MIDFOOT FRACTURES AND DISLOCATIONS: ANATOMY AND BIOMECHANICS
The midfoot serves as the critical biomechanical transition zone between the highly mobile hindfoot and the rigid forefoot lever arm. Comprising the navicular, cuboid, and the three cuneiforms, the midfoot is organized into two distinct longitudinal columns. The medial column (talus, navicular, medial cuneiform, and first metatarsal) is relatively mobile and essential for shock absorption and load transfer. The lateral column (calcaneus, cuboid, and fourth/fifth metatarsals) is more rigid, providing a stable fulcrum for propulsion.
Fractures and dislocations in this region—whether isolated tarsal fractures or complex fracture-dislocations of the Chopart or Lisfranc joints—threaten the structural integrity of the plantar arch. The overarching surgical goals are the restoration of articular congruity, maintenance of column length, and re-establishment of a plantigrade, pain-free foot.
FRACTURES OF THE TARSAL NAVICULAR
The tarsal navicular is the keystone of the medial longitudinal arch. Fractures of the navicular are broadly divided into four types: cortical avulsion fractures, tuberosity fractures, body fractures, and stress fractures. While minimally displaced fractures can be managed conservatively in a well-molded, non-weight-bearing cast, displaced fractures of the navicular body demand open reduction and internal fixation (ORIF).
Sangeorzan Classification of Navicular Body Fractures
Sangeorzan et al. classified navicular body fractures into three distinct types, which dictate the surgical approach and prognosis:
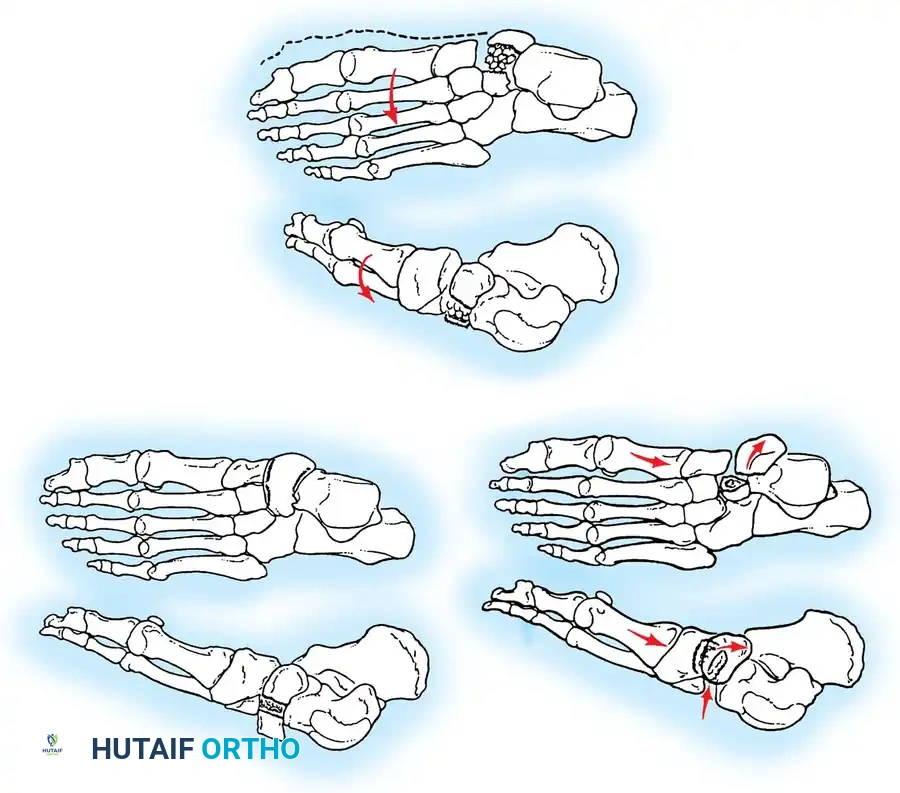
Fig. 86-35: Sangeorzan Classification of Navicular Fractures. (A) Type I: Transverse fracture plane. (B) Type II: Dorsomedial subluxation of the talonavicular joint. (C) Type III: Comminuted fracture with lateral deviation of the forefoot.
- Type I: The fracture plane is transverse in the coronal plane. The dorsal fragment typically comprises less than 50% of the navicular body. Anteroposterior (AP) radiographs may only show a subtle double cortical shadow at the joint line. Anatomical reduction is usually obtainable.
- Type II: The primary fracture line is from dorsolateral to plantar-medial. The talonavicular joint is frequently subluxated dorsally and medially, accompanied by adduction of the forefoot.
