DEFINITION
The finger metacarpophalangeal (MCP) joint is commonly and characteristically involved in inflammatory arthritis.The MCP joint is often involved early in inflammatory arthritis and usually presents with ulnar extensor tendon subluxation resulting in ulnar deviation of the fingers.Occasionally in systemic lupus erythematosus (SLE), radial subluxation of the extensor tendon is seen.
ANATOMY
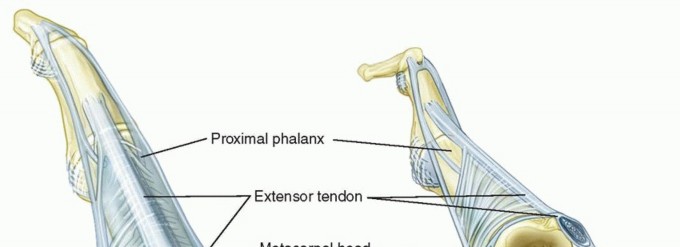


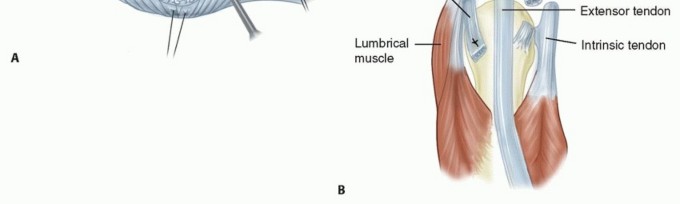
FIG 1 • A. Normal anatomy of the MCP joint. B. Abnormal anatomy seen in inflammatory arthritis. The extensor tendon is subluxated ulnarly. The MCP joint collateral ligaments are asymmetric.The ulnar collateral ligament is more parallel to the long axis of the fingers.The radial collateral ligament is more oblique.This causes supination of the MCP joint with MCP joint flexion.The collateral ligament also resists volar-directed forces.The volar plate is fibrocartilaginous distally and has a membranous portion proximally. It limits MCP joint extension.The transverse intermetacarpal ligament connects the volar plates to each other.The accessory collateral ligament connects the collateral ligament and volar plate and keeps the volar plate close to the volar aspect of the MCP joint throughout motion.The A1 pulley of the flexor tendon sheath is attached to the volar plate.The extensor digitorum tendon is maintained centrally over the MCP joint by the transverse fibers of the sagittal band that attach volarly to the volar plate and the intermetacarpal ligament. This forms a sling mechanism. The ulnar sagittal band is felt to be stronger and denser than the radial sagittal band.P.1085There is usually no direct extensor tendon insertion into the proximal phalanx. The proximal phalanx is extended through the sling mechanism.The lumbrical muscle originates from the tendon of the flexor digitorum profundus and is volar to the intermetacarpal ligament. It inserts into the lateral band.There are three volar (which adduct) and four dorsal (which abduct) interossei that have tendons that all pass dorsal to the transverse intermetacarpal ligament. They have variable insertions into the proximal phalanx and extensor mechanism.The first dorsal interosseous almost always inserts completely into the radial side of the proximal phalanx of the index finger.
PATHOGENESIS
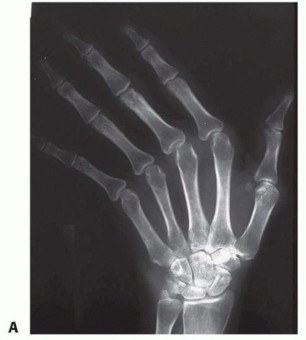
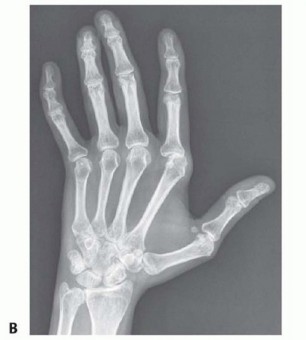
FIG 2 • A. Radiograph of a patient with extensor tendon subluxation and ulnar deviation of the MCP joints. The joint spaces are maintained and the joints are not subluxated. B. Radiograph of a patient with extensor tendon subluxation and ulnar deviation of the MCP joints with reducible MCP joint subluxation involving the index and middle MCP joints. Articular cartilage changes progress from softening of the cartilage to erosion with significant loss of cartilage and bone. This contributes to the deformity.Once there are significant cartilage and bone changes, extensor tendon realignment alone, without joint resurfacing, is not indicated.The changes seen in SLE are secondary not to synovitis but rather to alteration in the collagen that results in a change in the equilibrium of the MCP joint and subsequent deformity.The finger deformity in SLE is often ulnar deviation, but radial deviation is not uncommon.In SLE, it is easy to change one deformity to another (ie, ulnar drift into a radial deviation deformity aftersurgery) because of the global changes to the supporting structures.Despite the MCP deformity becoming fixed, the articular cartilage is usually preserved.
