Minimally Invasive Lateral: Secure Proximal Humerus Fixation
Introduction & Epidemiology
Proximal humerus fractures (PHFs) represent a significant orthopedic burden, accounting for approximately 5-6% of all fractures and 45% of all humerus fractures. Their incidence is biphasic, with a peak in younger, high-energy trauma patients and a much larger peak in elderly, osteoporotic individuals, particularly post-menopausal women, often following low-energy falls. The increasing life expectancy of the global population projects a continuous rise in PHF incidence, posing substantial challenges to healthcare systems.
PHFs exhibit a wide spectrum of fracture patterns, classically categorized by Neer (2-, 3-, 4-part fractures) based on displacement of the four major segments: the humeral head, greater tuberosity, lesser tuberosity, and humeral shaft. The AO/OTA classification provides a more comprehensive, alphanumeric system detailing articular involvement, metaphyseal comminution, and shaft extension. The choice between operative and non-operative management, as well as the specific surgical technique, is highly dependent on these fracture characteristics, patient demographics, bone quality, and functional demands.
Minimally invasive approaches to PHF fixation have gained considerable traction in recent decades. The rationale for these techniques stems from the desire to reduce soft tissue disruption, preserve the tenuous blood supply to the humeral head, minimize surgical morbidity (e.g., infection, wound complications), and potentially accelerate rehabilitation. While the traditional deltopectoral approach offers excellent visualization, it often necessitates significant soft tissue stripping, particularly of the deltoid and rotator cuff, which can compromise the humeral head's vascularity. The minimally invasive lateral approach, employing percutaneous or limited incision techniques, aims to mitigate these risks by respecting the biology of the fracture environment. This approach is particularly advantageous for fractures with significant shaft extension or segmental patterns where direct exposure of the shaft is required while minimizing trauma to the proximal articular segment.
Surgical Anatomy & Biomechanics
A thorough understanding of the complex anatomy and biomechanics of the proximal humerus is paramount for successful PHF management.
Surgical Anatomy
- Bony Anatomy: The proximal humerus comprises the humeral head, articular cartilage, anatomical neck, greater tuberosity (insertion of supraspinatus, infraspinatus, teres minor), lesser tuberosity (insertion of subscapularis), surgical neck, and proximal shaft. The bicipital groove lies between the tuberosities, housing the long head of the biceps tendon.
- Vascular Supply: The humeral head's blood supply is critical for fracture healing and preventing avascular necrosis (AVN). The primary supply originates from the anterior and posterior circumflex humeral arteries, branches of the axillary artery. The ascending branch of the anterior circumflex humeral artery (arcuate artery) runs within the bicipital groove, supplying the majority of the humeral head, particularly the superior and posterior aspects. Metaphyseal vessels also contribute. Significant displacement, particularly of the tuberosities, can disrupt this delicate vascular network, increasing AVN risk.
-
Nerve Anatomy:
- Axillary Nerve: The most critical nerve in the lateral approach, the axillary nerve typically courses transversely 5-7 cm distal to the lateral acromion, deep to the deltoid muscle. It innervates the deltoid and teres minor and provides sensory supply to the lateral shoulder via the superior lateral cutaneous nerve of the arm. Injury can result in deltoid weakness or paralysis and sensory deficits.
- Radial Nerve: While less frequently injured in direct lateral proximal humeral approaches, the radial nerve is vulnerable in fractures extending distally into the humeral shaft, particularly when inserting distal locking screws or during plate tunneling, as it spirals around the posterior aspect of the humerus in the radial groove, approximately 10-15 cm distal to the acromion.
- Musculocutaneous Nerve: Supplies the biceps and brachialis, typically not at risk with lateral approaches unless dissecting extensively anteriorly.
- Soft Tissue Envelope: The deltoid muscle covers the proximal humerus laterally. The rotator cuff tendons insert onto the greater and lesser tuberosities. These soft tissue attachments are vital for fragment reduction and maintaining stability, particularly for tuberosity fragments.
