Mastering the Minimally Invasive Distal Tibia Approach
Introduction & Epidemiology
Fractures of the distal tibia represent a challenging spectrum of injuries, encompassing metaphyseal, epiphyseal, and intra-articular (pilon/plafond) patterns. These injuries account for approximately 1-10% of all tibial fractures, with pilon fractures alone accounting for 7-10% of all tibial fractures and 1% of all lower extremity fractures. Their incidence peaks in young males involved in high-energy trauma (e.g., motor vehicle accidents, falls from height) and in elderly individuals with osteoporotic bone from low-energy falls. The anatomical characteristics of the distal tibia, notably the broad metaphysis flaring to form the ankle plafond and the critical articular surface, coupled with a precarious soft tissue envelope, render these injuries complex to manage.
The distal tibia has a large subcutaneous surface, making direct access seemingly straightforward. However, the soft tissues overlying the distal tibia are notoriously thin and fragile, consisting predominantly of skin, subcutaneous tissue, and underlying fascia. This paucity of soft tissue padding, combined with the high-energy mechanisms often associated with these fractures, predisposes to significant soft tissue compromise, including extensive swelling, blistering, and profound edema. These issues are exacerbated by underlying patient comorbidities such as chronic venous insufficiency and smoking, which further impair local tissue perfusion and healing capacity. Consequently, the timing of definitive surgical intervention is often delayed, prioritizing soft tissue recovery to mitigate postoperative complications.
The evolution of surgical management for distal tibia fractures has progressed from traditional open reduction and internal fixation (ORIF), often associated with high rates of wound complications, to the adoption of minimally invasive plate osteosynthesis (MIPO). MIPO techniques prioritize indirect reduction strategies and percutaneous plate insertion, aiming to preserve the delicate soft tissue envelope and periosteal blood supply, thereby reducing the risk of wound-related morbidity while achieving stable fixation and anatomical alignment. This approach is particularly advantageous in scenarios where soft tissue compromise is a primary concern.
Surgical Anatomy & Biomechanics
Surgical Anatomy
A thorough understanding of the regional anatomy is paramount for successful application of the minimally invasive approach.
*
Osseous Anatomy:
The distal tibia transitions from a triangular diaphysis to a rectangular metaphysis, which distally broadens to form the ankle plafond. The medial malleolus is a projection from the medial aspect of the distal tibia. The distal articular surface, the plafond, articulates with the talus. The anterolateral aspect features the incisura fibularis, a concave facet for articulation with the fibula, forming the distal tibiofibular syndesmosis. The cortical bone of the distal tibia is relatively thin anteriorly and laterally, becoming thicker posteriorly and medially.
*
Soft Tissue Envelope:
The soft tissue coverage anteriorly and medially is extremely tenuous.
*
Anteriorly:
The skin and subcutaneous tissue directly overlie the extensor retinaculum and the tendons of the tibialis anterior, extensor hallucis longus, extensor digitorum longus, and peroneus tertius. The deep peroneal nerve and anterior tibial artery and veins pass beneath the extensor retinaculum.
*
Medially:
The skin and subcutaneous tissue cover the medial aspect of the tibia, with the saphenous vein and nerve superficial to the medial malleolus. The tibialis posterior tendon and flexor digitorum longus pass posterior to the medial malleolus.
*
Laterally:
The superficial peroneal nerve typically courses anterolateral to the fibula, then divides into intermediate and medial dorsal cutaneous nerves. The peroneal tendons (longus and brevis) run posterior to the lateral malleolus.
*
Blood Supply:
The distal tibia receives its blood supply from the anterior tibial artery, posterior tibial artery, and peroneal artery, which form an anastomotic network around the ankle. Critically, the periosteal blood supply, particularly vulnerable in high-energy injuries, contributes significantly to bone viability and healing. Maintaining periosteal integrity is a cornerstone of MIPO.
*
Ligamentous Structures:
The stability of the ankle joint relies heavily on the deltoid ligament medially, the lateral collateral ligament complex (anterior talofibular, posterior talofibular, calcaneofibular ligaments) laterally, and the distal tibiofibular syndesmosis (anterior inferior tibiofibular, posterior inferior tibiofibular, interosseous ligament). Damage to these structures can impact fracture stability and reduction.
