Comprehensive Introduction and Patho-Epidemiology
Fractures of the metatarsals represent a significant portion of foot and ankle trauma encountered by the orthopedic surgeon, accounting for approximately 5% to 6% of all fractures presenting to emergency departments. Among these injuries, a disproportionate amount of academic, clinical, and surgical attention has been directed toward the treatment of fractures involving the proximal portion of the fifth metatarsal. The historical context of this injury dates back to 1902, when Sir Robert Jones described a fracture at the base of the fifth metatarsal that he sustained while dancing. Since that seminal description, the eponymous "Jones fracture" has become a notoriously challenging clinical entity, plagued by high rates of delayed union, nonunion, and refracture, particularly within high-demand athletic populations.
The unique vascular anatomy of the proximal fifth metatarsal is the primary driver of this challenging clinical course. The bone receives its blood supply from three distinct sources: the nutrient artery, metaphyseal vessels, and periosteal vessels. The nutrient artery enters the medial aspect of the diaphysis and provides endosteal perfusion, while the metaphyseal vessels supply the tuberosity and base. However, anatomical injection studies have consistently demonstrated a critical "watershed" area of relative avascularity at the metaphyseal-diaphyseal junction. When a fracture occurs in this specific zone, the intraosseous blood supply is severely disrupted, and the fracture must rely almost entirely on the tenuous periosteal network for healing, significantly compromising the biological potential for osteogenesis.
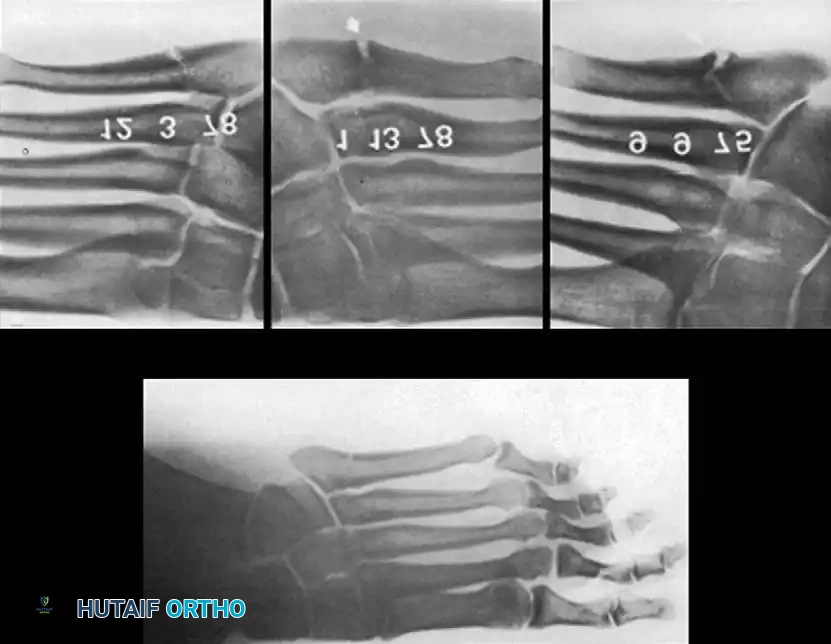
While midfoot trauma can present in various complex patterns, such as divergent Lisfranc fracture-dislocations requiring extensive arthrodesis for stabilization, isolated fifth metatarsal fractures demand a highly specific, classification-driven approach. Accurate classification is the absolute cornerstone of appropriate clinical decision-making. The classification system described by DeLee provides a robust framework based on anatomic location, chronicity, and articular involvement. Type I fractures represent acute injuries at the metaphyseal-diaphyseal junction, further subdivided into nondisplaced (Type IA) and displaced or comminuted (Type IB). Type II fractures occur in the same anatomic location but present with clinical or radiographic evidence of chronicity, such as prodromal pain, cortical hypertrophy, or medullary canal sclerosis. Type III fractures involve the styloid process (avulsion fractures) and are subdivided based on the absence (Type IIIA) or presence (Type IIIB) of fifth metatarsocuboid joint involvement.
Epidemiologically, these fractures exhibit a bimodal distribution. Avulsion fractures (Type III) are more commonly seen in the general population following simple inversion injuries, often associated with lateral ankle sprains. Conversely, metaphyseal-diaphyseal fractures (Types I and II) are predominantly seen in younger, active individuals, particularly competitive athletes participating in sports that require repetitive cutting, pivoting, and jumping, such as soccer, basketball, and football. The immense economic and professional impact of prolonged absence from sport in this demographic has driven a paradigm shift over the last two decades, moving away from prolonged conservative immobilization toward early, aggressive surgical intervention to optimize healing biology and biomechanics.
