Introduction to Metatarsophalangeal Joint Arthroplasty
Metatarsophalangeal (MTP) joint arthroplasty is a foundational procedure in operative orthopaedics, primarily indicated for the correction of severe, rigid forefoot deformities, including chronic MTP joint dislocations, advanced hammer toe deformities, and crossover toe pathology. When conservative measures fail and the deformity becomes fixed, surgical intervention is required to decompress the joint, restore a functional alignment, and alleviate debilitating plantar or dorsal forefoot pain.
The primary goal of resection or contouring arthroplasty at the MTP joint is not to restore normal anatomical kinematics—which is often impossible in chronically contracted joints—but rather to decompress the articulation, allow for concentric reduction of the proximal phalanx onto the metatarsal head, and restore a functional arc of motion.
Clinical Pearl: A successful MTP joint arthroplasty should restore 10 to 20 degrees of motion in an acceptable sagittal plane, ensuring the toe remains concentrically reduced on the metatarsal head without forceful impingement.
Preoperative Evaluation and Pathoanatomy
Chronic dislocation of the lesser MTP joints typically results from a progressive attenuation and ultimate rupture of the plantar plate and collateral ligament complex. This is often exacerbated by a long metatarsal (particularly the second metatarsal) or hallux valgus deformity, which alters forefoot biomechanics and increases sheer forces across the lesser MTP joints.
Clinical and Radiographic Assessment
Patients typically present with intractable metatarsalgia, dorsal PIP joint ulcerations, and a palpable, dorsally displaced proximal phalanx base. Weight-bearing anteroposterior, lateral, and oblique radiographs are mandatory to assess the degree of dorsal subluxation or frank dislocation, the relative lengths of the metatarsals, and the presence of degenerative joint disease.

Clinical appearance of a severe hammer toe deformity with chronic dislocation of the metatarsophalangeal joint.

Preoperative radiographic evaluation demonstrating dorsal dislocation of the MTP joint.
Vascular Considerations and Patient Counseling
Surgical correction of a chronically dislocated toe requires extensive soft tissue dissection, capsular release, and osseous shortening. This places significant tension on the neurovascular bundles.
Surgical Warning: A patient who requires extensive dissection on adjacent joints of the same toe must be advised preoperatively that loss of the toe from vascular compromise could occur. The reoperated toe is particularly vulnerable due to attendant scarring and compromised dorsal venous return.
Surgical Technique: Resection and Contouring Arthroplasty
The following step-by-step technique details the contouring arthroplasty of the metatarsal head combined with intramedullary pinning, designed to manage difficult, rigid deformities.
1. Incision and Exposure
A dorsal longitudinal or elliptical incision is utilized, depending on the need for concurrent skin contracture release.

Planned operative incision over the affected MTP and PIP joints.
The extensor digitorum longus (EDL) and extensor digitorum brevis (EDB) tendons are identified. A Z-lengthening or transverse tenotomy of the EDL is performed to allow access to the dorsal capsule. A thorough dorsal capsulotomy and collateral ligament release are executed to mobilize the base of the proximal phalanx.
2. Proximal Interphalangeal (PIP) Joint Correction
In moderate or severe deformities, the MTP joint cannot be accurately assessed or pinned until the PIP joint contracture is fully corrected.

Exposure after resection of the head and neck of the proximal phalanx, dorsal capsulotomy at the MTP joint, and extensor tendon lengthening.
3. Metatarsal Head Resection and Contouring
To achieve reduction of a chronically dislocated MTP joint, the metatarsal head must be decompressed.
- Distal Resection: Resect 3 to 4 mm of the distal articular surface of the metatarsal head.
- Plantar Condylectomy: It is critical to include the plantar projection (condyles) in this resection. The plantar condyles act as a cam; failing to resect them will maintain tension on the intrinsic musculature and prevent adequate decompression.

Resection of the distal portion of the metatarsal head.