- Type III: A highly comminuted fracture of the navicular body associated with disruption of the cuneiform-navicular joint, lateral deviation of the forefoot, and concomitant injuries to the cuboid or the anterior process of the calcaneus. Reduction is notoriously difficult.
Surgical Approach and Fixation Techniques
Surgical Warning: The blood supply to the navicular enters via the dorsal and plantar surfaces, leaving the central third relatively avascular. Meticulous soft-tissue handling is critical. The periosteum of the navicular must not be aggressively elevated, as this can precipitate avascular necrosis (AVN).
For displaced Type II and Type III fractures, an anteromedial hindfoot approach is utilized.
- Incision: The incision is centered over the anteromedial hindfoot, exploiting the internervous/intertendinous interval between the anterior tibial (tibialis anterior) and posterior tibial (tibialis posterior) tendons.
- Joint Preparation: The talonavicular and naviculocuneiform joints are inspected. Intra-articular hematoma and osteochondral debris are meticulously cleared.
- Reduction and Fixation: Fixation is achieved using smooth Kirschner wires (K-wires) for provisional stability, followed by small fragment AO screws (typically 3.5 mm or 4.0 mm partially threaded cancellous screws) when fragment size permits.



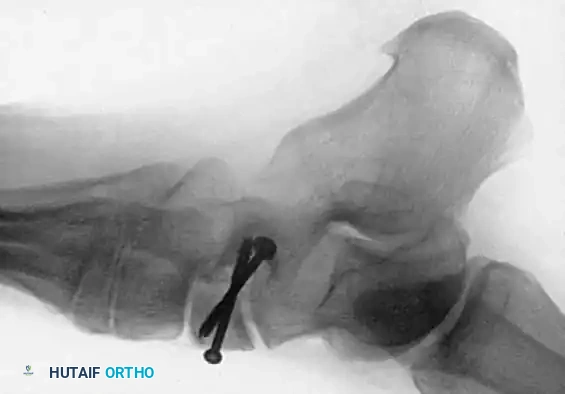

Fig. 86-36: Open reduction and internal fixation of a Type III navicular fracture. Note the severe comminution on the preoperative CT and the restoration of the medial column length postoperatively.
If severe comminution leads to collapse of the navicular and subsequent medial column shortening, structural bone grafting (autograft from the iliac crest) is mandatory. Temporary spanning fixation to the talus or cuneiforms, or the application of a small medial external fixator, may be required to maintain column length during healing. Prolonged recovery and persistent midfoot stiffness are common sequelae.
NAVICULAR STRESS FRACTURES
Navicular stress fractures are a frequent, yet often missed, cause of insidious arch pain in high-demand athletes, particularly track-and-field sprinters and jumpers.
Pathophysiology and Diagnosis
The central third of the navicular is a vascular watershed area, making it highly susceptible to stress failure under repetitive cyclic loading. Patients typically present with vague, increasing arch pain exacerbated by activity. Clinical examination reveals point tenderness over the dorsal navicular ("N-spot") and irritability with forced eversion and inversion.
Routine radiographs are notoriously insensitive in the early stages. A high index of suspicion must prompt advanced imaging. While bone scans are highly sensitive, thin-slice Computed Tomography (CT) in the sagittal and coronal planes or MRI is the gold standard for confirming the diagnosis and assessing fracture completeness. Khan et al. demonstrated that the vast majority of these fractures occur in the sagittal plane within the central avascular third.
Quirk's Treatment Protocol
Based on extensive outcome data, Quirk established a strict protocol for navicular stress fractures:
1. Initial Management: Strict non-weight-bearing (NWB) in a below-knee cast for 6 weeks. (Note: Limitation of activity without casting yields an unacceptable 38% success rate).
2. Re-evaluation: If localized tenderness persists at 6 weeks, an additional 2 weeks of NWB casting is applied.
3. Return to Play: Gradual, supervised return to activity only when clinically asymptomatic.
If conservative management fails, or in cases of complete/displaced stress fractures, surgical intervention is indicated. ORIF with bone grafting yields a 67% success rate.
Clinical Pearl: Quirk recommends obtaining a preoperative CT scan with a radiopaque marker placed over the suspected fracture line. This greatly assists in intraoperative localization of subtle, incomplete fracture lines that may be invisible on the dorsal cortical surface.