Clinical Presentation and Diagnostic Imaging
Patients presenting with proximal fifth metatarsal fractures typically report acute onset of lateral foot pain following an inversion or twisting injury, or a history of insidious, progressive lateral foot pain that acutely worsened. On physical examination, there is localized tenderness, ecchymosis, and soft tissue swelling directly over the base of the fifth metatarsal. It is imperative to perform a comprehensive examination of the entire foot and ankle to rule out concomitant injuries, such as lateral ligamentous complex tears, cuboid fractures, or subtle Lisfranc instability.
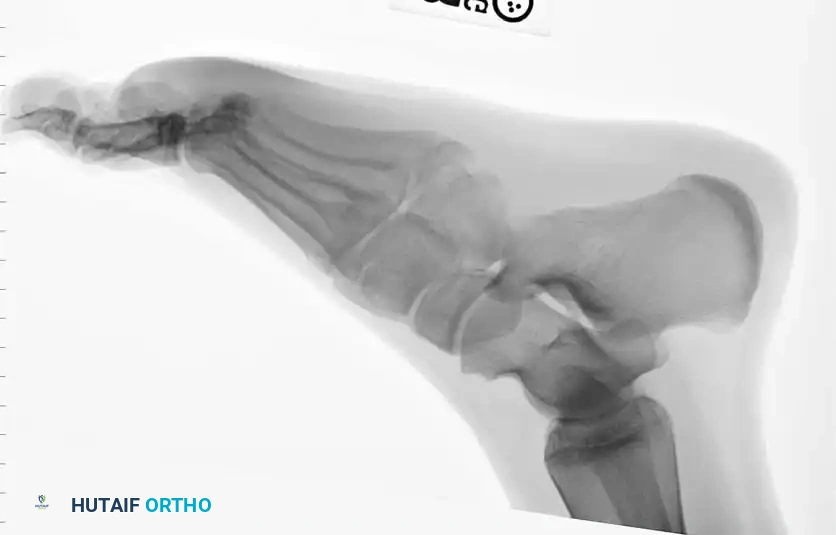
Standard radiographic evaluation must include weight-bearing (if tolerated) anteroposterior (AP), lateral, and 45-degree internal oblique views of the foot. The oblique view is particularly critical, as it profiles the fifth metatarsal base without the superimposition of the cuboid and fourth metatarsal, allowing for accurate assessment of articular extension and fracture displacement. In cases of suspected stress fractures (Type II) where initial radiographs are equivocal, or in elite athletes where immediate definitive diagnosis is required, advanced imaging is indicated. Magnetic Resonance Imaging (MRI) is highly sensitive for detecting bone marrow edema and radiographically occult stress reactions, while Computed Tomography (CT) provides superior bony detail to assess the extent of medullary canal sclerosis, cortical hypertrophy, and precise fracture morphology necessary for surgical planning.
Detailed Surgical Anatomy and Biomechanics
The osteology of the fifth metatarsal is characterized by a complex, multi-planar curvature that is critical to understand for successful intramedullary fixation. Unlike the relatively straight central metatarsals, the fifth metatarsal exhibits a distinct lateral bow in the transverse plane and a plantar bow in the sagittal plane. This intrinsic curvature means that the medullary canal is not a perfectly straight cylinder, but rather a curved tube with a narrow isthmus. Failure to account for this tri-planar bowing during surgical fixation is the leading cause of iatrogenic lateral or plantar cortical blowout during drilling or screw insertion.
The muscular and ligamentous attachments to the proximal fifth metatarsal create a complex biomechanical environment characterized by immense tensile and torsional forces. The peroneus brevis tendon inserts onto the dorsolateral aspect of the tuberosity, acting as a powerful evertor and plantarflexor of the foot. The peroneus tertius inserts dorsally on the metaphysis. Plantarly, the strong lateral band of the plantar fascia inserts onto the plantar aspect of the tuberosity. During the terminal stance phase of the gait cycle, as the heel rises and the patient transitions to the forefoot, the fifth metatarsal is subjected to significant bending moments. The plantar fascia and peroneus brevis exert massive tensile forces on the proximal segment, while ground reaction forces push the distal metatarsal head dorsally, creating a fulcrum effect precisely at the metaphyseal-diaphyseal junction.
