Introduction to Midfoot Amputations
Midfoot amputations represent a critical juncture in lower extremity limb salvage, offering a functional alternative to below-knee amputations (BKA) for patients suffering from severe trauma, intractable infection, ischemia, or advanced Charcot neuroarthropathy. Amputations through the middle of the foot primarily include the Lisfranc amputation (at the tarsometatarsal joints), the Chopart amputation (at the transverse tarsal joints), and the historically significant Pirogoff amputation (in which the calcaneus is rotated forward and fused to the tibia following a vertical section through its middle).
While these procedures preserve the heel pad and allow for direct end-bearing, they fundamentally alter the biomechanics of the foot. The loss of the anterior lever arm, combined with the sacrifice of key dorsiflexor insertions, creates a profound muscle imbalance. If not meticulously addressed during the index procedure, this imbalance inevitably leads to severe equinus or equinovarus deformities, resulting in anterior stump ulceration, pain, and eventual failure requiring proximal revision.
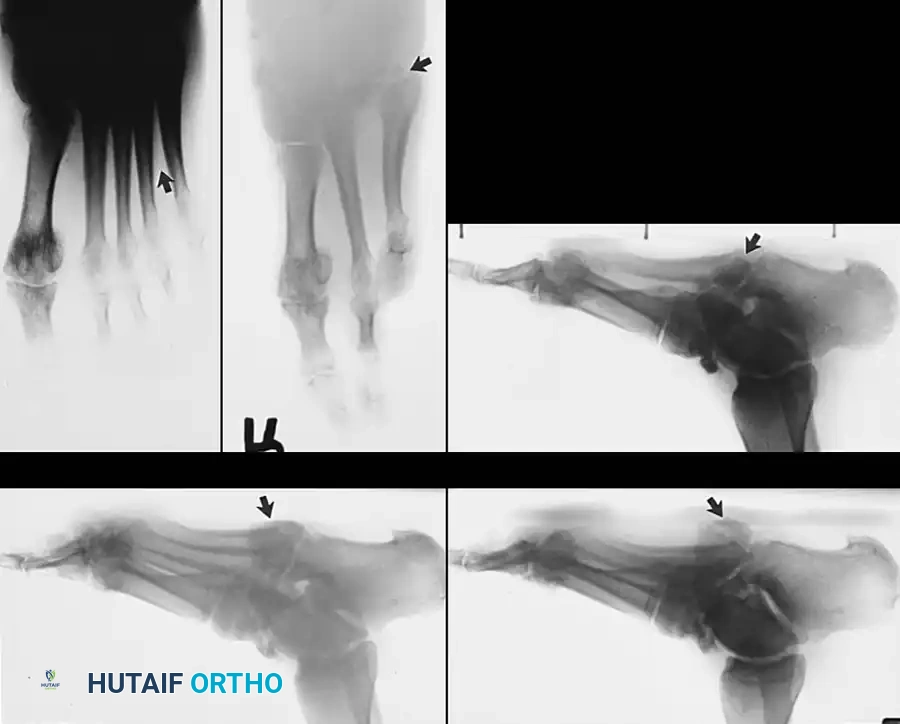
Clinical Pearl: Progressive collapse of the midfoot and hindfoot, often accompanied by a loss of bony architecture, is a hallmark of Charcot arthropathy in elderly patients with diabetes mellitus. Deep plantar space abscesses, osteomyelitis, or neuropathic periostitis frequently follow this collapse deformity, leading to recalcitrant ulceration. In select cases, by osteotomizing the border metatarsal or incising the capsule at the articulation with the tarsus, the gap created by multiple central ray amputations can be closed and managed without the need for complex skin grafts or flap coverage.
Biomechanical Principles and the Equinus Dilemma
The primary challenge in midfoot amputations is the preservation of a plantigrade, braceable stump. The foot functions as a complex lever system; amputating distal to the transverse tarsal or tarsometatarsal joints removes the insertion points of the anterior tibial, extensor hallucis longus (EHL), extensor digitorum longus (EDL), and peroneus brevis and longus tendons.
Consequently, the powerful triceps surae (gastrocnemius and soleus), acting through the Achilles tendon, is left unopposed. This unopposed plantarflexion force rapidly drives the hindfoot into a rigid equinus deformity. Furthermore, the unopposed pull of the tibialis posterior can introduce a severe varus component, resulting in an equinovarus posture where the patient bears weight on the vulnerable anterolateral distal stump.