Biomechanics
The distal tibia is a primary weight-bearing bone, transmitting axial loads from the leg to the foot. The ankle joint is a hinge joint designed for dorsiflexion and plantarflexion, but also tolerates limited inversion/eversion and internal/external rotation. High-energy axial loading, often combined with rotational or shearing forces, is the typical mechanism for pilon fractures. The integrity of the articular surface and the restoration of anatomical alignment (length, angulation, rotation) are crucial for load distribution across the ankle joint, minimizing the risk of post-traumatic arthritis. Locking plates provide angular stability, which is highly beneficial in the metaphyseal bone of the distal tibia, where traditional non-locking screws might fail due to poor bone stock or high stress concentrations. The concept of relative stability, achieved through MIPO, allows for callus formation and promotes biological healing in metaphyseal fractures, while anatomical reduction and absolute stability are paramount for the articular surface to minimize incongruity and subsequent arthrosis.
Indications & Contraindications
Indications
The minimally invasive approach to the distal tibia is a versatile technique applicable to a range of pathologies, particularly where soft tissue preservation is a priority.
-
Open Reduction and Internal Fixation (ORIF) of Fractures of the Distal Tibia:
- Distal Metaphyseal Fractures (AO/OTA 43-A): Especially multifragmentary or spiral/oblique fractures where indirect reduction can restore length, alignment, and rotation without extensive stripping.
- Selected Pilon Fractures (AO/OTA 43-B, 43-C): When the articular comminution is limited, amenable to indirect reduction techniques (e.g., ligamentotaxis, percutaneous clamps), and soft tissue concerns preclude an extensive open approach. Often used as part of a staged protocol after initial external fixation.
- Distal tibial shaft fractures extending into the metaphysis.
- Biopsy of Bone Tumors: For suspicious lesions in the distal tibia, a minimally invasive approach allows for tissue sampling with reduced morbidity compared to larger excisional biopsies.
- Corrective Osteotomies: For deformities such as malunion or nonunion, particularly those requiring opening or closing wedges in the metaphyseal region. This preserves the soft tissues for optimal healing of the osteotomy site.
- Malunion/Nonunion: Revision osteosynthesis for existing malunions or nonunions where a stable construct can be achieved with minimal soft tissue disruption.
- Ankle Arthrodesis: In certain cases, minimally invasive plating can be utilized for tibio-talar fusion, particularly for primary fusions where significant deformity correction is not required.
Contraindications
The use of the minimally invasive approach is subject to careful patient and injury assessment.
-
Absolute Contraindications:
- Severe Soft Tissue Compromise: Extensive degloving injuries, active infection, or impending skin necrosis directly contraindicate immediate MIPO due to high risk of wound breakdown and deep infection.
- Active Compartment Syndrome: Requires emergent fasciotomy, typically precluding a minimally invasive approach until the acute soft tissue swelling has resolved.
- Irreducible Intra-Articular Fractures: Pilon fractures with significant articular comminution or displacement that cannot be anatomically reduced indirectly, necessitating direct visualization and open reduction.
-
Relative Contraindications:
- Poor Local Soft Tissue Condition: Significant swelling, blistering, or profuse edema, as stated in the seed content, are common in these fractures. A delay in definitive surgery to allow for soft tissue recovery (e.g., via external fixation) is often prudent.
- Chronic Venous Insufficiency: Impairs venous return and predisposes to persistent edema, increasing the risk of wound complications.
- Smoking: A well-established risk factor for delayed union, nonunion, and wound complications due to impaired microcirculation.
- Severe Peripheral Vascular Disease: Compromised blood supply can significantly impair wound healing.
- Uncontrolled Diabetes Mellitus: Increases susceptibility to infection and wound healing delays.
- Morbid Obesity: Technical challenges in accessing the bone and higher risk of wound complications.
- Extremely Comminuted Intra-Articular Fractures: While MIPO can be part of the strategy, extensive comminution may still necessitate a limited open approach for articular surface reduction.