These biomechanical forces dictate the distinct mechanisms of injury for the different fracture types. Type III (styloid avulsion) fractures are typically the result of an acute inversion injury to a plantar-flexed foot. The sudden, violent tension from the lateral band of the plantar fascia and the peroneus brevis tendon results in an avulsion of the tuberosity. In contrast, Type I and Type II fractures (the true Jones fractures) occur 1.5 to 3.0 cm distal to the tuberosity. These are primarily caused by vertical or medial-lateral forces applied to the forefoot while the patient's weight is shifted laterally over the fifth ray. In athletes, this is often a repetitive, cyclic loading phenomenon. The continuous microtrauma outpaces the bone's remodeling capacity, particularly in the avascular watershed zone, leading to a stress reaction, cortical hypertrophy, and eventually, a complete fracture.
Surgically, the most critical neurovascular structure in this region is the sural nerve. As demonstrated by Donley et al., the sural nerve bifurcates into a dorsal and a lateral branch. The dorsolateral branch courses directly over the proximal fifth metatarsal, placing it in perilous proximity to the standard surgical incision and the insertion point for intramedullary fixation. Iatrogenic injury to this nerve can result in debilitating neuromas, chronic regional pain syndrome (CRPS), and severe lateral foot numbness. Consequently, surgical approaches must prioritize meticulous soft tissue handling, superficial dissection, and direct visualization and protection of these cutaneous nerve branches.
Exhaustive Indications and Contraindications
The decision-making process for managing proximal fifth metatarsal fractures hinges on a delicate balance between the fracture classification, the biological healing potential, and the patient's functional demands. While non-operative management remains a viable option for many patients, the unacceptably high rates of delayed union and nonunion in specific cohorts necessitate a rigorous, evidence-based approach to surgical indications.
For an acute Type IA fracture in a non-competitive, low-demand patient, conservative management is generally the standard of care. This involves a strict non–weight-bearing protocol in a short leg cast for 6 to 8 weeks, followed by progressive weight-bearing in a controlled ankle motion (CAM) boot. However, orthopedic surgeons must counsel patients that even with flawless compliance, Type I fractures treated conservatively have a reported nonunion rate ranging from 7% to 28%. The adjunctive use of electrical bone stimulation or pulsed electromagnetic field (PEMF) therapy may improve healing rates biologically, but these modalities cannot substitute for the rigid mechanical stability required in high-performance athletes.


Surgical intervention is definitively indicated for Type I fractures that fail to demonstrate clinical and radiographic progression of healing by 8 to 12 weeks. Furthermore, for acute Type IA and Type IB fractures in competitive athletes, early operative intervention is heavily favored. The primary goals in this demographic are to drastically decrease disability time, prevent the biological progression to a nonunion, and allow for an accelerated, predictable return to sport. In these cases, the risk of surgery is vastly outweighed by the risk of prolonged conservative management failure.
Type II fractures, characterized by chronic prodromal pain and radiographic evidence of medullary sclerosis, represent a biological failure of bone healing. While prolonged casting (often exceeding 8 to 10 weeks) may occasionally yield union, the regenerated bone is often biologically inferior and highly susceptible to refracture upon return to activity. Therefore, Type II fractures are a strong indication for surgical intervention, specifically utilizing techniques that re-establish the medullary canal, such as intramedullary reaming with robust screw fixation or the Torg corticocancellous inlay bone graft technique. Type III avulsion fractures rarely require surgery, as they heal predictably with conservative care. Open reduction and internal fixation (ORIF) is reserved only for significantly displaced intra-articular fractures (Type IIIB) involving the metatarsocuboid joint in highly competitive individuals, where restoration of articular congruity is paramount to prevent post-traumatic arthrosis.
| Indication / Procedure | Primary Indications for Surgery | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Intramedullary Screw Fixation | Acute Type I fractures in competitive athletes; Type I delayed unions (>8 weeks); Type II stress fractures with partial sclerosis. | Active local soft tissue infection; Active osteomyelitis; Charcot neuroarthropathy (relative to fixation type). | Severe peripheral arterial disease; Non-compliant patient; Extremely narrow medullary canal (<3.0 mm). |
| Torg Inlay Bone Grafting | Type II/III chronic nonunions with complete medullary sclerosis; Failed previous intramedullary screw fixation; Atrophic nonunions. | Acute Type I fractures (unnecessary morbidity); Active local infection. | Poor soft tissue envelope over the lateral foot; Donor site (iliac crest) morbidity concerns. |
| Conservative Management (NWB Cast) | Acute Type I fractures in sedentary/low-demand patients; Type III avulsion fractures (majority of cases). | Displaced intra-articular Type IIIB fractures with >2mm step-off; Elite athletes requiring immediate return to play. | Polytrauma requiring early weight-bearing on the affected extremity; Severe neuropathy (requires specialized total contact casting). |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the most critical determinant of success in the surgical management of fifth metatarsal fractures. The primary objective is to select an intramedullary implant that provides maximal thread purchase in the dense diaphyseal bone distal to the fracture site, while completely filling the medullary canal to maximize bending stiffness and resist the immense cantilever forces exerted on the proximal segment.