The Necessity of Achilles Tenectomy
To prevent equinus deformity after midfoot amputations, two critical biomechanical interventions are mandatory:
1. Transfer of Dorsiflexors: One or more dorsiflexors of the ankle must be transferred to the remaining tarsal bones to restore active dorsiflexion.
2. Weakening of Plantarflexors: Lessening the plantarflexion strength of the Achilles tendon is absolutely necessary.
Surgical Warning: A simple Z-lengthening of the Achilles tendon is often insufficient in the setting of a midfoot amputation. The tendon frequently heals and re-tethers, leading to recurrent equinus. Tenectomy of the Achilles tendon—involving the frank removal of 2 to 3 cm of the tendon—is strongly recommended to permanently de-tension the posterior lever arm.
Transmetatarsal Amputation (TMA) Principles
While slightly distal to the true midfoot disarticulations, the transmetatarsal amputation (TMA) shares similar biomechanical principles and is often the preferred initial salvage procedure before progressing to a Lisfranc or Chopart level.
Incision and Osteotomy Planning
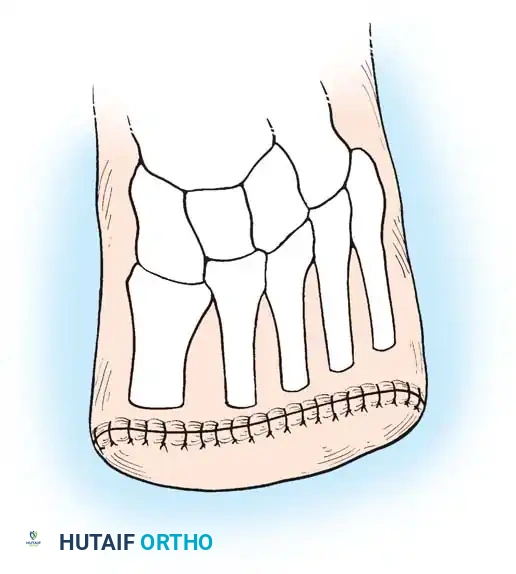
The success of a TMA relies on a robust, well-vascularized plantar flap. The dorsal incision is made straight across the mid-metatarsal shafts, while the plantar incision extends distally to the metatarsal necks before curving proximally.
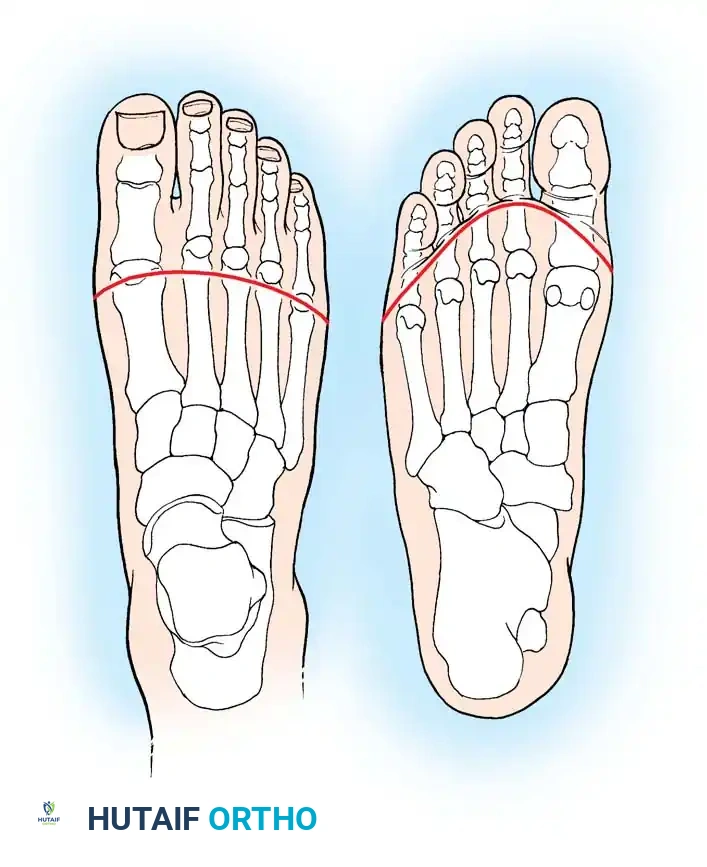
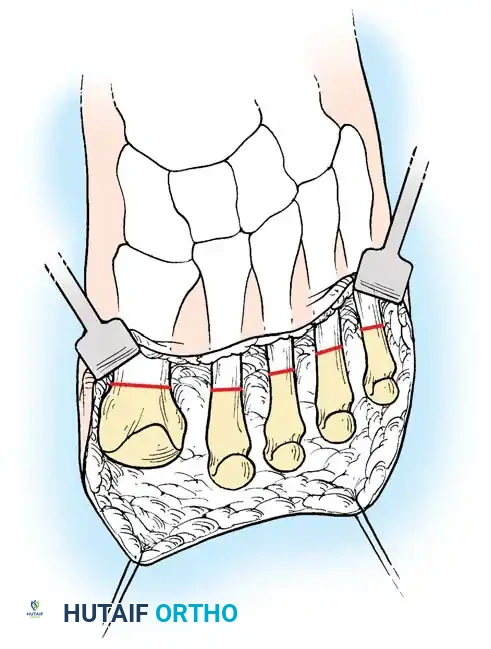