Operative vs. Non-Operative Indications
| Feature | Operative Indications (Minimally Invasive Plate Osteosynthesis) | Non-Operative Indications |
|---|---|---|
| Fracture Type | Displaced distal tibial metaphyseal fractures (AO/OTA 43-A); selected articular fractures (43-B/C) amenable to indirect reduction. | Stable, undisplaced, or minimally displaced (<2mm) distal tibial fractures without significant angulation or rotation. |
| Fracture Pattern | Spiral, oblique, transverse, or multifragmentary metaphyseal patterns; reducible articular patterns. | Stable non-displaced stress fractures; avulsion fractures without significant displacement or instability. |
| Displacement/Angulation | Significant displacement, angulation (>5 degrees), shortening (>5mm), or rotational deformity. | Minimal displacement (<2mm), acceptable angulation (<5 degrees), no rotational deformity. |
| Articular Involvement | Indirectly reducible intra-articular fractures (e.g., pilon with limited comminution, specific fracture lines). | No articular involvement, or stable, non-displaced intra-articular fractures without step-off or gap. |
| Soft Tissue Status | Closed fractures with good soft tissue envelope (after edema subsides); Grade I/II open fractures without extensive contamination. | Excellent soft tissue condition, no significant edema, blistering, or open wounds. |
| Patient Factors | Ambulatory patient with good physiological reserve, compliant with rehabilitation. | High surgical risk (severe comorbidities), non-ambulatory status, or patient preference for non-operative treatment if indicated. |
| Other Conditions | Corrective osteotomies for malunion/nonunion; biopsy of suspicious lesions; specific cases of ankle arthrodesis. | Not applicable. |
Pre-Operative Planning & Patient Positioning
Pre-Operative Planning
Metabolic pre-operative planning is essential for achieving optimal outcomes and minimizing complications.
1.
Clinical Assessment:
A thorough history and physical examination, including detailed neurovascular assessment of the limb, are mandatory. The condition of the soft tissues (swelling, blistering, open wounds) dictates the timing of surgery.
2.
Radiographic Evaluation:
*
Standard Radiographs:
AP, lateral, and oblique views of the ankle and distal tibia are initial requirements. Full-length tibia films are crucial to assess overall limb alignment and rule out associated proximal injuries, as well as to assess rotation.
*
Computed Tomography (CT) Scan:
Indispensable, especially for pilon fractures, to delineate articular involvement, fragment size, comminution, and to plan reduction strategies and screw trajectories. 3D reconstructions can further aid in understanding complex fracture patterns.
3.
Templating:
Pre-operative templating using radiographs and CT scans is critical. This involves selecting the appropriate plate length (ensuring adequate working length for relative stability in metaphyseal fractures), determining the number and direction of screws, and identifying potential pitfalls (e.g., screw-to-screw impingement, nerve courses). Consideration of specific periarticular locking plates designed for the distal tibia is standard.
4.
Staging:
For high-energy injuries with significant soft tissue swelling or open wounds, a staged approach is often preferred. This typically involves temporary external fixation (spanning the ankle) to restore length, alignment, and provide stability, allowing the soft tissue envelope to recover over several days to weeks ("perc-and-span" technique).
5.
Tourniquet Considerations:
While a tourniquet provides a bloodless field, its use should be weighed against the potential for exacerbating reperfusion injury in already compromised soft tissues. Many surgeons prefer not to use a tourniquet or use it for a limited duration.
Patient Positioning
The correct patient positioning and C-arm setup are fundamental for the success of the minimally invasive approach, which relies heavily on fluoroscopic guidance.
1.
Patient Position:
Position the patient supine on a radiolucent operating table.

The ipsilateral hip may be slightly flexed and abducted, with the knee flexed over a bolster, particularly if a posterior approach to the fibula is anticipated or if gastrocnemius relaxation is desired for distraction.
2.
Limb Alignment:
A small sandbag or bolster should be placed beneath the ipsilateral buttock to correct the natural external rotation of the limb. This maneuver helps to ensure the patella is facing directly anteriorly, indicating a neutral rotational alignment of the tibia. This neutral rotation makes it easier to assess the quality of reduction regarding rotational alignment and provides true AP and lateral radiographic views.
3.
Fluoroscopy Setup:
Ensure that the C-arm can be positioned to obtain true AP and true lateral views of the distal tibia and ankle without repositioning the patient or the limb. This typically involves placing the C-arm on the contralateral side of the patient, allowing it to rotate from a sagittal (lateral) plane to a coronal (AP) plane around the foot and ankle. The foot and ankle should be suspended or placed on a radiolucent support to allow unobstructed views.
4.