Biomechanics of Fixation
The biomechanical environment of the proximal humerus presents unique challenges for internal fixation:
*
Osteoporotic Bone:
A significant proportion of PHFs occur in osteoporotic bone, which limits screw purchase and increases the risk of screw cutout, particularly in the humeral head.
*
Shear Forces:
The high shear forces across the surgical neck, exacerbated by rotator cuff muscle pull, necessitate robust fixation to prevent varus collapse.
*
Medial Support:
Restoration of medial column continuity and support (either bone-to-bone contact or using a calcar screw/medial support plate) is paramount for preventing varus collapse and screw cutout, especially in osteoporotic bone. Locking plates alone, without medial support, may act as a fulcrum leading to failure.
*
Locking Plate Technology:
Modern locking plates, such as those designed for the proximal humerus (e.g., PHILOS plate), offer angular stability, effectively creating a fixed-angle construct. This reduces reliance on bone-screw interface compression, which is beneficial in osteoporotic bone. However, even with locking plates, the principles of anatomic reduction and stable fixation, including medial support, remain critical.
*
Screw Configuration:
Multiple, diverging locking screws into the humeral head provide a larger capture volume and improved resistance to pullout. Optimal screw length should approach the subchondral bone without penetrating the articular surface.
Indications & Contraindications
The decision-making process for PHFs is complex and multifactorial, balancing patient factors, fracture characteristics, and surgeon experience.
Operative Indications for Minimally Invasive Lateral Fixation
- Displaced 2-, 3-, and 4-part fractures: Especially those with significant displacement of the humeral head, tuberosities, or surgical neck, where non-operative management would lead to unacceptable functional outcomes (e.g., restricted motion, pain, severe malunion).
- Fracture-dislocations: Proximal humerus fractures accompanied by glenohumeral dislocation, particularly if irreducible by closed means.
- Segmental fractures: Fractures involving the proximal metaphysis and extending into the diaphysis, often requiring longer plates.
- Fractures with significant shaft extension: Where a traditional deltopectoral approach might not provide adequate distal exposure for plate fixation without excessive stripping, or where a limited deltoid split provides a direct path to the lateral shaft.
- Young, active patients: With displaced fractures, where restoration of anatomy and function is prioritized.
- Failure of non-operative management: Progressive displacement or symptomatic non-union after a trial of conservative care.
- Open fractures: After appropriate debridement and stabilization, often initially with external fixation.
- Polytrauma patients: Where early fixation facilitates rehabilitation and reduces systemic complications.
Contraindications
-
Absolute Contraindications:
- Active local or systemic infection.
- Extremely comminuted humeral head where reconstructive ORIF is deemed impossible or highly unlikely to succeed, and primary arthroplasty is a more appropriate solution.
- Severe overlying soft tissue compromise or devascularization.
-
Relative Contraindications:
- Severe osteoporosis precluding stable screw purchase (may favor arthroplasty).
- Patient comorbidities that significantly increase surgical risk (e.g., severe cardiopulmonary disease).
- Patient unwillingness or inability to comply with post-operative rehabilitation.
- Minimally displaced, stable fractures (often managed non-operatively).
- Extremely elderly, low-demand patients with acceptable alignment (consider non-operative management).