When performing the bone cuts, the level of bone transection must be carefully planned. The osteotomy locations should form a gentle curve, mimicking the natural transverse arch of the foot, with the first metatarsal left slightly longer than the fifth.
Closure
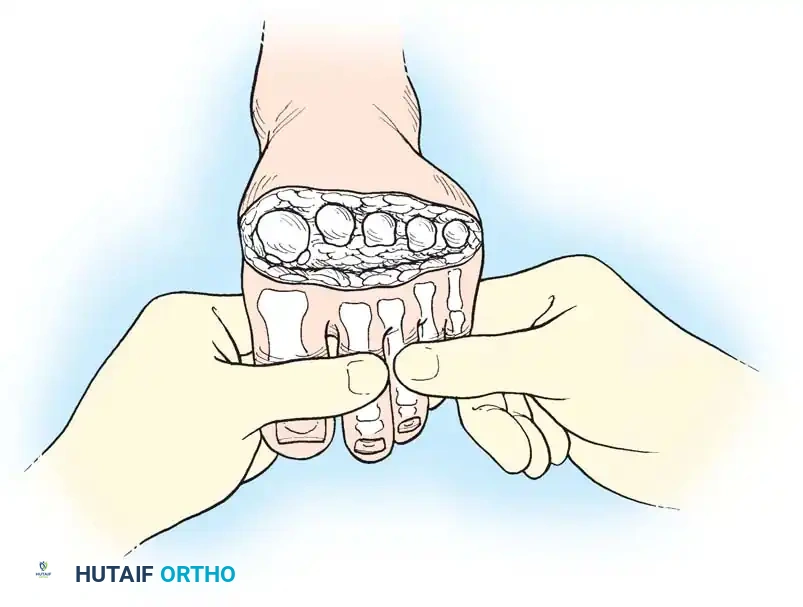
Meticulous soft-tissue handling is paramount. The thick plantar flap is brought dorsally to cover the metatarsal stumps. Closure should be performed in a single layer using monofilament nonabsorbable sutures to minimize tissue reactivity and ischemia at the wound edges.
The Lisfranc Amputation
The Lisfranc amputation involves disarticulation at the tarsometatarsal joints. Historically, this procedure has seldom been performed as a standalone definitive amputation because of the high incidence of equinus deformity that usually develops, which is frequently followed by a severe, unbraceable equinovarus deformity.
When a Lisfranc amputation is deemed necessary (often due to trauma strictly localized to the metatarsals), it must be accompanied by the same aggressive tendon balancing techniques utilized in the Chopart amputation, including Achilles tenectomy and transfer of the tibialis anterior to the midfoot to maintain a plantigrade posture.
The Chopart Amputation (Technique 10-7)
The Chopart amputation is a disarticulation through the transverse tarsal joints (the talonavicular and calcaneocuboid joints). It preserves only the talus and calcaneus. This level provides an excellent, durable heel pad for weight-bearing but requires meticulous surgical technique to prevent the talus from plantarflexing out of the ankle mortise.