Pre-operative templating relies heavily on high-quality orthogonal radiographs. The surgeon must carefully evaluate the AP and lateral views to determine the narrowest diameter of the medullary isthmus. Historically, a 4.5-mm malleolar screw was considered the gold standard. However, landmark biomechanical studies by Glasgow et al. demonstrated that the use of screws smaller than 4.5 mm was directly associated with catastrophic biomechanical failure, hardware fracture, and clinical refracture. Modern osteosynthesis principles dictate that the largest possible screw that the canal can accommodate should be utilized. Today, 5.5-mm, 6.5-mm, and even 7.0-mm solid or cannulated screws are frequently employed. The surgeon must template the screw length to ensure that all threads bypass the fracture site and engage the distal diaphyseal cortex, typically requiring a screw length between 40 mm and 50 mm.


Patient positioning is critical for facilitating optimal fluoroscopic imaging and surgical access. The procedure is typically performed under regional anesthesia (popliteal sciatic nerve block) with intravenous sedation, or general anesthesia depending on patient preference and comorbidities. A well-padded thigh tourniquet is applied to provide a bloodless surgical field. The patient is positioned either supine with a bump under the ipsilateral hip to internally rotate the leg, or in the lateral decubitus position. The lateral decubitus position is often preferred by high-volume foot and ankle surgeons as it allows the foot to rest naturally on the operative table, providing unobstructed access to the lateral border of the foot and facilitating perfect true lateral and AP fluoroscopic imaging without requiring awkward manipulation of the C-arm.
The fluoroscopy unit should be positioned on the opposite side of the table, entering perpendicular to the patient. Before prepping and draping, the surgeon must verify that perfect AP, lateral, and oblique views of the fifth metatarsal can be obtained easily. The surgeon must appreciate the tri-planar bowing of the metatarsal during this setup phase. Because the bone bows laterally and plantarly, the starting point for the guidewire or drill must be carefully planned. It cannot be directly in the center of the proximal articular surface; rather, it must be positioned "high and inside"—slightly dorsal and medial on the tuberosity—to allow the drill to pass linearly down the curved canal without breaching the lateral or plantar cortices.
Step-by-Step Surgical Approach and Fixation Technique
For Type I and Type II fractures requiring surgical intervention, intramedullary screw fixation remains the workhorse procedure. However, for recalcitrant nonunions with complete obliteration of the medullary canal, the Torg corticocancellous inlay bone graft technique is an invaluable salvage procedure. Both techniques demand a rigorous adherence to anatomic principles and meticulous soft tissue handling.
Surgical Technique: Intramedullary Screw Fixation
As emphasized by Donley et al., percutaneous fixation without direct visualization is fraught with danger due to the variable course of the sural nerve. Therefore, a mini-open approach is mandatory.
- Incision and Exposure: A 2 to 3 cm longitudinal or slightly curvilinear incision is made directly over the proximal 2 cm of the fifth metatarsal, extending proximally toward the cuboid. The incision is carried through the skin and subcutaneous tissues using blunt dissection.
- Nerve Identification and Protection: The surgeon must meticulously identify the dorsolateral and lateral branches of the sural nerve. These branches are mobilized and gently retracted using vessel loops. The deep fascia is incised, and the insertion of the peroneus brevis tendon is identified.
- Tendon Management: The optimal starting portal for the drill is often obscured by the broad insertion of the peroneus brevis. A longitudinal split is made in the tendon in line with its fibers, or a small dorsal portion is carefully elevated off the bone to expose the "high and inside" starting point on the tuberosity.