Table: Operative vs. Non-Operative Indications
| Feature | Operative Management (Minimally Invasive Lateral) | Non-Operative Management |
|---|---|---|
| Fracture Displacement | Significant displacement (Neer >1 cm or >45 degrees angulation), fracture-dislocations. | Minimally displaced (Neer <1 cm and <45 degrees angulation), stable valgus-impacted fractures. |
| Fracture Pattern | Unstable 2-, 3-, 4-part; segmental fractures; fractures with shaft extension. | Stable 1- or 2-part fractures. |
| Patient Age/Activity | Younger, active patients with high functional demands; some active elderly patients. | Very elderly, low-demand patients; patients with significant comorbidities. |
| Bone Quality | Adequate for implant purchase (though locking plates help in osteoporotic bone). | Poor bone quality, severe osteoporosis (where stable fixation is unlikely). |
| Comorbidities | Manageable surgical risk. | Severe comorbidities precluding safe anesthesia/surgery. |
| Soft Tissue | Intact or salvageable soft tissue envelope. | Significant soft tissue compromise (e.g., severe open fracture, burns) requiring alternative. |
| Functional Goal | Restoration of anatomical alignment and near-full function. | Pain control, maintenance of reasonable function, accepting potential malunion. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful surgical outcomes for PHFs.
Imaging Acquisition and Interpretation
- Plain Radiographs: A complete trauma series including AP, scapular Y, and axillary views is essential. These provide initial assessment of fracture pattern, displacement, and glenohumeral joint integrity.
- Computed Tomography (CT) Scan: Crucial for complex fracture patterns (3- and 4-part, head-splitting, fracture-dislocations) to delineate articular involvement, quantify displacement, assess comminution (especially of the tuberosities and calcar), and identify potential loose bodies. 3D reconstructions are invaluable for understanding the complex fracture geometry and planning screw trajectories.
- Angiography/Doppler Ultrasound: Indicated if there is suspicion of associated vascular injury (rare but critical).
Templating and Implant Selection
- Plate Length and Type: Based on fracture pattern and shaft extension. Longer plates may be necessary for segmental fractures or those extending distally. Locking plates designed for the proximal humerus (e.g., PHILOS, LCP Proximal Humerus Plate) are standard, offering fixed-angle stability.
-
Screw Selection:
- Proximal Screws: Locking screws, often converging, aiming for subchondral bone without articular penetration. Multiple screws (typically 5-7) are used to create a stable construct and enhance pullout resistance, especially those targeting the calcar.
- Distal Screws: Cortical or locking screws, usually bicortical, for diaphyseal fixation.
- Ancillary Fixation: K-wires for temporary reduction and rotation control, suture anchors for tuberosity reattachment (if needed), bone graft (autograft or allograft) for metaphyseal defects or medial column support.
Patient Consent and Risk Discussion
Detailed discussion with the patient regarding the anticipated procedure, potential benefits, and a comprehensive list of risks including non-union, malunion, avascular necrosis, infection, neurovascular injury (axillary nerve particularly), screw cutout, implant prominence, and the need for possible reoperation or arthroplasty.
Patient Positioning
The patient is typically placed in a
supine position
on a radiolucent operating table.
* The affected arm is positioned on a hand table or cantilevered off the edge of the main table, allowing for full range of motion, particularly abduction and rotation, necessary for fracture reduction maneuvers and C-arm imaging.
* The
head of the table is often elevated (reverse Trendelenburg)
to 20-30 degrees. This reduces venous pressure, which can minimize operative bleeding and improve visualization.
* A
sandbag or bolster
is placed under the ipsilateral scapula to protract the shoulder, facilitating posterior screw placement and providing a stable platform.
* Ensure
unrestricted C-arm access
for intraoperative fluoroscopy in multiple planes (AP, lateral/Y-view, axillary view) to confirm reduction, plate position, and screw length. The C-arm should be draped to allow sterile manipulation.
*
Anesthesia:
General endotracheal anesthesia is typically used, often supplemented with an interscalene brachial plexus block for post-operative pain management.
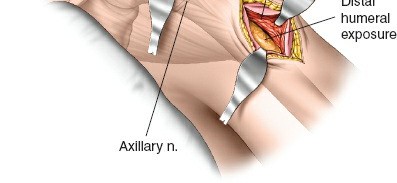
Figure: Patient positioned supine on a radiolucent table with the ipsilateral arm free-draped, allowing for full intraoperative manipulation and C-arm access.