Preoperative Planning and Incision
- Flap Design: Mark the skin incision preoperatively, creating a "fish-mouth" flap that is slightly longer on the plantar surface to ensure the weight-bearing heel pad is utilized for distal coverage.
- Incision Execution: Begin the incision at the transtarsal joints medially and laterally. Extend the flaps in a dorsal and plantar direction, creating adequate skin flaps for coverage without tension. Carry the incision sharply through the skin and subcutaneous tissue.
Soft Tissue and Nerve Management
- Nerve Resection: Locate the superficial sensory nerves (superficial peroneal, deep peroneal, sural, and saphenous nerves). Pull them distally, apply gentle traction, transect them sharply, and allow them to retract deep into the proximal soft tissue bed. This traction neurectomy prevents the formation of painful neuromas at the weight-bearing stump interface.
- Tendon Release: Clamp the extensor digitorum longus (EDL) and extensor hallucis longus (EHL) tendons. With distal retraction, incise them and allow them to retract proximally.
- Preservation of the Tibialis Anterior: Carefully dissect the anterior tibial tendon off its insertion at the medial cuneiform and base of the first metatarsal. Preserve its length, as it will be the primary motor unit transferred to balance the foot.
Disarticulation and Bone Preparation
- Joint Release: Identify the transverse tarsal joints (calcaneocuboid and talonavicular). Disarticulate the midfoot by systematically releasing the dorsal, lateral, medial, and plantar ligaments.
- Cartilage Management: While some surgeons prefer to leave the articular cartilage intact, others advocate for shaving the cartilage off the head of the talus and the anterior process of the calcaneus to promote soft-tissue adherence and reduce synovial fluid production.
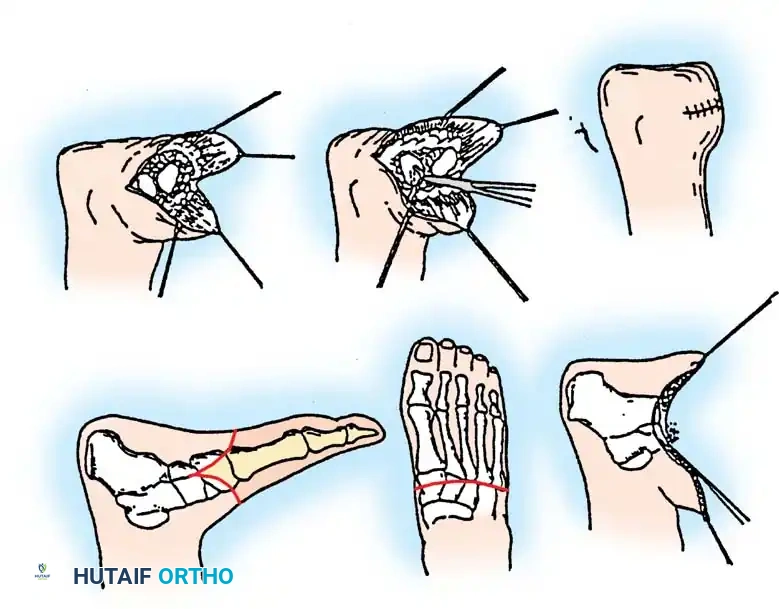
Biomechanical Rebalancing: Tenotomy and Transfers
- Achilles Tenectomy: At this stage, make a separate longitudinal posteromedial incision over the distal Achilles tendon. Perform a radical tenotomy. Excise a full 2 cm of the tendon to completely abolish its plantarflexion force. Attempt to preserve the paratenon and sheath of the Achilles tendon to aid in organized hematoma formation and eventual fibrous bridging. Handle the posterior soft tissues with extreme care to avoid wound healing complications.
- Primary Tendon Transfer: Transfer the preserved anterior tibial tendon to the neck of the talus. This can be achieved by drilling a tunnel through the talar neck or by creating a bony trough and using heavy nonabsorbable suture, bone anchors, or a staple to secure rigid fixation.
Advanced Tendon Balancing: Several authors have suggested that a single tendon transfer (tibialis anterior alone) is inadequate to balance the foot in this setting, as it may not sufficiently counteract varus forces. Alternatives include:
* Transferring the anterior tibial tendon to the neck of the talus AND transferring the peroneus brevis to the anterior process of the calcaneus (to restore eversion/abduction balance).