Plantar condylectomy of the metatarsal head to eliminate the cam effect and decompress the joint.
Surgical Pitfall: A word of caution concerning palpable grating of the arthroplasty: If, after contouring the metatarsal head, the MTP joint still feels tight with the proximal phalanx grating on the contoured bone, more bone must be removed until the grating stops. You should be able to passively move the toe 30 to 40 degrees without forceful impingement.
4. Intramedullary Pinning Technique
Once adequate decompression is achieved, the joint must be stabilized with a medullary pin (Kirschner wire) for 3 to 4 weeks to allow the soft tissues to heal in the corrected position.
Antegrade Pinning:
Insert a 0.045-inch or 0.062-inch Kirschner wire antegrade through the remaining shaft of the proximal phalanx, passing it through the PIP joint, middle phalanx, and distal phalanx. The pin should exit in the midline, approximately 2 to 3 mm plantar to the nail bed.
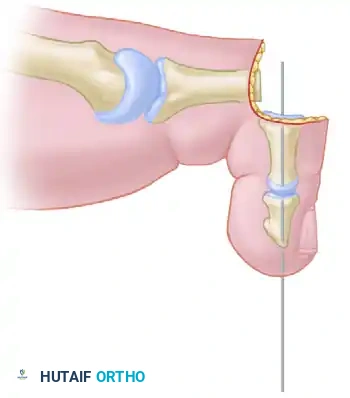
Diagrammatic representation: Pin inserted antegrade through the middle and distal phalanges.

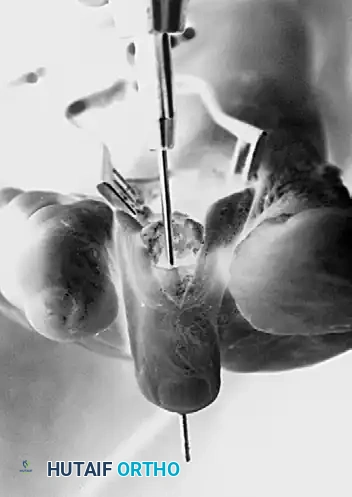
Intraoperative view of antegrade pinning through the proximal interphalangeal joint.
Retrograde Pinning:
Reverse the drill and drive the pin retrograde through the remaining portion of the proximal phalanx shaft.
Technical Tip: Finding the medullary canal of the proximal phalanx can occasionally be difficult. Take a free 0.062-inch K-wire or a small straight hemostat to manually open the canal. This creates a pilot track, allowing the definitive K-wire to find its way without inadvertently exiting the cortex before reaching the proximal articular surface.
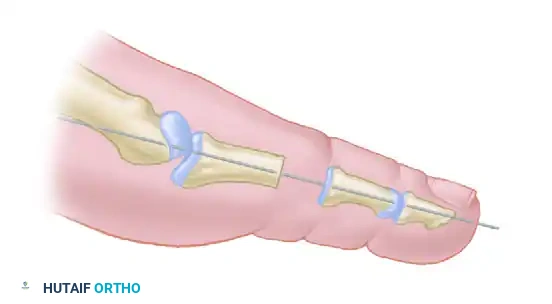
Diagrammatic representation: Pin reversed and driven retrograde through the remaining portion of the shaft of the phalanx and across the MTP joint.
Exit the articular surface of the proximal phalanx near its center. Stand at the head of the table, holding the toe concentrically reduced at the MTP joint (viewing the toe as the patient would see it). Have an assistant drill the pin into the metatarsal shaft.

