Comprehensive Introduction and Patho-Epidemiology
Histopathological Distinctions
The condition universally referred to as Morton’s neuroma represents one of the most frequently encountered etiologies of forefoot pain in the adult population. However, from a strict histopathological standpoint, the nomenclature is fundamentally a misnomer. A primary interdigital neuroma is not a neoplastic process, nor does it represent the haphazard, disorganized proliferation of axonal tissue characteristic of a traumatic amputation stump neuroma. Rather, the primary lesion is most accurately classified as an interdigital perineural fibrosis. The pathophysiology is driven by chronic, repetitive microtrauma and mechanical impingement of the common digital nerve as it courses beneath the unyielding deep transverse metatarsal ligament. This mechanical insult initiates a cascade of localized inflammatory and fibrotic changes, primarily localized to the epineurium and perineurium.
Microscopic analysis of excised primary specimens consistently reveals profound perineural fibrosis, endoneurial edema, and varying degrees of axonal demyelination and degeneration. Notably, inflammatory infiltrates are typically absent in chronic specimens, replaced instead by dense, hyalinized connective tissue and the presence of Renaut bodies—whorls of perineurial cells that indicate chronic nerve compression. Furthermore, the accompanying common digital artery frequently demonstrates significant pathological alterations, including intimal hyperplasia and thrombosis, suggesting a concomitant ischemic component to the nerve’s degeneration. Understanding this histopathology is paramount for the operating surgeon, as it underscores the necessity of addressing the mechanical entrapment (the transverse metatarsal ligament) in addition to resecting the diseased neural tissue.
Conversely, the "recurrent" interdigital neuroma represents an entirely distinct pathological entity. When a patient presents with recurrent, intractable pain following a previous excision, the underlying lesion is typically a true histopathologic amputation stump neuroma. This occurs when the proximal nerve stump, transected during the index procedure, fails to retract sufficiently into the protective environment of the intrinsic foot musculature. Subjected to the repetitive sheer forces of weight-bearing against the plantar aspect of the metatarsal heads, the transected axons engage in frustrated, disorganized sprouting. This results in a bulbous, highly sensitive mass of tangled nerve fibers embedded in dense scar tissue. The distinction between primary perineural fibrosis and a recurrent stump neuroma dictates our surgical approach, preoperative counseling, and expected postoperative outcomes.
Epidemiological Considerations and Biomechanical Etiology
Epidemiologically, Morton’s neuroma exhibits a striking predilection for the female demographic, with a female-to-male ratio frequently reported as high as 8:1 to 10:1. This gender disparity is heavily attributed to extrinsic biomechanical factors, most notably footwear choices. High-heeled shoes with narrow, restrictive toe boxes force the forefoot into a confined space while simultaneously hyperextending the metatarsophalangeal (MTP) joints. This hyperextension effectively tethers the common digital nerve against the distal edge of the deep transverse metatarsal ligament, maximizing tensile and compressive forces during the terminal stance phase of the gait cycle.

The anatomical distribution of these lesions is highly predictable. Approximately 85% to 90% of primary interdigital neuromas are localized to the third intermetatarsal space, with the vast majority of the remainder occurring in the second interspace. Involvement of the first or fourth interspaces is exceedingly rare and should immediately prompt the clinician to broaden the differential diagnosis. The predilection for the third interspace is multifactorial. Biomechanically, the third web space represents the junction between the relatively rigid medial three rays (stabilized by the Lisfranc complex) and the more mobile lateral two rays. This differential mobility creates increased shearing forces across the third interspace during ambulation.
Furthermore, anatomical constraints play a critical role. Cadaveric and radiographic studies have consistently demonstrated that the second and third intermetatarsal spaces are significantly narrower than the first and fourth. When this diminished spatial capacity is combined with the increased neural cross-sectional area often found in the third interspace—frequently due to the presence of a communicating branch between the medial and lateral plantar nerves—the threshold for mechanical entrapment is substantially lowered.
Differential Diagnosis and Clinical Mimickers
The diagnosis of an interdigital neuroma is primarily clinical, but it demands a rigorous exclusion of other forefoot pathologies that can present with remarkably similar symptomatology. Misdiagnosis is the leading cause of "recurrent" symptoms presenting within the first 12 months following a primary excision. True amputation stump neuromas typically require 1 to 4 years of continuous mechanical irritation to develop sufficient axonal mass to become symptomatic. Therefore, early postoperative failure strongly suggests that the original pain generator was either missed or misidentified.