Detailed Surgical Approach / Technique
The minimally invasive lateral approach leverages the principle of indirect reduction and percutaneous plating while minimizing soft tissue stripping. The goal is stable fixation with preservation of the humeral head's blood supply.
Skin Incision and Landmarks
The approach typically involves one or two small incisions.
*
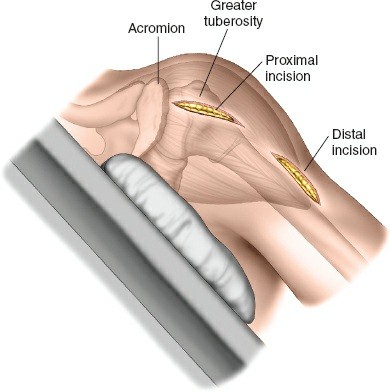
Proximal Incision:
A 3-5 cm longitudinal incision centered over the lateral aspect of the greater tuberosity, extending distally from the acromion.
*
Distal Incision(s):
One or more smaller incisions, or a single longer incision made more distally along the humeral shaft, are used for plate insertion and distal screw fixation. The precise location depends on fracture extension and plate length. These incisions facilitate tunneling of the plate.
Landmarks include the lateral acromion, the deltoid tubercle, and palpation of the humeral shaft.
Dissection and Internervous Planes
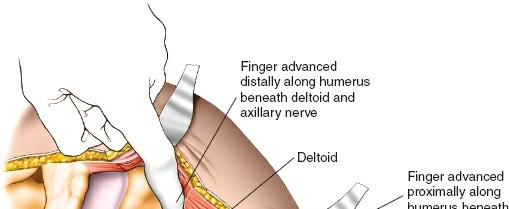
- Deltoid Split: The primary approach involves a longitudinal split within the fibers of the deltoid muscle. This split should be carefully performed to avoid injuring the axillary nerve. The safe zone for a deltoid split is generally considered to be within 5-7 cm distal to the acromial edge. Electrocautery is used for muscle splitting.
- Protecting the Axillary Nerve: As the deltoid fibers are split, the surgeon must be acutely aware of the axillary nerve running transversely on the deep surface of the deltoid. blunt dissection is preferred, and identifying the nerve's course visually or through palpation (if possible) or by careful measurement from the acromion is critical. Use of retractors should be gentle and precise to avoid nerve compression.
- Submuscular Tunneling: Once the proximal fracture site is exposed, a submuscular tunnel is created distally, superficial to the periosteum but deep to the deltoid muscle. This tunnel will accommodate the proximal humerus plate. The tunneling can be performed with a blunt instrument or the plate itself, guided by fluoroscopy.
Fracture Reduction
The goal is anatomical reduction, restoring length, rotation, and alignment.
*
Indirect Reduction:
Often preferred to minimize periosteal stripping.
*
Traction and Manipulation:
Longitudinal traction applied to the arm, combined with external rotation or abduction, can help reduce the head and shaft fragments.
*
Ligamentotaxis:
Soft tissue attachments (rotator cuff, periosteum) can assist in reducing fragments when traction is applied.
*
Percutaneous K-wires/Joysticks:
Small K-wires can be inserted percutaneously into the humeral head or shaft fragments to serve as joysticks for direct manipulation under fluoroscopic guidance.
*
Direct Reduction (Limited):
Through the proximal incision, specialized reduction clamps or bone hooks can be used to directly manipulate displaced tuberosities or the humeral head.
*
Medial Column Support:
Crucial for stability. If there's a metaphyseal defect, bone graft (autograft or allograft) can be inserted to provide structural support to the medial calcar region, preventing varus collapse.
Plate Application & Fixation
- Plate Insertion: Once reduction is achieved and temporarily maintained (e.g., with K-wires), the chosen locking plate is inserted through the proximal incision into the submuscular tunnel, guiding it distally along the lateral aspect of the humerus.