Sterile Field:
The limb is prepped and draped from the mid-thigh to the toes, allowing full manipulation of the foot and ankle, and access for potential fibular fixation if required.
Detailed Surgical Approach / Technique
The minimally invasive distal tibia approach typically utilizes an anteromedial or direct anterior trajectory, prioritizing indirect reduction and subcutaneous plate insertion.
Incision Planning and Soft Tissue Dissection
-
Incision Selection:
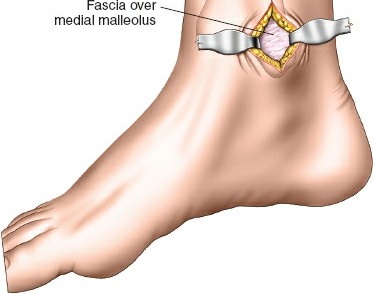
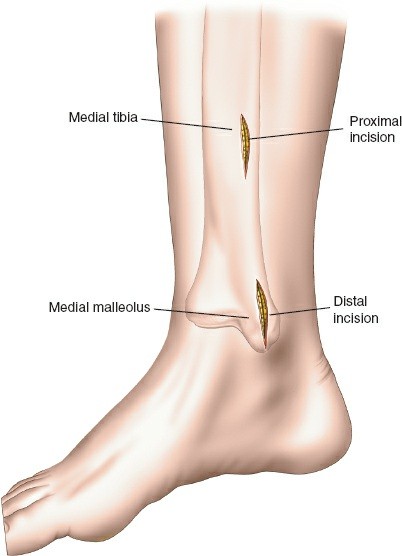
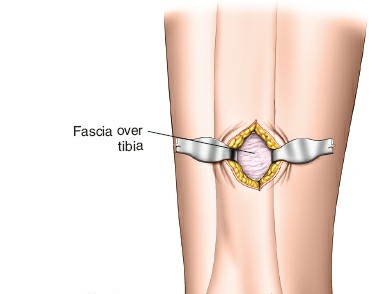
- Anteromedial Approach: Often preferred. A longitudinal incision, typically 3-5 cm, is made proximally and another similar incision distally (or a single longer incision) along the anteromedial aspect of the tibia. The proximal incision is placed away from the fracture zone and the distal incision is typically just proximal to the joint line, usually aligning with the non-articular part of the medial malleolus. The superficial peroneal nerve and saphenous nerve and vein must be identified and protected.
- Direct Anterior Approach: Can also be utilized, with incisions typically placed over the interval between the tibialis anterior and extensor hallucis longus muscles. The deep peroneal nerve and anterior tibial vessels lie deeper and must be protected.
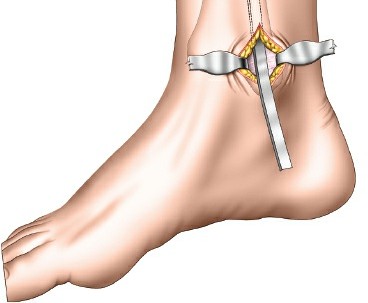
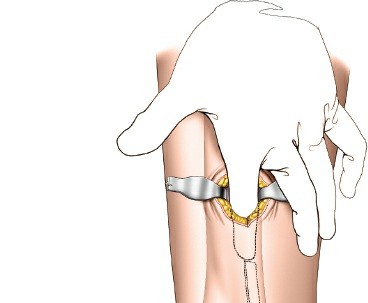
- Subcutaneous Tunnel Creation: After skin incisions, subcutaneous dissection is performed to elevate skin flaps minimally. A submuscular or subcutaneous tunnel is then created, connecting the proximal and distal incisions. This tunnel should be just wide enough to accommodate the plate. Blunt dissection (e.g., using a blunt elevator, specialized plate insertion guide, or fingers) is critical to preserve the periosteum overlying the fracture fragments, which maintains their blood supply and vitality.
- Protection of Neurovascular Structures: Meticulous care must be taken to identify and protect superficial peroneal nerve branches (anterolateral aspect), saphenous nerve and vein (anteromedial aspect), and deep peroneal nerve and anterior tibial vessels (anterior compartment).
Fracture Reduction
The core principle of MIPO is indirect reduction, leveraging existing soft tissue attachments and controlled maneuvers under fluoroscopic guidance.