The differential diagnosis must comprehensively evaluate both osseous and soft-tissue structures. MTP joint synovitis, particularly involving the second or third ray, is perhaps the most common confounder. While both conditions cause localized forefoot pain, MTP synovitis is typically exacerbated by direct palpation of the joint capsule and forced plantarflexion of the toe, which stretches the inflamed dorsal capsule. In contrast, neuroma pain is generally worsened by MTP hyperextension and lateral compression of the forefoot. Plantar plate tears, often presenting with a positive dorsal drawer test of the proximal phalanx, must also be meticulously ruled out.
Other critical differentials include Freiberg’s infraction (avascular necrosis of the metatarsal head, most commonly the second), which can be identified via standing radiographs demonstrating sclerosis or collapse of the articular surface. Stress fractures of the metatarsal necks are common in active individuals and elicit pain with axial loading of the digit. Proximal nerve entrapments, such as tarsal tunnel syndrome, can refer pain distally to the forefoot, mimicking a neuroma. Finally, systemic conditions like diabetic peripheral neuropathy, lumbar radiculopathy (particularly L5 or S1), and space-occupying soft tissue masses (ganglion cysts, synovial cysts, or lipomas) must be systematically excluded through a thorough history, physical examination, and appropriate diagnostic adjuncts.
Detailed Surgical Anatomy and Biomechanics
Neurovascular Topography of the Forefoot
Mastery of forefoot neurovascular anatomy is the fundamental prerequisite for safe and effective neuroma excision. The sensory innervation of the plantar forefoot is provided by the terminal branches of the tibial nerve: the medial and lateral plantar nerves. The medial plantar nerve is the larger of the two, typically supplying sensory coverage to the plantar aspect of the first, second, and third digits, as well as the medial hemi-pulp of the fourth digit. It courses obliquely across the plantar vault, emerging plantar and medial to the flexor digitorum brevis musculature. The lateral plantar nerve provides sensation to the lateral hemi-pulp of the fourth digit and the entirety of the fifth digit.
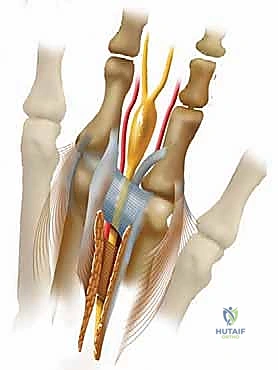
As these main nerve trunks approach the metatarsal heads, they arborize into the common digital nerves. These common digital nerves course distally within the intermetatarsal spaces, positioned plantarly to the deep transverse metatarsal ligament. Just distal to this ligament, they bifurcate into the proper digital nerves, which provide terminal sensation to the adjacent sides of the toes. A critical anatomical variant, present in approximately 27% of the population, is a communicating branch that courses obliquely from the lateral plantar nerve to join the medial plantar nerve, most frequently within the third intermetatarsal space. This confluence of neural tissue significantly increases the cross-sectional diameter of the nerve precisely at the level where the intermetatarsal space is narrowest, creating a perfect anatomical storm for entrapment.
Running in close proximity to the common digital nerves are the common digital arteries and veins. The common digital artery typically originates from the plantar metatarsal arteries. Crucially, the artery generally courses dorsal to the nerve within the intermetatarsal space, often crossing from a proximal-medial to a distal-lateral position relative to the nerve. During surgical excision, particularly via a dorsal approach, the surgeon will encounter the artery before the nerve. Meticulous blunt dissection is required to separate the neurovascular bundle, preserving the artery to prevent postoperative digital ischemia, while isolating the nerve for resection.
The Transverse Metatarsal Ligament and Intermetatarsal Space
The deep transverse metatarsal ligament (DTML) is a stout, unyielding band of fibrous tissue that connects the plantar plates of the adjacent MTP joints. It forms the rigid roof of the intermetatarsal space through which the neurovascular bundle must pass. The floor of this space is formed by the plantar aponeurosis and the plantar skin, while the medial and lateral walls are defined by the adjacent metatarsal shafts and heads.
The DTML is the primary site of mechanical entrapment in Morton's neuroma. During the propulsive phase of gait, as the heel rises and the MTP joints hyperextend, the common digital nerve is stretched tightly against the distal margin of the DTML. Over time, this repetitive bowstringing effect induces the characteristic perineural fibrosis. Complete surgical division of the DTML is therefore a non-negotiable step in the primary excision of a neuroma. Failure to completely release this ligament not only leaves the mechanical entrapment unresolved but also severely limits the surgeon's ability to trace the nerve proximally for adequate resection.