CUBOID AND CUNEIFORM FRACTURES
Isolated fractures of the cuboid and cuneiforms are exceedingly rare. They are almost universally associated with broader high-energy injury patterns, most notably Lisfranc or Chopart joint disruptions.
Cuboid "Nutcracker" Fractures
Cuboid fractures are classified into avulsion and compression types. Small avulsion fractures occur secondary to severe inversion ankle sprains and are managed symptomatically.
Compression fractures, or "nutcracker" fractures, occur when the cuboid is crushed between the calcaneus and the 4th/5th metatarsal bases during forced forefoot abduction. This results in lateral column shortening.
* Conservative Care: Minimally displaced fractures are treated with a NWB cast for 4 weeks, followed by a weight-bearing cast for 4 weeks, and subsequent arch support.
* Operative Care: Severe displacement with lateral column shortening requires ORIF. The lateral column length must be restored using a distractor, the articular surface elevated, and the resulting void filled with cancellous bone graft. Fixation is achieved with a bridging plate or K-wires.
CHOPART JOINT DISLOCATIONS
Dislocations and fracture-dislocations of the Chopart (midtarsal) joint—comprising the talonavicular and calcaneocuboid articulations—are severe, high-energy injuries. Historically associated with high-speed motor vehicle accidents, the incidence of severe Chopart injuries has paradoxically increased with the advent of vehicular airbags; patients who previously might not have survived now sustain massive blunt force trauma to the floorboard-planted foot.
Richter et al. demonstrated that early operative intervention with anatomical or near-anatomical reduction of the Chopart joint significantly improves functional outcome scores. The poorest outcomes are seen in combined Chopart-Lisfranc fracture-dislocations.
Surgical Exposure: Adequate visualization of the Chopart joint typically requires a dual-incision approach:
1. An anterolateral incision (similar to the approach for subtalar dislocations) to access the calcaneocuboid joint.
2. A dorsomedial incision to access the talonavicular joint.
LISFRANC (TARSOMETATARSAL) FRACTURE-DISLOCATIONS
Injuries to the tarsometatarsal (Lisfranc) articulation represent a broad spectrum of pathology, ranging from subtle, purely ligamentous sprains in athletes to widely displaced, debilitating crush injuries. Myerson reported a 4% annual incidence of Lisfranc injuries in collegiate football players alone.
Anatomy and Biomechanics
The Lisfranc joint complex is inherently stable due to its bony architecture and robust ligamentous restraints. The base of the second metatarsal is recessed proximally between the medial and lateral cuneiforms, acting as a biomechanical "keystone" that locks the tarsometatarsal complex.
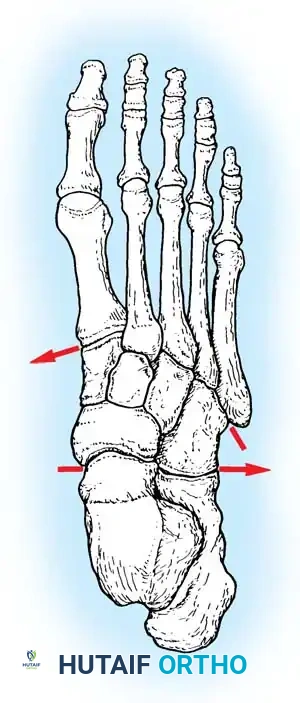
Fig. 86-37: Dorsal view of the foot illustrating the recessed contour of the tarsometatarsal joints, highlighting the keystone base of the second metatarsal.
Notably, there is no transverse ligament connecting the bases of the first and second metatarsals. Stability here relies entirely on the Lisfranc ligament, a stout interosseous ligament running from the lateral aspect of the medial cuneiform to the medial base of the second metatarsal.