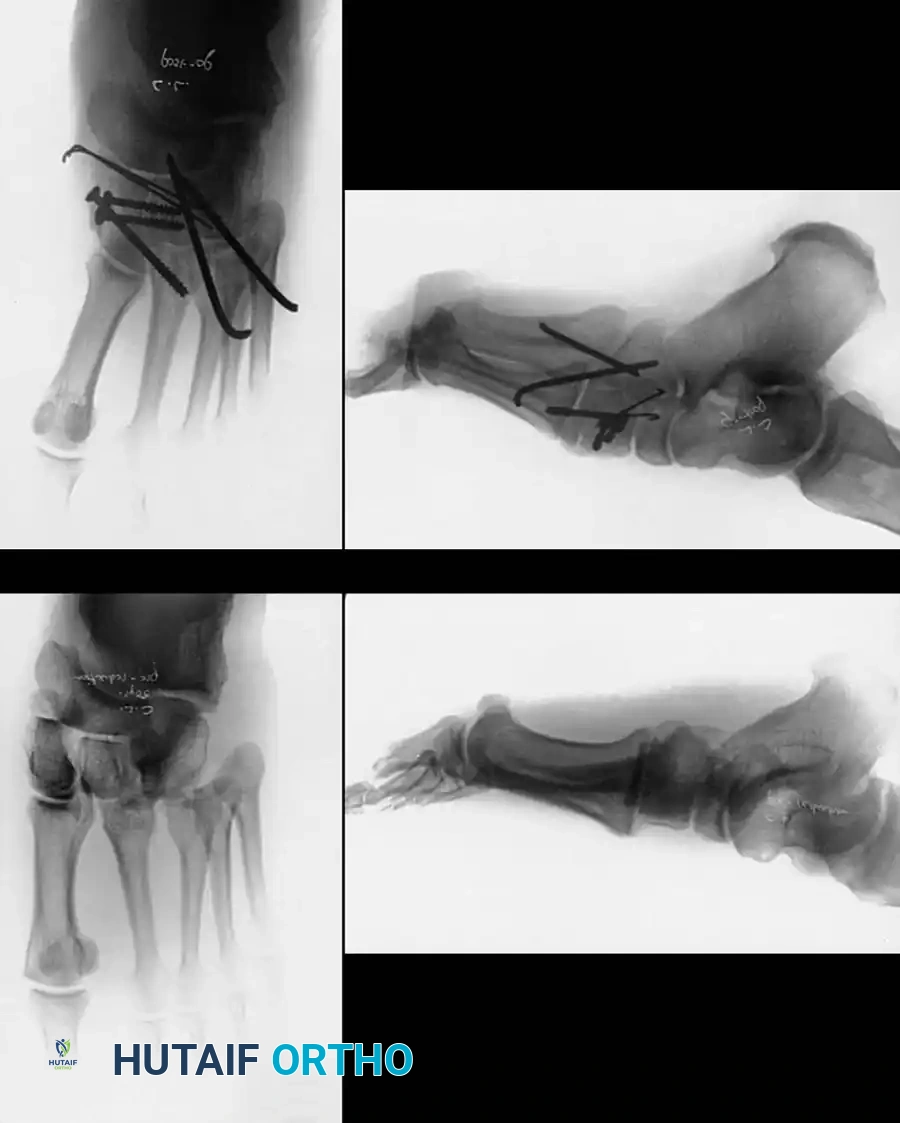
- Guidewire Placement: A 1.6-mm or 2.0-mm Kirschner wire (or the proprietary guidewire for a cannulated system) is introduced into the starting point. Surgical Pearl: The wire must be directed almost parallel to the lateral border of the hindfoot and plantar surface. Multi-planar fluoroscopy is utilized to confirm that the wire is perfectly centered within the medullary canal on both AP and lateral views, bypassing the fracture site by at least 1.5 to 2.0 cm.
- Canal Preparation and Drilling: If using a solid screw system, a 3.2-mm drill bit is driven over the wire trajectory. If using a cannulated system, the cannulated drill is passed over the wire. The surgeon must feel the "chatter" of the drill engaging the dense diaphyseal bone distal to the fracture.
- Tapping: Tapping the narrow isthmus is a critical step. Even if modern screws are self-tapping, pre-tapping the dense diaphyseal cortex with a 3.2-mm or appropriately sized tap prevents excessive torque generation during screw insertion, which is the primary cause of iatrogenic comminution or lateral cortical blowout.
- Screw Insertion: The entry portal is countersunk to allow the screw head to sit flush with the proximal cortex, preventing postoperative hardware prominence and painful shoe wear. The templated screw (e.g., 5.5-mm solid or cannulated, variable pitch or partially threaded) is inserted. The surgeon must observe compression at the fracture site under live fluoroscopy as the screw head engages the proximal cortex.
- Closure: The wound is thoroughly irrigated. The split in the peroneus brevis is repaired with absorbable suture, ensuring the hardware is covered. The subcutaneous tissues and skin are closed in a layered fashion.