Adjacent to the neurovascular bundle within the intermetatarsal space are the lumbrical muscles. These intrinsic muscles originate from the tendons of the flexor digitorum longus and course distally to insert into the medial aspect of the extensor expansion of the digits. The lumbrical tendon typically lies lateral and superficial (plantar) to the neurovascular bundle. In a blood-stained or poorly illuminated surgical field, a pale, fibrotic lumbrical tendon can easily be mistaken for the common digital nerve. Inadvertent resection of the lumbrical tendon instead of the neuroma is a documented cause of persistent postoperative pain and surgical failure.
Critical Anatomical Variants and Tethering Structures
Beyond the primary neurovascular structures, the surgeon must be acutely aware of secondary tethering structures that can complicate nerve resection. The most critical of these are the small, plantar-directed articular and cutaneous nerve branches that originate from the common digital nerve proximal to the DTML. These tiny branches course plantarly to innervate the plantar skin and the joint capsule.
If these plantar-directed branches are not identified and meticulously divided during the proximal dissection, they will act as unyielding tethers. When the surgeon attempts to transect the common digital nerve proximally, these tethers will prevent the proximal stump from retracting deeply into the intrinsic musculature of the foot. Instead, the stump will remain suspended superficially, just beneath the weight-bearing surface of the metatarsal heads. This is the primary iatrogenic mechanism for the development of a highly symptomatic, recurrent amputation stump neuroma.
Furthermore, when utilizing a dorsal surgical approach, the surgeon must navigate the dorsal sensory nerves. These are terminal branches of the superficial peroneal nerve (and occasionally the sural nerve laterally). They course within the superficial subcutaneous tissues, directly over the intermetatarsal spaces. Careless superficial dissection or aggressive retraction can lead to transection or traction neuropraxia of these dorsal sensory nerves, resulting in frustrating postoperative numbness or painful dorsal neuromas that complicate the patient's recovery.
Exhaustive Indications and Contraindications
Diagnostic Criteria for Surgical Intervention
The decision to proceed with surgical excision of an interdigital neuroma should be made only after a thorough clinical evaluation and the exhaustion of appropriate conservative measures. Surgery is indicated for patients who present with classic, debilitating symptoms that significantly impair their activities of daily living and have proven refractory to non-operative management.
Patients typically describe a burning, lancinating, or electrical pain radiating into the affected toes. A classic subjective complaint is the sensation of "walking on a marble" or a wrinkled sock bunched up under the forefoot. Symptoms are almost universally exacerbated by wearing tight, narrow, or high-heeled shoes and are dramatically relieved by removing the footwear and massaging the foot. If a patient experiences significant pain while walking barefoot on a soft carpet, the diagnosis of a primary neuroma should be questioned, as this removes the compressive forces that typically trigger neuroma pain.
A trial of conservative management, lasting a minimum of 3 to 6 months, is mandatory. This includes aggressive footwear modification (wide toe box, zero-drop heels, rigid soles), the use of custom or over-the-counter orthotics with a metatarsal dome pad placed immediately proximal to the metatarsal heads to splay the intermetatarsal space, and judicious use of corticosteroid injections. Surgical excision is indicated when these modalities fail to provide lasting relief, and the patient's quality of life remains compromised.
Absolute and Relative Contraindications
While neuroma excision is a highly successful procedure in appropriately selected patients, several contraindications must be respected to avoid catastrophic complications or exacerbation of underlying pathology. Absolute contraindications include the presence of an active, untreated local or systemic infection. Operating in an infected field risks deep space infection, osteomyelitis, and devastating functional loss. Severe peripheral vascular disease is another absolute contraindication. The forefoot relies on a delicate microvascular network; surgical trauma in the setting of profound ischemia can precipitate non-healing wounds, gangrene, and eventual amputation.
Relative contraindications require careful preoperative optimization and patient counseling. Poorly controlled diabetes mellitus increases the risk of postoperative infection and delayed wound healing. Furthermore, diabetic patients frequently suffer from concurrent peripheral neuropathy. It is exceptionally challenging to differentiate the focal pain of a neuroma from the diffuse burning of diabetic neuropathy. Operating on a neuropathic foot risks failing to relieve the patient's primary symptoms and introduces the risk of Charcot neuroarthropathy.