Classification of Lisfranc Injuries
While not strictly prognostic, Myerson’s modification of the Quénu and Küss classification is the standard for describing the plane of displacement and magnitude of injury:
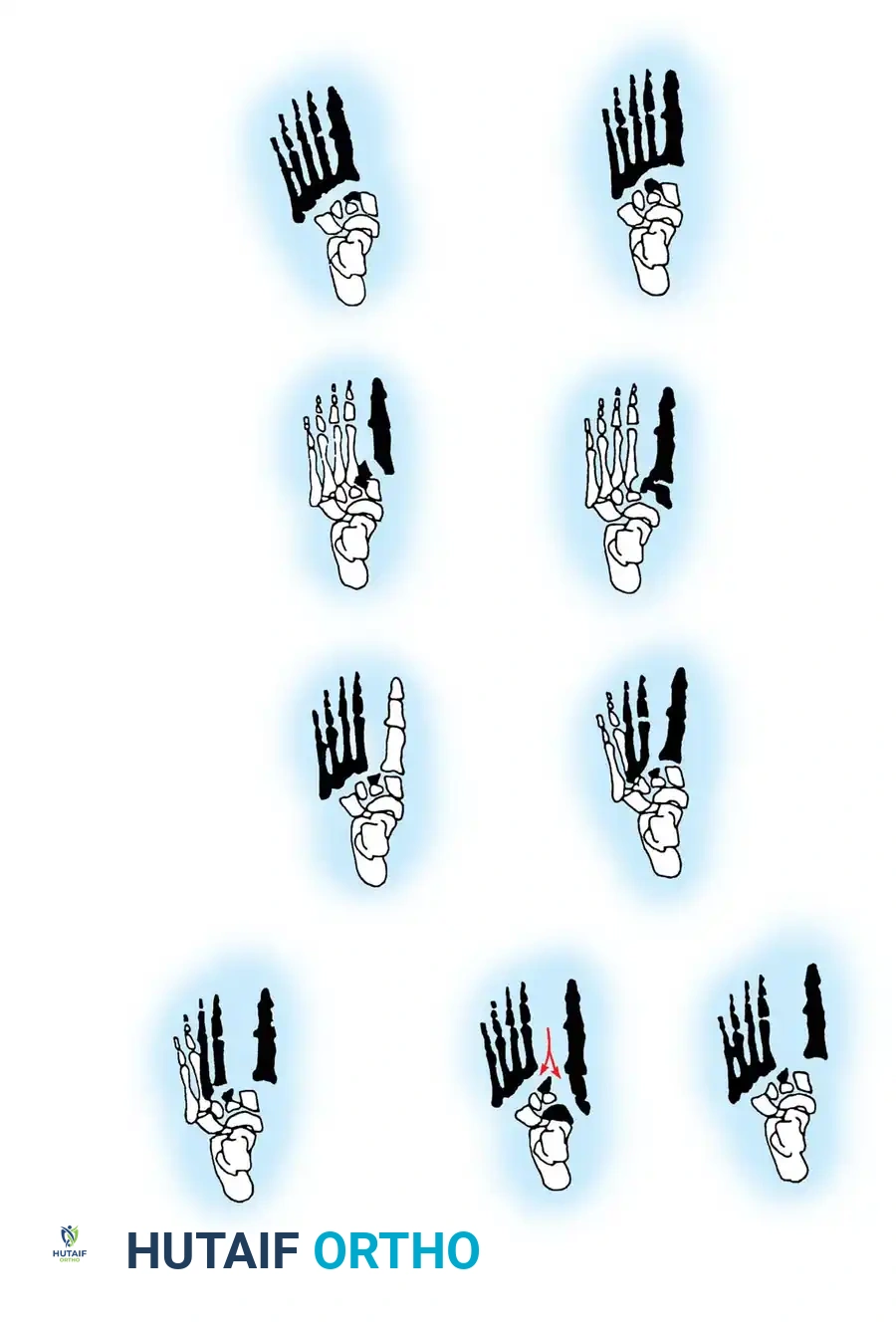
Fig. 86-38: Classification of tarsometatarsal fracture-dislocations (Myerson modification).
- Type A (Total Incongruity): Displacement of all five metatarsals (homolateral), usually laterally or dorsolaterally. The metatarsals move as a single unit.
- Type B (Partial Incongruity): One or more articulations remain intact.
- Type B1: Medial displacement (often involving the 1st metatarsal-cuneiform joint).
- Type B2: Lateral displacement of the lesser metatarsals.
- Type C (Divergent): The 1st metatarsal displaces medially, while the lesser metatarsals displace laterally. Can be partial (C1) or complete (C2). These are highly unstable, high-energy injuries prone to compartment syndrome.
Clinical and Radiographic Evaluation
Subtle Lisfranc injuries are easily missed. A high index of suspicion is required for any patient presenting with midfoot pain and swelling following an axial load to a plantarflexed foot.
* Clinical Signs: Plantar ecchymosis is considered pathognomonic for a midfoot injury until proven otherwise. The "Rotation Test" (Trevino and Kodros)—elevating and depressing the 2nd metatarsal head relative to the 1st—will elicit severe pain at the Lisfranc joint. Inability to bear weight is a red flag.
* Radiographic Evaluation: True weight-bearing AP, lateral, and 30-degree oblique radiographs are mandatory. If the patient cannot bear weight, a NWB cast is applied for 2 weeks, followed by repeat weight-bearing films.