- Restoration of Fibular Length and Rotation (if fibula fracture present): If a concomitant fibula fracture is present, its reduction and fixation should generally precede tibial fixation. Restoring fibular length and rotation often significantly aids in indirectly reducing the tibia, particularly the syndesmosis.
- Distraction and Ligamentotaxis: Traction can be applied to the foot, either manually, via a fracture table, or through a temporary spanning external fixator, to restore overall length and achieve preliminary reduction of articular fragments via ligamentotaxis.
-
Percutaneous Reduction Tools:
- K-wires as Joysticks: Kirschner wires can be inserted into large, displaced fragments and used as joysticks to manipulate them into alignment.
- Percutaneous Clamps: Specialized pointed reduction clamps can be introduced through small stab incisions to reduce fragments, particularly for angulation and translation.
- Olive Wires: Used to pull or push fragments into position, with fluoroscopic guidance.
- Fluoroscopic Guidance: Real-time fluoroscopy is paramount at every step. AP, lateral, and oblique views are used to confirm reduction in all planes, ensuring restoration of length, alignment (sagittal and coronal), and rotation. Critical attention must be paid to the articular surface for intra-articular fractures.
Plate Insertion & Fixation
- Plate Selection: Precontoured, anatomically shaped distal tibia locking plates are the standard. They are designed to fit the specific contours of the distal tibia and feature multi-directional locking screw options distally. The plate length should be adequate to span the fracture zone, providing sufficient working length (distance between screws nearest to the fracture) to allow for relative stability in metaphyseal fractures.
-
Plate Insertion:
- The chosen plate is carefully slid into the submuscular/subcutaneous tunnel created earlier, from either the proximal or distal incision.
- A plate inserter handle or targeting guide may be used to maneuver the plate and align it correctly on the bone surface.
- Confirm plate position with fluoroscopy (AP and lateral views), ensuring it is centered on the bone and its distal extent is appropriate relative to the joint line.
-
 - The plate should ideally rest directly on the bone, minimizing soft tissue tension.
- Temporary Fixation: Once the plate is positioned, it can be temporarily secured to the bone using K-wires or a plate-holding clamp through designated holes. This allows for final adjustments before permanent screw insertion.
-
Screw Placement:
- Distal Locking Screws: These screws are inserted first to secure the plate to the distal fragment(s). Using the plate's targeting guide, drill guides are utilized to ensure accurate placement of locking screws. Fluoroscopy is critical to confirm that screws are not entering the ankle joint. Typically, 3-4 divergent locking screws are placed in the distal fragment to maximize pullout strength and angular stability.
-
 - Proximal Screws: Proximal locking screws are then inserted into the tibial diaphysis. The number and type (locking vs. non-locking cortical) depend on the fracture pattern and bone quality. For metaphyseal fractures, often 3-4 locking screws are sufficient proximally to provide adequate stability.
- Lag Screws (Optional): If a large, reconstructible primary fracture fragment is present, a percutaneous lag screw can be inserted prior to plate application to achieve absolute stability of that fragment, followed by plate application for neutralization and additional support.
- Joint Penetration Check: After each distal screw, fluoroscopic images (AP, lateral, and true mortise views, possibly oblique views) are meticulously checked to ensure no intra-articular penetration. Articular cartilage violation can lead to significant post-traumatic arthritis.
-

- Final Assessment: After all screws are inserted, the reduction, alignment, and rotation are re-confirmed with multiple fluoroscopic views. The implant should be well-seated, and the soft tissues should not be under excessive tension.
Wound Closure
The limited incisions are irrigated thoroughly. A meticulous, layered closure is performed, paying attention to subcutaneous tissue and skin to achieve good apposition. Careful skin closure minimizes tension and reduces the risk of wound dehiscence. A sterile dressing is applied.