Patients with a history of complex regional pain syndrome (CRPS) represent a high-risk cohort. Surgical trauma can trigger a severe flare of CRPS, leading to chronic, debilitating pain that far exceeds the original neuroma symptoms. Finally, if the clinical picture is dominated by concurrent forefoot pathology—such as severe hallux valgus, profound lesser toe deformities, or advanced MTP joint osteoarthritis—isolated neuroma excision is likely to fail. In these complex cases, the neuroma is often a secondary manifestation of global forefoot biomechanical collapse, and a comprehensive reconstructive approach is required.
Table: Indications and Contraindications
| Category | Specific Criteria | Clinical Rationale / Considerations |
|---|---|---|
| Indications | Refractory Pain | Failure of 3-6 months of conservative care (footwear modification, orthotics, injections). |
| Classic Symptomatology | Burning, electrical pain radiating to toes, "marble" sensation, worsened by tight shoes. | |
| Positive Provocative Exams | Positive Mulder's click, focal web space tenderness, negative MTP joint drawer tests. | |
| Diagnostic Injection Relief | Temporary but complete cessation of pain following a localized local anesthetic block. | |
| Absolute Contraindications | Active Local Infection | Risk of deep space infection, osteomyelitis, and systemic sepsis. |
| Severe Ischemia / PVD | Inability to heal surgical wounds; high risk of gangrene and subsequent amputation. | |
| Pure Radiculopathy | Pain originating from lumbar spine (e.g., L5/S1); distal surgery will not alter symptoms. | |
| Relative Contraindications | Uncontrolled Diabetes | High risk of wound complications, infection, and concurrent diffuse peripheral neuropathy. |
| History of CRPS | Surgical trauma may trigger a severe, debilitating flare of sympathetically mediated pain. | |
| Severe Concurrent Deformity | Advanced hallux valgus or global crossover toe deformities require comprehensive reconstruction, not isolated excision. |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Evaluation and Provocative Maneuvers
The cornerstone of preoperative planning for neuroma excision is a meticulous physical examination. The examination begins with a weight-bearing inspection of the foot. The surgeon should look for splaying of the toes, specifically the "V" sign (divergence of the digits adjacent to the affected web space), which can indicate a bulky neuroma or, more commonly, an underlying plantar plate rupture.

Palpation is performed systematically, starting proximally between the metatarsal shafts and moving distally into the web space. Focal tenderness precisely between the metatarsal heads is highly suggestive of a neuroma. The surgeon must then perform the MTP joint plantarflexion stress test and the dorsal drawer test. Pain or instability during these maneuvers points toward MTP joint synovitis or plantar plate insufficiency, respectively, which must be addressed to ensure a successful outcome.

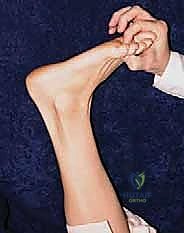
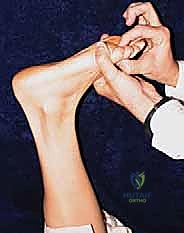
The pathognomonic clinical test is the Mulder maneuver. With the patient supine or seated, the examiner grasps the medial and lateral aspects of the forefoot with one hand, applying a compressive force to squeeze the metatarsal heads together. Simultaneously, the thumb and index finger of the opposite hand are placed on the dorsal and plantar aspects of the affected web space. As the metatarsal heads are compressed, the thickened neuroma is forced plantarly, escaping the narrow intermetatarsal space. This displacement often produces a palpable and sometimes audible "click." Crucially, this click must reproduce the patient's exact radiating pain to be considered diagnostic. A painless click is frequently a normal variant caused by the shifting of intermetatarsal bursal tissue.
Advanced Imaging and Diagnostic Modalities
While the diagnosis is primarily clinical, imaging plays a vital role in ruling out other pathologies and confirming the diagnosis in equivocal cases. Standard weight-bearing radiographs (anteroposterior, lateral, and oblique views) are mandatory. These films are utilized to evaluate for stress fractures, Freiberg's infraction, degenerative joint disease, and the overall alignment of the metatarsal parabola.