-
Plate Positioning: The plate should be positioned approximately 5-8 mm distal to the superior aspect of the greater tuberosity and slightly anterior to the bicipital groove. This allows for optimal screw trajectories into the humeral head and avoids impingement with the acromion or rotator cuff. Fluoroscopy confirms correct plate position.
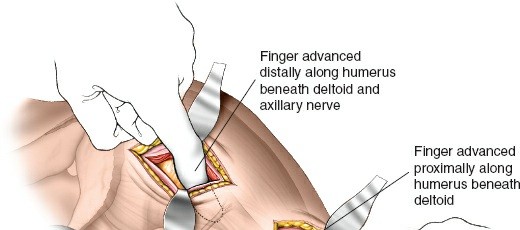
Figure: Intraoperative fluoroscopic image demonstrating the correct positioning of the locking plate on the lateral aspect of the proximal humerus, distal to the greater tuberosity. -
Distal Fixation:
- Through the distal incision(s) or via percutaneous guides, the plate is secured to the humeral shaft.
- A minimum of 3-4 bicortical locking screws are typically used distally to achieve stable fixation to the diaphysis.
-
Care is taken to ensure the plate is centralized on the shaft, and that screw trajectories do not endanger the radial nerve, especially for plates extending into the mid-shaft.
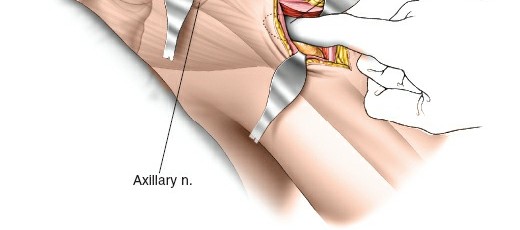
Figure: Percutaneous insertion of distal locking screws, ensuring bicortical purchase and adequate working length.
-
Proximal Fixation:
- Once distal fixation is secure, attention turns to the humeral head.
- Multiple (typically 5-7) converging locking screws are inserted into the humeral head through the plate. These screws should aim for the subchondral bone for maximum purchase.
- Calcar Screws: At least one screw should be directed inferomedially towards the calcar region (medial support screw). This screw acts as an additional buttress against varus collapse, which is a common mode of failure.
-
Screw Length:
Accurate screw length measurement is paramount. Intraoperative fluoroscopy in multiple planes (AP, lateral, axillary) is used to confirm screw tip position and ensure no intra-articular penetration. Articular penetration can lead to chondral damage, pain, and early arthritis.

Figure: Fluoroscopic image showing multiple converging locking screws achieving fixation in the humeral head, with attention to screw length and subchondral engagement.
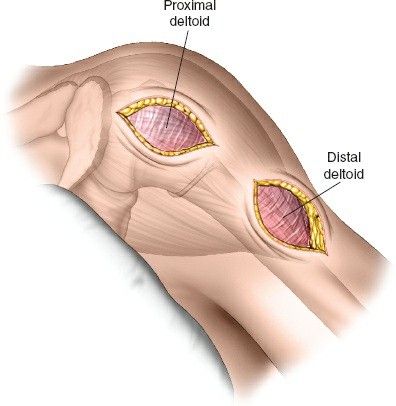
Figure: Lateral fluoroscopic view confirming optimal screw lengths within the humeral head, avoiding articular breach.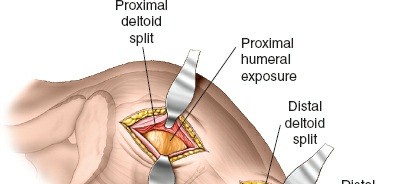
Figure: Axillary view demonstrating the trajectory and depth of the proximal locking screws, crucial for avoiding anterior or posterior articular penetration. -
Tuberosity Fixation (if applicable): If the greater or lesser tuberosities are fractured and displaced, they are reduced anatomically and can be fixed directly to the plate using non-locking screws or held with transosseous sutures passed through suture holes in the plate. This is vital for restoring rotator cuff function.
