
- Arafa M, Noble J, Royle SG, et al. Dupuytren's and epilepsy revisited. J Hand Surg Br 1992;17(2):221-224.
- Arkkila PE, Koskinen PJ, Kantola IM, et al. Dupuytren's disease in type I diabetic subjects: investigation of biochemical markers of type III and I collagen. Clin Exp Rheumatol 2000;18(2):215-219.
- Badalamente MA, Hurst LC. Efficacy and safety of injectable mixed collagenase subtypes in the treatment of Dupuytren's contracture. J Hand Surg Am 2007;32(6):767-774.
- Badalamente MA, Hurst LC, Sampson SP. Prostaglandins influence myofibroblast contractility in Dupuytren's disease. J Hand Surg Am 1988;13(6):867-871.
- Badalamente MA, Sampson SP, Hurst LC, et al. The role of transforming growth factor beta in Dupuytren's disease. J Hand Surg Am 1996; 21(2):210-215.
- Balaguer T, David S, Ihrai T, et al. Histological staging and Dupuytren's disease recurrence or extensionafter surgical treatment: a retrospective study of 124 patients. J Hand Surg Eur Vol 2009;34(4): 493-496.
- Baltzer H, Binhammer PA. Cost-effectiveness in the management of Dupuytren's contracture. A Canadian cost-utility analysis of current and future management strategies. Bone Joint J 2013;95-B(8): 1094-1100.
- Bisson MA, Beckett KS, McGrouther DA, et al. Transforming growth factor-beta1 stimulation enhances Dupuytren's fibroblast contraction in response to uniaxial mechanical load within a 3-dimensional collagen gel. J Hand Surg Am 2009;34(6):1102-1110.
- Black EM, Blazar PE. Dupuytren disease: an evolving understanding of an age-old disease. J Am Acad Orthop Surg 2011;19(12): 746-757.
- Bower M, Nelson M, Gazzard BG. Dupuytren's contractures in patients infected with HIV. BMJ 1990;300(6718):164-165.
- Burge P, Hoy G, Regan P, et al. Smoking, alcohol and the risk of Dupuytren's contracture. J Bone Joint Surg Br 1997;79(2):206-210.
- Cagliero E, Apruzzese W, Perlmutter GS, et al. Musculoskeletal disorders of the hand and shoulder in patients with diabetes mellitus. Am J Med 2002;112(6):487-490.
- Chen NC, Shauver MJ, Chung KC. Cost-effectiveness of open partial fasciectomy, needle aponeurotomy, and collagenase injection for dupuytren contracture. J Hand Surg Am 2011;36(11):1826-1834.e1832.
- Chiu HF, McFarlane RM. Pathogenesis of Dupuytren's contracture: a correlative clinical-pathological study. J Hand Surg Am 1978;3(1): 1-10.
- Coleman S, Gilpin D, Kaplan FT, et al. Efficacy and safety of concurrent collagenase clostridium histolyticum injections for multiple Dupuytren contractures. J Hand Surg Am 2014;39(1):57-64.P.1221
- De Salas-Cansado M, Cuadros M, Del Cerro M, et al. Budget impact analysis in Spanish patients with Dupuytren's contracture: fasciectomy vs. collagenase Clostridium histolyticum. Chir Main 2013;32(2): 68-73.
- Diaz R, Curtin C. Needle aponeurotomy for the treatment of Dupuytren's disease. Hand Clin 2014;30(1):33-38.
- Eaton C. Percutaneous fasciotomy for Dupuytren's contracture. J Hand Surg Am 2011;36(5):910-915.
- Foucher G, Medina J, Malizos K. Percutaneous needle fasciotomy in dupuytren disease. Tech Hand Up Extrem Surg 2001;5(3):161-164.
- Foucher G, Medina J, Navarro R. Percutaneous needle aponeurotomy. Complications and results [in French]. Chir Main 2001;20(3): 206-211.
- Foucher G, Medina J, Navarro R. Percutaneous needle aponeurotomy: complications and results. J Hand Surg Br 2003;28(5):427-431.
- Gabbiani G, Majino G. Dupuytren's contracture: fibroblast contraction? An ultrastructural study. Am J Pathol 1972;66:131-138.
- Godtfredsen NS, Lucht H, Prescott E, et al. A prospective study linked both alcohol and tobacco to Dupuytren's disease. J Clin Epidemiol 2004;57(8):858-863.