Complications & Management
Complications following surgical fixation of distal tibia fractures, particularly those involving the articular surface, can be significant. While minimally invasive techniques aim to mitigate soft tissue complications, others remain inherent to the fracture pattern and patient factors.
| Complication | Incidence (Approximate) | Salvage/Management Strategy |
|---|---|---|
| Fracture Malreduction | 10-20% | Early revision internal fixation to achieve anatomical reduction (especially articular). Corrective osteotomy for established malunion. |
| Nonunion/Delayed Union | 5-15% | Biological augmentation (autogenous bone graft, allograft, PRP, BMP). Revision fixation with more stable construct (longer plate, additional screws, compression). External fixation with dynamization or bone transport. Non-weight bearing until union. Electrical stimulation. |
| Malunion | 5-10% | Corrective osteotomy to restore anatomical alignment and limb length. |
| Infection (Superficial/Deep) | 5-10% (superficial), 1-5% (deep) | Superficial: Local wound care, oral antibiotics. Deep: Surgical debridement, intravenous antibiotics. If stable union, hardware removal. If nonunion, staged reconstruction with external fixation or flap coverage. |
| Soft Tissue Complications (Blistering, Skin Necrosis, Wound Dehiscence) | 10-25% (general distal tibia) | Blistering: Expectant management, sterile dressings. Skin Necrosis/Dehiscence: Local wound care, debridement. Negative pressure wound therapy. Delayed primary closure, skin grafting, or rotational/free flap coverage if extensive. |
| Nerve Injury (Superficial Peroneal, Sural, Saphenous) | <5% | Expectant management (most resolve), neurolysis for persistent symptoms. Nerve graft in severe cases. |
| Hardware Irritation/Prominence | 10-20% | Hardware removal after fracture union, typically 12-18 months post-surgery, if symptoms persist. |
| Deep Venous Thrombosis (DVT) | 1-5% | Prophylactic anticoagulation. Therapeutic anticoagulation for diagnosed DVT. Early mobilization. |
| Compartment Syndrome | Rare (typically early post-trauma) | Emergent fasciotomy. |
| Post-Traumatic Arthritis | 10-30% | Physiotherapy, activity modification, NSAIDs. Intra-articular injections. If severe, ankle arthrodesis, total ankle arthroplasty (rare for post-traumatic), or distraction arthroplasty. |
| Loss of Reduction/Fixation Failure | <5% | Revision internal fixation with a stronger construct or alternative fixation method (e.g., external fixation, intramedullary nail in selected cases). Bone grafting if associated with nonunion. |
Post-Operative Rehabilitation Protocols
A structured and individualized rehabilitation protocol is crucial for optimizing functional outcomes following minimally invasive distal tibia fixation. The protocol must be tailored to the specific fracture pattern, quality of fixation, patient comorbidities, and progress of bone healing.
Initial Phase (0-2 weeks post-op)
- Weight Bearing Status: Strict non-weight bearing (NWB) on the operative extremity. Ambulation with crutches or a walker.
- Protection: Splint or removable boot for comfort and protection, especially during transfers.
- Pain & Swelling Management: Elevation of the limb above heart level, regular ice application, and prescribed analgesics.
-
Range of Motion (ROM):
- Initiate gentle active and passive ankle ROM exercises (dorsiflexion/plantarflexion, inversion/eversion) as tolerated, within pain limits , ensuring NWB.
- Toe flexion and extension exercises.
- Avoid stressing the fracture site.
- Wound Care: Daily inspection of incision sites. Dressing changes as per surgeon's instructions.
- DVT Prophylaxis: Pharmacological and mechanical prophylaxis as indicated.
Intermediate Phase (2-6/8 weeks post-op)
- Weight Bearing Status: Progress to partial weight bearing (PWB) in a protective boot or orthosis, typically around 6-8 weeks post-op, contingent upon radiographic evidence of early callus formation and stable fixation. Gradual increase in weight bearing as tolerated, progressing to full weight bearing (FWB) by 10-12 weeks.
- ROM: Continue and gradually increase active and passive ankle ROM exercises. Incorporate gentle stretching.
-
Strengthening:
- Initiate isometric strengthening exercises for ankle dorsiflexors, plantarflexors, invertors, and evertors.
- Progress to light resistance exercises using resistance bands.
- Begin hip and knee strengthening exercises for the operative limb.
- Proprioception/Balance: Once PWB is established, begin basic balance exercises (e.g., single leg stance with support).
- Gait Training: Focus on proper gait mechanics with assistive devices.
Advanced Phase (8-12+ weeks post-op)
- Weight Bearing Status: Progress to full weight bearing (FWB) out of the boot, as tolerated, once radiographic union is confirmed (typically by 12 weeks, but variable).
- ROM & Flexibility: Continue to maximize ankle ROM and flexibility.
-
Strengthening:
- Progress to more advanced resistance training for the ankle and lower leg.