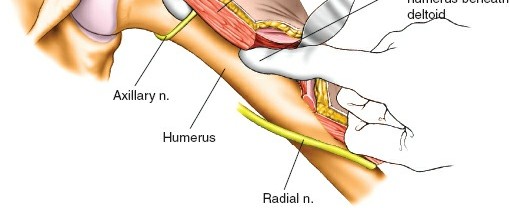
Figure: Final fluoroscopic image after complete plate and screw fixation, demonstrating stable reduction of the proximal humerus fracture and optimal implant position.
Figure: Post-operative radiograph (AP view) showing the definitive fixation of a complex proximal humerus fracture with a lateral locking plate.
Wound Closure
After confirming stable fixation and hemostasis, the incisions are irrigated. The deltoid muscle is allowed to fall back into place. Subcutaneous tissue and skin are closed in layers. A drain is usually not necessary but may be considered in cases of significant bleeding or extensive soft tissue dissection.
Complications & Management
Despite advancements in surgical techniques and implants, complications remain a concern in PHF fixation, particularly given the often-osteoporotic bone and complex vascular supply.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence | Etiology/Risk Factors | Clinical Presentation | Salvage Strategies |
|---|---|---|---|---|
| Non-union/Malunion | 5-20% | Inadequate reduction/fixation, poor bone quality, vascular compromise, infection, smoking. | Persistent pain, functional limitation, deformity. | Revision ORIF with bone grafting, conversion to hemiarthroplasty/TSA. |
| Avascular Necrosis (AVN) | 0-30% | 3/4-part fractures, extensive soft tissue stripping, displacement of medial calcar. | Progressive pain, collapse of humeral head, osteonecrosis on imaging. | Hemiarthroplasty, total shoulder arthroplasty (TSA), reverse TSA (rTSA). |
| Screw Cut-out/Pull-out | 5-20% | Osteoporosis, poor reduction (varus collapse), lack of medial support, improper screw length/trajectory. | Acute pain, loss of reduction, implant failure. | Revision with longer screws/bone graft, conversion to arthroplasty. |
| Axillary Nerve Injury | 2-15% (transient) | Direct trauma during deltoid split, excessive retraction, thermal injury. | Deltoid weakness/paralysis, lateral shoulder sensory deficit. | Observation (most recover), EMG for prognosis, nerve repair/graft if indicated. |
| Radial Nerve Injury | <1% (lateral approach) | Distal screw placement, extensive distal dissection, fracture extension to shaft. | Wrist drop, sensory loss in radial distribution. | Observation, nerve exploration/repair if no recovery. |
| Infection | 1-5% | Open fracture, prolonged surgery, poor wound care, patient comorbidities. | Pain, warmth, redness, swelling, drainage, systemic signs. | Debridement, antibiotics, implant removal (if severe), possible re-fixation. |
| Implant Prominence/Irritation | 10-30% | Malposition of plate, prominent screw heads, thin soft tissue coverage. | Pain with motion, palpable hardware. | Hardware removal (usually after fracture healing, 12-18 months post-op). |
| Rotator Cuff Dysfunction | 5-15% | Poor tuberosity reduction/healing, iatrogenic injury during exposure. | Persistent weakness, limited active motion. | Physiotherapy, revision of tuberosity fixation, possible rotator cuff repair. |
| Stiffness/Adhesive Capsulitis | 10-25% | Prolonged immobilization, inadequate rehabilitation, pain. | Progressive loss of passive and active range of motion. | Aggressive physiotherapy, manipulation under anesthesia, arthroscopic capsular release. |
Management Principles for Specific Complications
- Non-union: If asymptomatic, observation may suffice. Symptomatic non-unions often require revision surgery, including implant removal, debridement of the non-union site, re-reduction, stable fixation, and bone grafting (autograft or allograft, often with biologics like PRP or BMPs). For complex patterns or significant bone loss, conversion to arthroplasty (hemiarthroplasty or rTSA) may be considered.