Intraoperative view of retrograde pinning through the proximal phalanx across the metatarsophalangeal joint.
Critical Positioning Parameters:
* Pin the MTP joint in 10 degrees of extension.
* The ankle must be held at 90 degrees (neutral dorsiflexion) during pinning to accurately assess extensor tension.
* Ensure the joint is perfectly reduced in the mediolateral plane.
5. Soft Tissue Balancing and Closure
- Remove the tourniquet and obtain meticulous hemostasis.
- Resuture the Extensor Digitorum Longus (EDL) in a lengthened position, end-to-end.
- With the ankle joint held at 90 degrees, apply just enough tension on the proximal end of the EDL to bring it out to its resting length. Where the severed ends overlap, excise the redundant proximal portion and repair with 3-0 or 4-0 absorbable suture.
- Close the skin with 4-0 or 5-0 nonabsorbable suture.
Final postoperative appearance demonstrating excellent alignment and K-wire stabilization.
6. Intraoperative Vascular Assessment
After applying a forefoot dressing (taking care not to constrict the toe), evaluate capillary refill. Reducing severe contractures can stretch the neurovascular bundles, leading to ischemia.
Salvage Strategy: If the toe appears vascularly impaired (blanched, lacking capillary refill, or cyanotic), immediately remove the Kirschner wire and allow the toe to "settle" in a shortened position. This relieves tension on the digital arteries. This scenario places additional demands on the postoperative dressing, which must be meticulously applied to hold the unpinned toe in an acceptable alignment.
Advanced Alternative: The Weil Shortening Osteotomy
As an alternative to contouring or resection arthroplasty of the metatarsal head, a shortening osteotomy of the metatarsal neck and head region (the Weil osteotomy) is highly effective for correcting a dislocated MTP joint.
Indications and Biomechanics
The Weil osteotomy is particularly useful if the length of the involved metatarsal (most commonly the second) is excessive in relation to the adjacent first and third metatarsals.
Advantages:
* Preserves the native articular surface.
* Effectively decompresses the joint longitudinally.
* Alters the axis of the interosseous muscles, converting them from dorsal subluxators to plantarflexors, thereby aiding in joint stability.
Surgical Execution of the Weil Osteotomy
The osteotomy is performed intra-articularly, starting at the dorsal margin of the articular cartilage and aiming proximally and plantarly, parallel to the weight-bearing surface of the foot.

Diagram A: Preoperative state of a dislocated MTP joint prior to Weil osteotomy.
Once the cut is complete, the capital fragment is translated proximally to achieve the desired shortening.

Diagram B: Proximal displacement of the metatarsal head fragment, decompressing the joint.
The fragment is temporarily fixed with a K-wire and definitively secured with one or two small fragment snap-off screws. The overhanging dorsal lip of the proximal metatarsal shaft is then resected flush with the articular fragment to prevent dorsal impingement.

Diagram C: Final construct after resection of the distal tip of the dorsal fragment.
Complications of the Weil Osteotomy
While highly successful, the Weil osteotomy carries a 7% to 15% complication rate. The most notorious complication is the "floating toe" deformity, where the toe fails to purchase the ground during the stance phase of gait. Other complications include recurrent instability, transfer metatarsalgia, and joint stiffness.
Strategies to Prevent Floating Toe:
1. Remove a slice of bone: Taking a 1-2 mm parallel slice of bone during the osteotomy prevents excessive plantar translation of the metatarsal head, which can alter the intrinsic muscle mechanics.
2. Plantar Plate Repair: Directly repair the attenuated or ruptured plantar plate if indicated and technically feasible.
3. Flexor-to-Extensor Transfer: Transferring the flexor digitorum longus (FDL) tendon dorsally (Girdlestone-Taylor procedure) provides a dynamic plantarflexion force to the proximal phalanx.
4. Transarticular Pinning: Utilize temporary K-wire stabilization across the MTP joint to hold the toe in neutral alignment while the soft tissues heal.
Postoperative Care and Rehabilitation
Meticulous postoperative care is essential to maintain the surgical correction and prevent recurrent deformity.
- Immediate Post-Op: The foot is kept strictly elevated for 48 to 72 hours to minimize edema and protect the vascular status of the digits. Weight-bearing to tolerance is allowed thereafter, though the use of crutches is optional depending on patient comfort and concomitant procedures.
- Immobilization: A rigid, wooden-soled postoperative shoe is worn for the first 4 weeks to protect the K-wires and prevent bending or breakage.
- Pin Removal: The transarticular Kirschner wire is typically removed in the clinic at 3 to 4 weeks postoperatively.
- Taping and Transition: Following pin removal, the toe must be maintained in the corrected position at both the MTP and PIP joints using a specialized gauze wrap and 1/2-inch tape (e.g., buddy taping or plantarflexion taping).
- Footwear: The patient transitions to a deep, wide, soft-accommodative shoe for an additional 4 to 6 weeks while residual swelling resolves.
Conclusion
Metatarsophalangeal joint arthroplasty, whether achieved through meticulous metatarsal head contouring or a joint-preserving Weil osteotomy, remains a highly reliable solution for severe forefoot deformities. Success hinges on adequate joint decompression, precise soft-tissue balancing, and vigilant postoperative management. By adhering to strict biomechanical principles and respecting the delicate vascular anatomy of the forefoot, orthopedic surgeons can reliably restore function, alleviate pain, and achieve lasting patient satisfaction.