- Incorporate eccentric exercises.
- Calf raises (bilateral, then unilateral).
- Functional exercises (e.g., squats, lunges).
- Proprioception/Balance: Advanced balance exercises (e.g., wobble board, uneven surfaces, sport-specific drills).
- Activity Progression: Gradual return to activities of daily living. Low-impact activities (e.g., cycling, swimming) are encouraged. Return to higher impact activities or sports is typically delayed until 4-6 months post-op, dependent on bone healing, functional recovery, and surgeon's clearance.
Key Considerations for Rehabilitation
- Individualization: Protocols must be highly individualized based on patient factors, fracture stability, and healing trajectory.
- Radiographic Follow-up: Regular clinical and radiographic assessments are essential to monitor fracture healing and guide progression through rehabilitation stages.
- Pain Management: Pain should be a guide; exercises should not cause severe or persistent pain.
- Patient Education: Patients must be educated on weight-bearing restrictions, warning signs of complications, and the importance of adherence to the rehabilitation program.
- Addressing Stiffness: Early, gentle ROM is key to preventing ankle stiffness, a common sequela. If stiffness persists, aggressive physical therapy, static progressive splinting, or in rare cases, manipulation under anesthesia or arthroscopic capsular release may be considered.
Summary of Key Literature / Guidelines
The management of distal tibia fractures has evolved significantly, driven by an improved understanding of soft tissue biology and biomechanics. The minimally invasive plate osteosynthesis (MIPO) technique has emerged as a preferred strategy for selected distal tibia fractures, particularly metaphyseal patterns and certain pilon fractures.
- Reduced Soft Tissue Complications: Numerous comparative studies and systematic reviews have demonstrated that MIPO for distal tibia fractures is associated with significantly lower rates of wound complications, including infection, dehiscence, and skin necrosis, compared to traditional open reduction internal fixation (ORIF) approaches. This is attributed to the preservation of the periosteal blood supply and minimal soft tissue stripping.
- Comparable Union Rates and Functional Outcomes: Despite the indirect nature of reduction, MIPO has shown comparable rates of fracture union, nonunion, and malunion to ORIF techniques. Functional outcomes, as assessed by various ankle outcome scores (e.g., Olerud and Molander Ankle Score, AOFAS score), are also generally similar between MIPO and ORIF, with some studies suggesting a trend towards better early outcomes for MIPO due to reduced soft tissue morbidity.
- Importance of Staged Protocol: For high-energy pilon fractures with significant soft tissue swelling, the "pilon protocol" involving initial spanning external fixation followed by delayed definitive internal fixation (often MIPO) after soft tissue recovery is a widely accepted and evidence-based strategy. This staged approach has been shown to reduce the overall complication rate.
- Articular Reduction in Pilon Fractures: While MIPO emphasizes indirect techniques, anatomical reduction of the articular surface remains paramount for pilon fractures. In cases of significant articular comminution or displacement that cannot be achieved indirectly, a limited, direct open approach may be necessary for reduction and stabilization of the articular fragments, often supplemented by a MIPO approach for metaphyseal fixation.
- Role of Locking Plates: Periarticular locking plates are now considered the implant of choice for unstable distal tibia fractures, particularly in osteoporotic bone or comminuted patterns. Their angular stability provides superior fixation strength and allows for early mobilization without compromising reduction.
- Fibular Fixation: Concomitant fibula fractures, especially those compromising ankle stability or affecting tibial reduction, should be addressed. Fixation of the fibula (often with a small plate or IM nail) can help restore ankle mortise anatomy and facilitate tibial length and alignment restoration.
- Limitations: The primary limitations of MIPO include the reliance on fluoroscopic imaging, which requires expertise and can involve higher radiation exposure, and the technical challenge of achieving precise anatomical reduction of articular fragments without direct visualization in highly comminuted pilon fractures.
In summary, the minimally invasive distal tibia approach, primarily through MIPO, represents a refined surgical strategy that respects the challenging soft tissue environment of the distal tibia. When applied judiciously, with meticulous pre-operative planning, precise execution, and a commitment to protecting the biological milieu, it offers a robust solution for complex distal tibia pathologies, aiming to optimize fracture healing and functional recovery while mitigating surgical morbidity.
Clinical & Radiographic Imaging