- Avascular Necrosis (AVN): Management depends on the stage of AVN and patient symptoms. Early, asymptomatic AVN may be observed. Symptomatic AVN with humeral head collapse typically necessitates arthroplasty. In younger, active patients, hemiarthroplasty may be considered. In older patients with rotator cuff deficiency or severe glenoid involvement, reverse total shoulder arthroplasty (rTSA) is often preferred.
- Screw Cut-out: Most commonly seen with varus collapse, often due to inadequate medial support. Early recognition is crucial. If stable, observation. If causing acute pain or significant articular damage, revision surgery is required, potentially involving re-reduction, medial column support, longer/different screws, or conversion to arthroplasty.
- Nerve Injuries: Most iatrogenic nerve injuries (especially axillary nerve neuropraxia) are transient and managed with observation and electrodiagnostic studies (EMG/NCS) to assess recovery. Persistent deficits beyond 3-6 months may warrant surgical exploration and possible nerve repair or grafting.
Post-Operative Rehabilitation Protocols
A structured and individualized rehabilitation program is critical for optimizing functional recovery after PHF fixation. The protocol must balance protecting the fracture healing and fixation with preventing stiffness and restoring mobility. Close communication between the surgeon and physical therapist is essential.
General Principles
- Fracture Stability Dictates Protocol: The initial phase is guided by the stability of surgical fixation. Unstable fixation warrants more protected early motion.
- Pain Management: Adequate pain control is crucial for patient participation in rehabilitation.
- Gradual Progression: Exercise progression is slow and deliberate, avoiding sudden increases in load or range of motion.
- Patient Compliance: Emphasize patient education and adherence to home exercise programs.
Phases of Rehabilitation
-
Phase I: Protection and Early Motion (0-6 weeks Post-op)
- Immobilization: Sling or abduction pillow brace for comfort and protection (e.g., for 4-6 weeks). The arm should be kept close to the body, particularly when ambulating or sleeping.
- Goals: Control pain and swelling, protect fracture healing, prevent shoulder stiffness, maintain distal extremity function.
-
Exercises:
- Pendulum exercises: Gentle, gravity-assisted swings of the arm in flexion/extension and circumduction, performed while leaning forward.
- Passive Range of Motion (PROM): Initiated early (often within the first week), typically by a therapist, within pain-free limits. Focus on external rotation (0-30 degrees), flexion (0-90 degrees), and abduction (0-60 degrees), avoiding internal rotation past neutral or forced stretching.
- Active Elbow, Wrist, Hand ROM: Maintained frequently throughout the day.
- Scapular stabilization exercises: Gentle isometric contractions.
- Precautions: No active shoulder flexion, abduction, or internal rotation against resistance. Avoid lifting, pushing, or pulling.
-
Phase II: Active Assisted Range of Motion (AAROM) and Gentle Strengthening (6-12 weeks Post-op)
- Progression: As radiographic signs of healing appear (usually around 6 weeks), the sling may be discontinued gradually for ADLs.
- Goals: Restore full pain-free passive ROM, initiate active ROM, begin gentle strengthening.
-
Exercises:
- AAROM: Use of pulleys, cane exercises, and therapist-assisted movements to increase flexion, abduction, and rotation.
- Active Range of Motion (AROM): Gradually initiate AROM in all planes as pain allows.
- Isometric strengthening: Gentle isometric contractions for deltoid and rotator cuff (supraspinatus, infraspinatus, subscapularis) in neutral positions.
- Scapular strengthening: Retraction, protraction, depression.
- Precautions: Avoid lifting heavy objects. No sudden movements or impacts. Continue to avoid forceful or resisted internal rotation and abduction initially.
-
Phase III: Progressive Strengthening and Functional Return (12+ weeks Post-op)
- Progression: Once full AROM is achieved and fracture healing is robust (typically 3-4 months radiographically), resistance exercises are introduced.
- Goals: Restore full strength, power, endurance, and return to functional activities.