Critical Radiographic Parameters:
1. AP View: The medial shaft of the 2nd metatarsal must align perfectly with the medial aspect of the middle cuneiform.
2. Oblique View: The medial shaft of the 4th metatarsal must align perfectly with the medial aspect of the cuboid.
3. Lateral View: The dorsal cortices of the metatarsals should be flush with the cuneiforms (no dorsal subluxation).
4. The "Fleck Sign": A small bony avulsion fragment in the space between the medial cuneiform and the 2nd metatarsal base represents an avulsion of the Lisfranc ligament and indicates gross instability.
If plain films are equivocal but clinical suspicion remains high, MRI is highly sensitive for identifying acute Lisfranc ligament tears.
Compartment Syndrome of the Foot
High-energy Type C divergent injuries carry a significant risk of acute compartment syndrome of the foot. Failure to decompress leads to devastating ischemic contractures, rigid claw toes, and chronic neuropathic pain. Diagnosis is primarily clinical (tense swelling, pain out of proportion, pain with passive toe stretch), though compartmental pressures can be measured.
Surgical Technique (Manoli Decompression):
We prefer a dual-incision technique to release all nine compartments of the foot.
1. A long medial incision is used to decompress the abductor hallucis, the deep calcaneal compartment, and the medial plantar structures.
2. Two dorsal incisions (one between the 2nd/3rd metatarsals, and one between the 4th/5th metatarsals) are utilized to release the dorsal interosseous compartments.
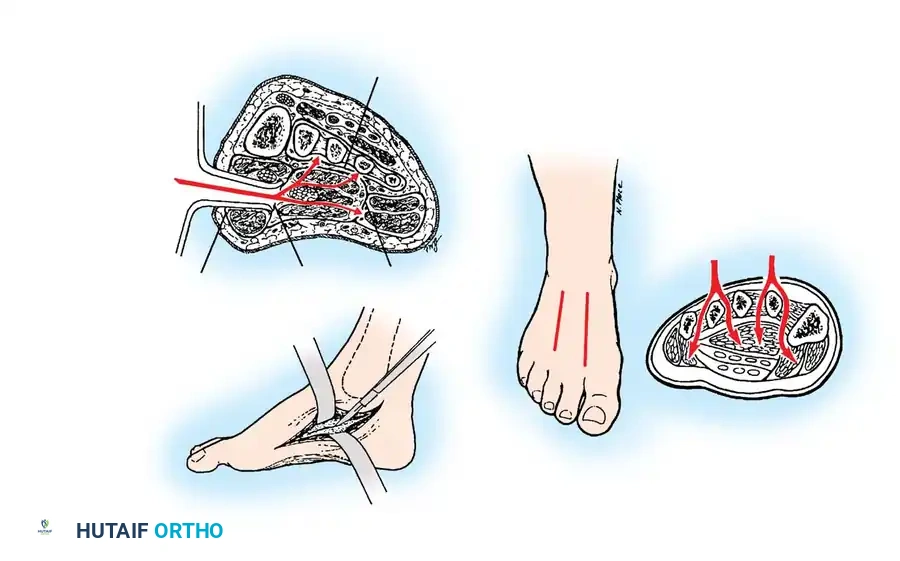
Fig. 86-39: Manoli dual-incision technique for complete fasciotomy and decompression of the foot compartments.
Surgical Management of Lisfranc Injuries
The absolute key to a successful outcome in Lisfranc injuries is rigid, anatomical alignment of the involved joints. Even 1 to 2 mm of displacement leads to altered contact stresses and rapid post-traumatic arthrosis.
While truly non-displaced injuries (< 2 mm on weight-bearing films) can be treated with 6 weeks of NWB casting, any displacement dictates operative intervention.
Open Reduction and Internal Fixation (ORIF):
Closed reduction with percutaneous pinning is rarely sufficient for definitive management due to the interposition of soft tissues (e.g., anterior tibial tendon, peroneus longus) or small osteochondral fragments blocking anatomical reduction. Open reduction is the gold standard.
- Incision: A dorsal longitudinal incision is made centered over the 1st and 2nd metatarsal bases, lateral to the extensor hallucis longus (EHL) tendon. The deep peroneal nerve and dorsalis pedis artery must be identified and protected. A second incision over the 4th/5th metatarsals is used if the lateral column is involved.
- Reduction Sequence: The joints are debrided. Reduction proceeds from medial to lateral. The 1st tarsometatarsal joint is reduced and provisionally pinned. Next, the keystone 2nd metatarsal base is reduced into the cuneiform mortise.