- Gudmundsson KG, Arngrimsson R, Jonsson T. Dupuytren's disease, alcohol consumption and alcoholism. Scand J Prim Health Care 2001; 19(3):186-190.
- Hay DC, Louie DL, Earp BE, et al. Surgical findings in the treatment of Dupuytren's disease after initial treatment with clostridial collagenase (Xiaflex). J Hand Surg Eur Vol 2013;39(5):463-465.
- Hayton MJ, Bayat A, Chapman DS, et al. Isolated and spontaneous correction of proximal interphalangeal joint contractures in Dupuytren's disease: an exploratory analysis of the efficacy and safety of collagenase collagenase Clostridium histolyticum. Clin Drug Investig 2013;33(12):905-912.
- Hentz VR. Collagenase injections for treatment of Dupuytren disease. Hand Clin 2014;30(1):25-32.
- Hindocha S, John S, Stanley JK, et al. The heritability of Dupuytren's disease: familial aggregation and its clinical significance. J Hand Surg Am 2006;31(2):204-210.
- Hindocha S, Stanley JK, Watson S, et al. Dupuytren's diathesis revisited: evaluation of prognostic indicators for risk of disease recurrence. J Hand Surg Am 2006;31(10):1626-1634.
- Hotchkiss RN, Peimer CA, Coleman SG, et al. Recurrence of Dupuytren contracture after nonsurgical treatment with collagenase Clostridium histolyticum: summary of 4-year CORDLESS data. Presented at the 68th Annual Meeting of the American Society for Surgery of the Hand, October 3-5, 2010, San Francisco, CA.
- Hu FZ, Nystrom A, Ahmed A, et al. Mapping of an autosomal dominant gene for Dupuytren's contracture to chromosome 16q in a Swedish family. Clin Genet 2005;68(5):424-429.
- Hueston JT. Enzymatic fasciotomy. Hand 1971;3(1):38-40.
- Hurst LC, Badalamente MA, Hentz VR, et al. Injectable collagenase clostridium histolyticum for Dupuytren's contracture. N Engl J Med 2009;361(10):968-979.
- Hurst LC, Badalamente MA, Makowski J. The pathobiology of Dupuytren's contracture: effects of prostaglandins on myofibroblasts. J Hand Surg Am 1986;11(1):18-23.
- Hutchison RL, Rayan GM. Astley Cooper: his life and surgical contributions. J Hand Surg Am2011;36(2):316-320.
- Kaplan FT, Badalemente M, Hurst L, et al. Delayed manipulation following clostridial collagenase histolyticum injection for Dupuytren contracture. Presented at the 68th Annual Meeting of the American Society for Surgery of the Hand, October 3-5, 2013, San Francisco, CA.
- Ketchum LD, Donahue TK. The injection of nodules of Dupuytren's disease with triamcinolone acetonide. J Hand Surg Am 2000; 25(6):1157-1162.
- Lermusiaux J, Debeyre N. Le traitement médical de la maladie de Dupuytren. In: De Seze S, Ryckewaert A, Kahn MF, et al, eds. L' Actualité Rhumatologique. Paris, France: Expansion Scientifique, 1979: 338-343.
- Logan AJ, Mason G, Dias J, et al. Can rock climbing lead to Dupuytren's disease? Br J Sports Med 2005;39(9):639-644.
- Lucas G, Brichet A, Roquelaure Y, et al. Dupuytren's disease: personal factors and occupational exposure. Am J Ind Med 2008;51(1):9-15.
- Luck JV. Dupuytren's contracture; a new concept of the pathogenesis correlated with surgical management. J Bone Joint Surg Am 1959; 41-A(4):635-664.
- McCarthy DM. The long-term results of enzymic fasciotomy. J Hand Surg Br 1992;17(3):356.
- McFarlane RM. Patterns of the diseased fascia in the fingers in Dupuytren's contracture. Displacement of the neurovascular bundle. Plast Reconstr Surg 1974;54(1):31-44.
- McMillan C, Binhammer P. Steroid injection and needle aponeurotomy for Dupuytren contracture: a randomized, controlled study. J Hand Surg Am 2012;37(7):1307-1312.
- Medjoub K, Jawad A. The use of multiple needle fasciotomy in Dupuytren disease: retrospective observational study of outcome and patient satisfaction. Ann Plast Surg 2014;72(4):417-422.
- Meinel A. Long-term static overnight extension splinting following percutaneous needle fasciotomy [in German]. Handchir Mikrochir Plast Chir 2011;43(5):286-288.