* Transferring both the anterior tibial and the extensor hallucis longus (EHL) tendons to the neck of the talus, while transferring the extensor digitorum longus (EDL) to the anterior aspect of the calcaneus.
Irrigation and Closure
- Thoroughly irrigate the wound with sterile saline to remove bone debris and hematoma.
- Close the wound as a single layer using interrupted nonabsorbable monofilament sutures. Avoid multi-layer closures that may strangulate the delicate vascular supply of the flaps.
- Apply a well-padded, rigid dressing (short leg cast) with the stump held in slight dorsiflexion.
Salvage of the Equinus Stump
In cases where a tarsometatarsal or midtarsal amputation was previously performed without adequate tendon balancing, a fixed equinus deformity frequently develops. The patient presents with severe pain, skin breakdown, and pressure irritation over the distal anterior stump.
To salvage these failing amputations, Burgess and Lieberman et al. recommend a straightforward but highly effective intervention:
1. Perform a radical division (tenectomy) of the Achilles tendon.
2. Manually correct the equinus deformity.
3. Place the limb in a rigid dressing (cast) in slight dorsiflexion for 6 weeks.
By this means, the equinus is corrected, and weight is borne—as it biomechanically should be—on the thick plantar skin of the heel and the remaining plantar aspect of the foot.
Clinical Outcome: Recurrence of the equinus deformity following this salvage procedure has not been a significant problem. While a slight calcaneus deformity (excessive dorsiflexion) may develop due to the weakened posterior lever arm, it causes no difficulty in fitting a modified shoe or prosthesis, nor does it act as a source of pain. Although terminal "push-off" during the gait cycle is compromised, it is important to recognize that the stump, prior to the lengthening of the Achilles tendon, was already incapable of functional push-off due to the fixed equinus deformity. By this simple method, skin problems, pressure irritation, and pain associated with excessive weight on the end of the stump are largely eliminated.
Postoperative Management and Rehabilitation
The postoperative protocol is as critical as the surgical execution. Premature weight-bearing or inadequate immobilization will lead to failure of the tendon transfers and wound dehiscence.
- Immobilization: The patient should be placed in a slight dorsiflexion rigid dressing (cast) immediately postoperatively. This prevents equinus contracture and removes tension from the anterior tendon transfers.
- Wound Care: The rigid dressing is changed intermittently (typically at 1 to 2 weeks) to inspect the wound.
- Suture Removal: Sutures are kept in place for an extended period, typically 4 to 6 weeks, to allow for adequate healing of the potentially compromised distal soft tissues.
- Tendon Incorporation: The splint or cast must be worn continuously for 6 to 8 weeks to allow for solid bony incorporation of the transferred ankle dorsiflexors and to ensure the Achilles tenectomy site fills with stable, elongated scar tissue.
- Prosthetics: Once fully healed, the patient is fitted with a specialized prosthesis. For a Chopart amputation, this typically involves a custom-molded ankle-foot orthosis (AFO) or a clamshell prosthesis with a rigid sole, rocker bottom, and a custom toe filler to prevent excessive motion within the shoe and to simulate a normal rollover during the stance phase of gait.
📚 Medical References
- midfoot amputations, Clin Orthop Relat Res 361:85, 1999.
- Eginton MT, Brown KR, Sealbrook GR, et al: A prospective randomized evaluation of negative-pressure wound dressings for diabetic foot wounds, Ann Vasc Surg 17:645, 2003.
- Gaine WJ, McCreath SW: Syme’s amputation revisited: a review of 46 cases. J Bone Joint Surg 78B:461, 1996.
- Ger R, Angus G, Scott P: Transmetatarsal amputation of the toe: an analytic study of ischemic complications, Clin Anat 12:407, 1999.
- Greene WB, Cary JM: Partial foot amputations in children: a comparison of the several types with the Syme amputation, J Bone Joint Surg 64A:438, 1982.
- Hansen ST: Salvage or amputation after complex foot and ankle trauma, Orthop Clin North Am 32:181, 2001.
- Harness N, Pinzur MS: Health related quality of life in patients with dysvascular