- Fixation:
- Medial Column (1st, 2nd, 3rd TMT joints): Rigid fixation is required. We utilize 4.0-mm cannulated or standard partially threaded cancellous screws. A "home run" screw is typically placed from the medial cuneiform into the base of the 2nd metatarsal, recreating the vector of the Lisfranc ligament.
- Lateral Column (4th, 5th TMT joints): The lateral column requires mobility. Therefore, it is stabilized with smooth K-wires (3/32-inch) rather than rigid screws. These wires are removed at 6 weeks.

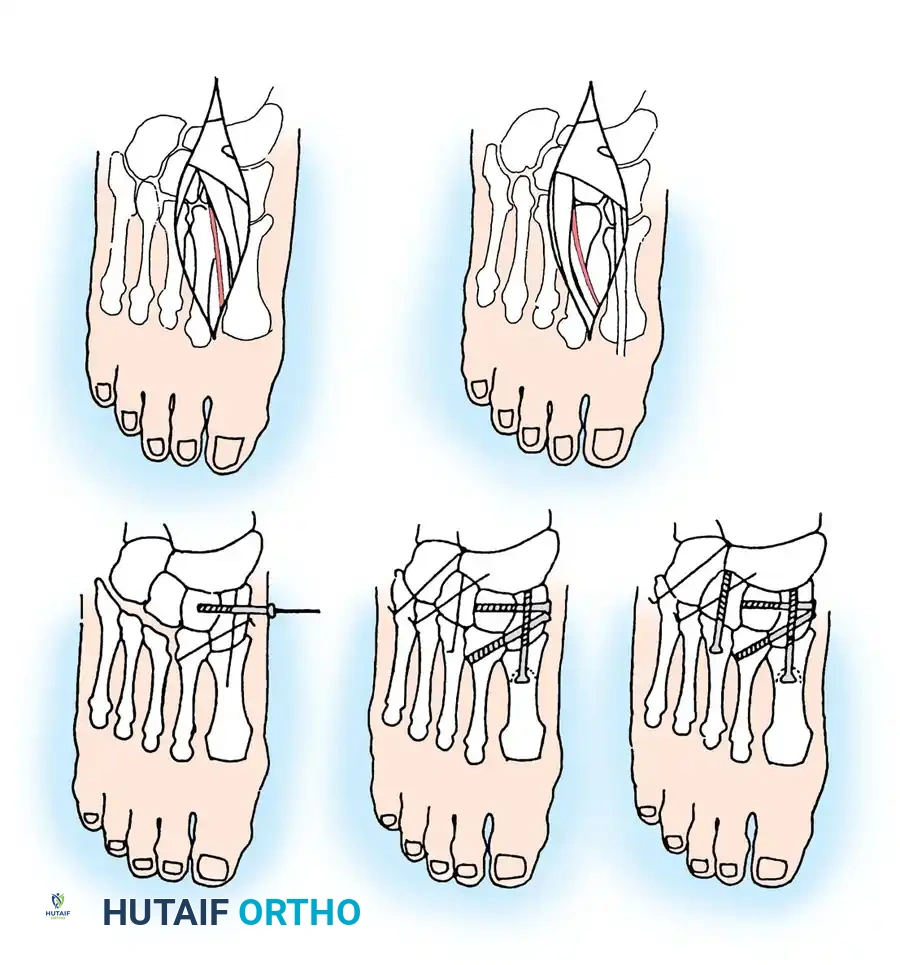
Fig. 86-40: Open reduction and internal fixation of a Lisfranc fracture-dislocation. Note the use of solid screw fixation for the medial and middle columns to ensure rigid stability, while the lateral column is managed dynamically.
Postoperative Protocol:
Patients are placed in a NWB splint for 2 weeks, followed by a NWB cast for an additional 4 to 6 weeks. K-wires stabilizing the lateral column are removed at 6 weeks. Weight-bearing is gradually advanced in a CAM boot. Hardware removal of the medial column screws is generally recommended at 4 to 6 months postoperatively to restore physiologic midfoot motion and prevent screw breakage, though some surgeons prefer to leave them in situ unless symptomatic.
In cases of purely ligamentous Lisfranc injuries or severe comminution where ORIF is impossible, primary arthrodesis of the 1st, 2nd, and 3rd tarsometatarsal joints has shown superior outcomes compared to ORIF, minimizing the risk of hardware failure and secondary degenerative joint disease.