When the clinical picture remains unclear, advanced imaging is warranted. High-resolution diagnostic ultrasonography has emerged as a highly sensitive and specific modality for identifying interdigital neuromas. It offers the distinct advantage of dynamic assessment; the sonographer can perform a Mulder maneuver under real-time visualization, observing the hypoechoic neuroma mass subluxating plantarly between the metatarsal heads.
Magnetic Resonance Imaging (MRI) is also highly effective, though more costly and static. On MRI, a neuroma typically appears as a teardrop-shaped or dumbbell-shaped soft tissue mass within the intermetatarsal space, situated plantar to the DTML. It classically demonstrates low to intermediate signal intensity on both T1-weighted and T2-weighted sequences, reflecting its dense, fibrotic nature. MRI is particularly valuable for identifying concurrent pathologies, such as intermetatarsal bursitis or subtle plantar plate tears, which may alter the surgical plan.
Finally, a diagnostic local anesthetic block is an invaluable tool. Injecting 1-2 cc of short-acting local anesthetic (e.g., 1% lidocaine) precisely into the symptomatic web space, taking care to remain plantar to the DTML, should result in complete, albeit temporary, resolution of the patient's typical pain. If the block fails to provide relief, the surgeon must seriously reconsider the diagnosis of an interdigital neuroma before proceeding with excision.
Anesthesia, Patient Positioning, and Tourniquet Application
Neuroma excision can be safely and effectively performed under various anesthetic modalities, ranging from local anesthesia with monitored anesthesia care (MAC) to regional blocks (popliteal or ankle blocks) or general anesthesia. The choice depends on patient preference, comorbidities, and the surgeon's comfort level. A regional ankle block provides excellent intraoperative anesthesia and extends postoperative pain control, minimizing the need for systemic opioids.
The patient is positioned supine on the operating table. A small bump placed beneath the ipsilateral hip is highly recommended. This bump internally rotates the operative leg slightly, bringing the foot into a neutral, vertically oriented position. This simple maneuver dramatically improves the surgeon's visualization of the dorsal web spaces, preventing the foot from externally rotating away from the surgical field.
Hemostasis is critical for identifying the delicate neurovascular structures and avoiding inadvertent injury. A tourniquet is almost universally employed. An ankle tourniquet (typically inflated to 250 mmHg) or a calf tourniquet is sufficient for isolated neuroma excisions. The limb is elevated and exsanguinated with an Esmarch bandage prior to tourniquet inflation. The surgeon must ensure adequate padding beneath the tourniquet to prevent pressure necrosis or nerve palsy, particularly in patients with thin subcutaneous tissue.
Step-by-Step Surgical Approach and Fixation Technique
The Dorsal Approach: Incision and Dissection
The dorsal approach is the gold standard for primary interdigital neuroma excision. It avoids placing a potentially painful scar on the weight-bearing plantar surface of the foot, which is a significant risk with the plantar approach.


The procedure begins with a 3 to 4 cm longitudinal incision centered over the affected intermetatarsal space. The incision should start just proximal to the web space commissure and extend proximally between the metatarsal shafts. Careful superficial dissection is performed using sharp dissecting scissors or a scalpel, taking great care to identify and retract any crossing dorsal sensory nerve branches or prominent dorsal veins.


Once the superficial fascia is breached, blunt dissection is utilized to enter the deep intermetatarsal space. A small self-retaining retractor, such as a Weitlaner or a specialized lamina spreader, is gently inserted between the metatarsal heads. As the retractor is opened, the intermetatarsal space is splayed, placing the deep structures under tension and dramatically improving visualization.

Division of the Transverse Metatarsal Ligament
With the space retracted, the surgeon must identify the deep transverse metatarsal ligament (DTML). It appears as a taut, glistening white band of transverse fibers running between the metatarsal necks. The neuroma and neurovascular bundle lie deep (plantar) to this structure.


Using a pair of fine scissors or a scalpel, the DTML is carefully divided longitudinally from distal to proximal. It is imperative to ensure complete transection of the ligament. The surgeon can confirm complete release by passing a blunt Freer elevator proximally along the nerve; there should be no remaining restrictive bands. At this stage, the surgeon or an assistant can apply upward pressure on the plantar aspect of the web space. This "push-up" maneuver forces the neuroma dorsally into the surgical wound, making it readily identifiable as a bulbous, yellowish-white enlargement of the nerve.
Nerve Isolation, Resection, and Stump Management
Once the neu
Clinical & Radiographic Imaging Archive