- Nydick JA, Olliff BW, Garcia MJ, et al. A comparison of percutaneous needle fasciotomy and collagenase injection for dupuytren disease. J Hand Surg Am 2013;38(12):2377-2380.
- O'Gorman DB, Vi L, Gan BS. Molecular mechanisms and treatment strategies for Dupuytren's disease. Ther Clin Risk Manag 2010;6: 383-390.
- Peimer CA, Blazar P, Coleman S, et al. Dupuytren contracture recurrence following treatment with collagenase clostridium histolyticum (CORDLESS study): 3-year data. J Hand Surg Am 2013;38(1): 12-22.
- Peimer CA, McGoldrick CA, Fiore GJ. Nonsurgical treatment of Dupuytren's contracture: 1-year US post-marketing safety data for collagenase clostridium histolyticum. Hand 2012;7(2):143-146.
- Peimer CA, McGoldrick CA, Kaufman G. Nonsurgical treatment of dupuytren contracture: 3-year safety results using collagenaseClostridium histolyticum. Presented at the 68th Annual Meeting of the American Society for Surgery of the Hand, October 3-5, 2013, San Francisco, CA.
- Peimer CA, Skodny P, Mackowiak JI. Collagenase clostridium histolyticum for dupuytren contracture: patterns of use and effectiveness in clinical practice. J Hand Surg Am 2013;38(12):2370-2376.
- Pess GM, Pess RM, Pess RA. Results of needle aponeurotomy for Dupuytren contracture in over 1,000 fingers. J Hand Surg Am 2012; 37(4):651-656.
- Rayan GM. Clinical presentation and types of Dupuytren's disease. Hand Clin 1999;15(1):87-96, vii.
- Rayan GM, Parizi M, Tomasek JJ. Pharmacologic regulation of Dupuytren's fibroblast contraction in vitro. J Hand Surg Am 1996; 21(6):1065-1070.
- Reilly RM, Stern PJ, Goldfarb CA. A retrospective review of the management of Dupuytren's nodules. J Hand Surg Am 2005;30(5): 1014-1018.
- Rombouts JJ, Noel H, Legrain Y, et al. Prediction of recurrence in the treatment of Dupuytren's disease: evaluation of a histologic classification. J Hand Surg Am 1989;14(4):644-652.
- Sanjuan Cerveró R, Franco Ferrando N, Poquet Jornet J. Use of resources and costs associated with the treatment of Dupuytren's contracture at an orthopedics and traumatology surgery department in Denia (Spain): collagenase clostridium hystolyticum versus subtotal fasciectomy. BMC Musculoskelet Disord 2013;14:293.
- Short WH, Watson HK. Prediction of the spiral nerve in Dupuytren's contracture. J Hand Surg Am 1982;7(1):84-86.
- Starkweather KD, Lattuga S, Hurst LC, et al. Collagenase in the treatment of Dupuytren's disease: an in vitro study. J Hand Surg Am 1996;21(3):490-495.
- Swanson JW, Watt AJ, Vedder NB. Skin graft loss resulting from collagenase clostridium histolyticum treatment of Dupuytren contracture: case report and review of the literature. J Hand Surg Am 2013;38(3):548-551.
- Symes T, Stothard J. Two significant complications following percutaneous needle fasciotomy in a patient on anticoagulants. J Hand Surg Br 2006;31(6):606-607.
- Thomas PR, Clarke D. Vibration white finger and Dupuytren's contracture: are they related? Occup Med 1992;42(3):155-158.P.1222
- Tubiana R. Surgical management. In: Tubiana R, ed. The Hand. Philadelphia: WB Saunders Company, 1999:480.
- van Rijssen AL, Gerbrandy FS, Ter Linden H, et al. A comparison of the direct outcomes of percutaneous needle fasciotomy and limited fasciectomy for Dupuytren's disease: a 6-week follow-up study. J Hand Surg Am 2006;31(5):717-725.
- van Rijssen AL, ter Linden H, Werker PM. Five-year results of a randomized clinical trial on treatment in Dupuytren's disease: percutaneous needle fasciotomy versus limited fasciectomy. Plast Reconstr Surg 2012;129(2):469-477.
- van Rijssen AL, Werker PM. Percutaneous needle fasciotomy for recurrent Dupuytren disease. J Hand Surg Am 2012;37(9): 1820-1823.
- Verjee LS, Midwood K, Davidson D, et al. Myofibroblast distribution in Dupuytren's cords: correlation with digital contracture. J Hand Surg Am 2009;34(10):1785-1794.