-
Exercises:
- Progressive resistance exercises (PRE): Using resistance bands, light weights, progressing to heavier weights. Focus on all major shoulder muscle groups: deltoid, rotator cuff, biceps, triceps, scapular stabilizers.
- Proprioceptive training: Balance and coordination exercises.
- Endurance training: Repetitive movements with lighter loads.
- Sport-specific/Work-specific training: Gradual introduction of activities mimicking patient's hobbies or occupation.
- Precautions: Listen to the body, avoid pain. Gradual increase in intensity and duration.
Full recovery can take 6-12 months, or even longer for complex fractures. Persistent pain, stiffness, or weakness should prompt re-evaluation for potential complications.
Summary of Key Literature / Guidelines
The management of proximal humerus fractures, particularly displaced and complex patterns, remains an area of ongoing research and debate. The shift towards minimally invasive techniques, including the lateral approach with locking plates, is supported by a growing body of literature highlighting several advantages over traditional open techniques.
- Biological Advantage: Numerous studies emphasize the importance of preserving the vascularity of the humeral head. Minimally invasive approaches, by limiting soft tissue dissection, are theorized to reduce the risk of avascular necrosis and promote fracture healing compared to extensive open approaches. Cadaveric studies and clinical series have demonstrated less periosteal stripping and potentially better preservation of the ascending branch of the anterior circumflex humeral artery with minimally invasive techniques.
- Locking Plate Efficacy: The advent of locking plate technology has revolutionized PHF fixation. These plates provide angular stability, which is particularly beneficial in osteoporotic bone, reducing the incidence of screw pull-out and loss of reduction compared to conventional plating. However, biomechanical studies consistently underscore the critical role of medial calcar support (either through an anatomically reduced medial column or a dedicated calcar screw/medial support plate) in preventing varus collapse and subsequent screw cutout, even with locking plates.
- Clinical Outcomes: Systematic reviews and meta-analyses comparing open reduction and internal fixation (ORIF) via deltopectoral approach versus minimally invasive lateral approaches with locking plates generally report comparable functional outcomes (e.g., Constant score, ASES score) and similar rates of complications like non-union, malunion, and infection. Some studies suggest a trend toward lower rates of avascular necrosis and wound complications with minimally invasive techniques, though this is not universally demonstrated across all literature. The main advantages often cited for minimally invasive techniques are potentially reduced blood loss, shorter hospital stays, and less cosmetic scarring, though these are often secondary to improved soft tissue handling rather than a direct intrinsic superiority of the approach itself in all cases.
- Specific Fracture Patterns: The minimally invasive lateral approach is particularly well-suited for PHFs extending into the humeral shaft or segmental fractures where distal fixation is crucial, allowing direct access to the lateral shaft without extensive proximal dissection. For very comminuted 4-part fractures or fracture-dislocations in the elderly, the evidence increasingly supports primary arthroplasty (hemiarthroplasty or reverse total shoulder arthroplasty) due to high rates of complications and unpredictable outcomes with ORIF, regardless of approach.
- Guidelines: Major orthopedic organizations (e.g., AAOS, OTA) provide treatment algorithms that emphasize individualized patient care. These guidelines typically recommend non-operative management for minimally displaced fractures, while operative intervention with ORIF or arthroplasty is considered for significantly displaced fractures in active patients. The choice of specific ORIF approach (deltopectoral vs. lateral minimally invasive) often depends on surgeon preference, training, and the specific fracture morphology.
- Future Directions: Research continues to explore novel implant designs, biodegradable fixation, role of biologics (e.g., PRP, bone marrow aspirate), patient-specific implants, and the integration of advanced imaging and navigation techniques to further optimize PHF treatment outcomes and minimize complications. The ongoing refinement of surgical techniques, particularly in maximizing the benefits of minimally invasive principles while ensuring robust fixation, remains a primary focus.
Clinical & Radiographic Imaging