Surgical Technique: Inlay Bone Graft (Torg Technique)
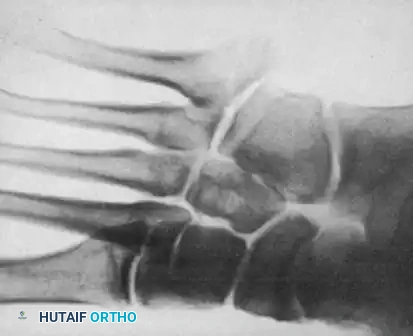
A consistent pathological finding in chronic fifth metatarsal nonunions is the complete obliteration of the medullary canal by dense, avascular sclerotic bone. Torg et al. postulated that this sclerotic bone acts as both a mechanical and biological barrier to osteogenesis. The Torg technique aims to reestablish canal continuity and provide structural osteoconductive and osteoinductive elements via an inlay graft.
- Approach and Osteotomy: The base of the fifth metatarsal is approached through a slightly larger curvilinear dorsolateral incision. The fracture site is exposed subperiosteally. Using a fine drill or a microsaw, a rectangular window measuring approximately 0.7 cm wide by 2.0 cm long is outlined, centered directly over the fracture line.
- Window Removal and Canal Preparation: The rectangular cortical window is carefully removed with a sharp osteotome. The underlying sclerotic bone is aggressively debrided using high-speed burrs and curettes. The surgeon must ream proximally and distally until healthy, bleeding cancellous bone is encountered and the normal continuity of the medullary canal is fully reestablished.
- Graft Harvesting and Placement: A structural corticocancellous bone graft of exact matching dimensions (0.7 cm x 2.0 cm) is harvested, typically from the ipsilateral anterosuperior iliac spine (ASIS) or proximal tibia. The graft is meticulously contoured and press-fit into the rectangular defect. The cortical surface of the graft provides immediate structural stability, while the cancellous portion bridges the medullary defect to stimulate osteogenesis.
- Supplemental Fixation (Modern Modification): While Torg originally described this without hardware, modern surgeons frequently supplement the inlay graft with a low-profile neutralization plate or an intramedullary screw to provide rigid mechanical stability during the incorporation phase.

Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and advanced implants, the surgical management of proximal fifth metatarsal fractures is associated with a specific set of complications. The avascular nature of the watershed zone, combined with the extreme biomechanical forces acting on the lateral column of the foot, makes this procedure unforgiving of technical errors.
The most devastating intraoperative complication is iatrogenic lateral or plantar cortical blowout. This occurs when the surgeon fails to account for the tri-planar bowing of the metatarsal, or utilizes a starting point that is too central or lateral. If the drill or screw breaches the cortex, the mechanical integrity of the fixation is entirely lost. Salvage of an intraoperative blowout requires immediate removal of the intramedullary hardware and conversion to a laterally applied, low-profile locking plate construct to bridge the fracture and the iatrogenic defect.
Postoperatively, delayed union and nonunion remain significant concerns, even following rigid fixation. If a patient presents with persistent pain and radiographic evidence of nonunion at 4 to 6 months postoperatively, a comprehensive workup is required to rule out infection or hardware failure. Salvage of an aseptic nonunion typically requires removal of the existing hardware, aggressive reaming of the sclerotic canal to a larger diameter, placement of a larger intramedullary screw (e.g., exchanging a 4.5-mm screw for a 6.5-mm screw), and the addition of autologous bone marrow aspirate concentrate (BMAC) or a structural Torg inlay graft to optimize the biological environment.
Symptomatic hardware prominence is a frequent complaint, particularly in elite athletes wearing tight-fitting cleats. If the screw head is not adequately countersunk, it can cause chronic irritation of the peroneus brevis tendon or direct pressure against the shoe. Once complete clinical and radiographic union is definitively confirmed (often requiring a CT scan for absolute certainty), the screw can be removed in a minor outpatient procedure. However, surgeons must caution patients that screw removal carries a small but distinct risk of refracture through the empty screw tract.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Sural Nerve Neurapraxia / Neuroma | 5% - 10% | Percutaneous technique; Aggressive retraction; Direct laceration during approach. | Gabapentinoids; Local corticosteroid injections; Surgical excision and burying of neuroma in muscle belly. |
| Lateral/Plantar Cortical Blowout | 2% - 5% | Incorrect starting point (too lateral); Failure to accommodate metatarsal bowing; Oversized rigid drill. | Immediate intraoperative conversion to lateral locking plate fixation; Bone grafting of the defect. |
| Delayed Union / Nonunion | 5% - 15% | Undersized screw (<4.5mm); Inadequate thread purchase distal to fracture; Smoking; Premature weight-bearing. | Exchange nailing to larger diameter screw; Torg inlay grafting; BMAC injection; Extracorporeal shockwave therapy (ESWT). |
| Symptomatic Hardware Prominence | 10% - 20% | Failure to countersink screw head; Extremely thin soft tissue envelope; High-demand footwear (cleats). | Hardware removal only after definitive CT confirmation of complete cortical bridging and remodeling. |
| Hardware Failure (Screw Breakage) | 1% - 3% | Fatigue failure of undersized screw prior to union; Non-compliant early weight-bearing. | Hardware removal (often requires specialized extraction tools); Revision ORIF with larger screw or plate and bone grafting. |

Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation protocol following surgical fixation of a proximal fifth metatarsal fracture is just as critical as the surgical execution. The protocol must be carefully phased to protect the fragile mechanical fixation during the early inflammatory and soft callus phases of bone healing, while progressively loading the bone to stimulate remodeling according to Wolff's Law.
Phase I: Maximum Protection (Weeks 0 - 2)
Immediately post-operatively, the patient is placed in a well-padded, short leg, non-walking splint or cast extending past the toes. The primary goals during this phase are strict elevation to control edema, strict non-weight-bearing (NWB) status utilizing crutches or a knee scooter, and incision healing. The patient is instructed to perform active range of motion of the toes, knee, and hip to prevent deconditioning and deep vein thrombosis. Sutures are typically removed at the 10 to 14-day mark, provided the soft tissue envelope is fully healed.
Phase II: Controlled Mobilization (Weeks 2 - 6)
Following suture removal, the patient is transitioned into a removable controlled ankle motion (CAM) boot. Depending on the rigidity of the fixation and the patient's compliance, the surgeon may allow touch-down weight-bearing (TDWB) or continue strict NWB. The critical component of this phase is the initiation of active range of motion (AROM) of the ankle and subtalar joints out of the boot. Early mobilization prevents arthrofibrosis and stiffness in the hindfoot. However, passive inversion and eversion must be strictly avoided, as these motions place massive tensile stress on the peroneus brevis and the fracture site.
Phase III: Progressive Loading (Weeks 6 - 10)
At the 6-week mark, new orthogonal radiographs are obtained. If there is evidence of early bridging callus and the patient is clinically non-tender over the fracture site, progressive weight-bearing in the CAM boot is initiated. The patient is advanced from partial weight-bearing
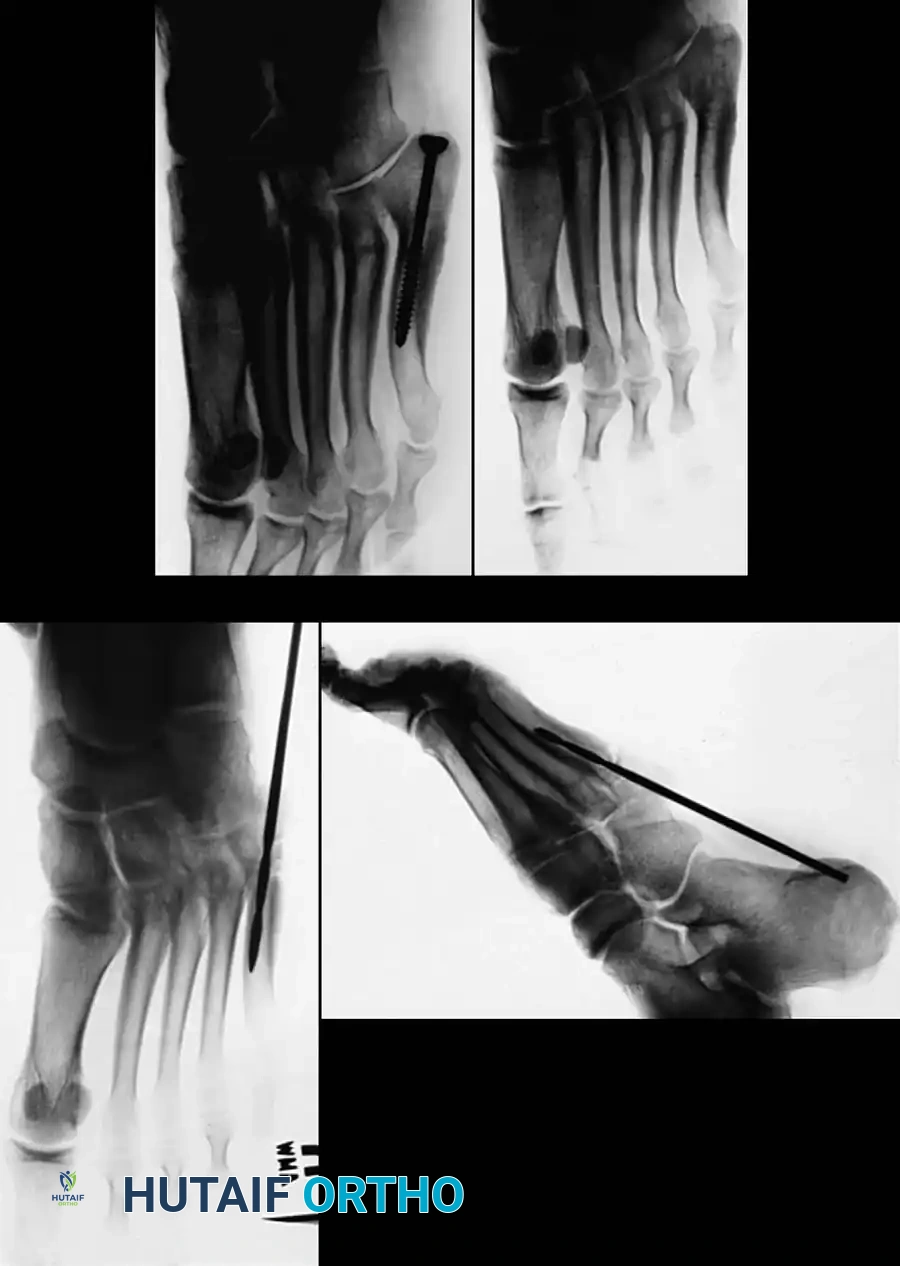
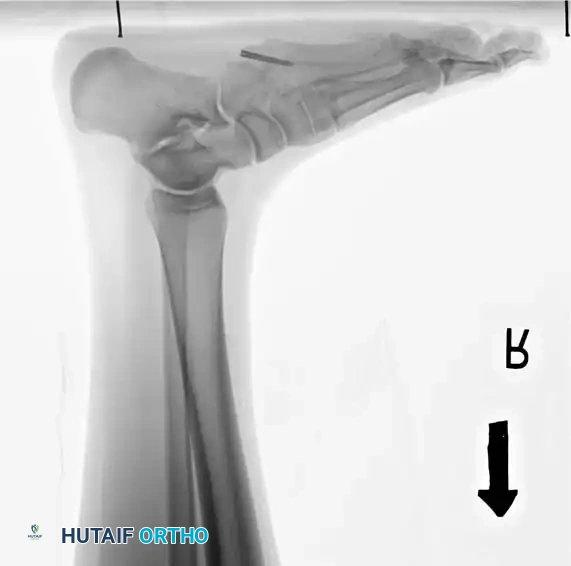
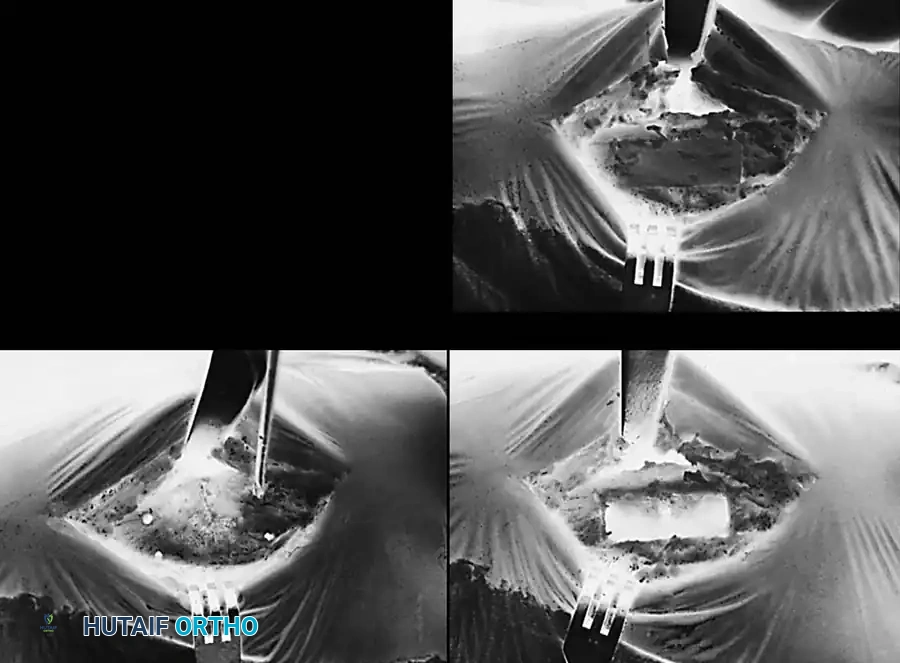
Clinical & Radiographic Imaging Archive