NATURAL HISTORY
The natural history of the MCP joint changes in inflammatory arthritis is not known and is probably highly variable and influenced by the new disease-modifying medications.P.1086Mild ulnar deviation of the fingers is normal and increases with MCP joint flexion.In inflammatory arthritis, such as rheumatoid arthritis, deformity is initially passively correctable.Mild ulnar deviation of the fingers is seen in less than 10% of the patients in the first 5 years of having rheumatoid arthritis.3Ulnar deviation has been reported in 30% of patients with rheumatoid arthritis, with palmar subluxation in 20%.3Palmar subluxation almost always occurs with ulnar deviation.3
PATIENT HISTORY AND PHYSICAL FINDINGS
In a patient with inflammatory arthritis who is being considered for MCP joint surgery, the entire upper extremity is evaluated. Involvement of the lower extremities must also be considered, given that the upper extremities may need to assist in ambulation.The need to use the upper extremities for weight bearing can significantly affect the durability of the correction obtained after MCP joint surgery.Ideally, MCP joint surgery is performed when the upper extremity is not needed for such support.The wrist is evaluated for the presence of a static deformity at the time of MCP joint surgery. Presence of a static radial deviation deformity will negatively affect the results of MCP joint surgery.The skin over the MCP joint is evaluated; it should be in good condition.Motion of the MCP joint is assessed. The surgeon should specifically ensure that ulnar deviation and flexion deformities can be easily corrected passively.Proximal interphalangeal (PIP) joint motion and alignment must be critically evaluated.If there is a significant boutonnière deformity, this should be corrected before the MCP joint surgery because the PIP flexion will influence the amount of MCP joint flexion obtained postoperatively.If there is a swan-neck deformity, this can be treated at the same time or after the MCP joint. A stiff PIP joint in extension will cause the patient to flex the finger at the MCP joint and can help obtain better flexion postoperatively.Any radial or ulnar deformity at the PIP joint must be corrected before the MCP joint surgery.The flexor and extensor tendons must be intact before any MCP joint surgery.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Radiographs of the hand and wrist are essential before MCP joint surgery to evaluate alignment, congruence, and joint integrity.
DIFFERENTIAL DIAGNOSIS
The most common cause of inflammatory arthritis that affects the MCP joint is rheumatoid arthritis.SLE is more common in black women, and the deformity is secondary to a collagen abnormality causing ligament and tendon imbalance. Articular cartilage loss is a much less common problem in SLE. Soft tissue realignment can be performed even after the condition has been present for a long time.Psoriatic arthritis is more common in men and has a characteristic skin rash, although patients may have joint involvement before a clinically obvious skin rash. The patient with psoriatic arthritis often has an asymmetric deformity and more stiffness. The cartilage and bone are also affected. FIG 3 • A splint used to try to prevent progression of the ulnar deviation. Usually, this is not successful and ulnar deviation eventually progresses.
NONOPERATIVE TREATMENT
SURGICAL MANAGEMENT
One of the most difficult operations to decide to perform is MCP joint synovectomy and realignment.This is usually best performed early when there is minimal deformity.However, at this time, the patient often has minimal pain and only slight loss of function.With the use of disease-modifying medications, if the anatomy can be restored and the mechanicalproblems corrected, salvage procedures may be prevented or significantly delayed.The ideal patient for surgery is one with increasing deformity and good medical management with control of his or her synovitis.The deformity should be passively correctable with good active MCP joint motion.Ideally, the MCP joint is not volarly subluxated because correction and maintenance of correction is more unreliable.There should be a well-aligned wrist with good PIP joint function without deformity.If the deformity is passively correctable but cannot be actively corrected, obtaining active ulnar deviation by an extensor carpi ulnaris tendon relocation or transfer should be considered.The radiographs should reveal good preservation of the joint space without volar subluxation.If all of these criteria are met and the joints are not passively correctable or there is volar subluxation of the MCP joint, surgery can be performed, although the results may not be as reliable.2A firm diagnosis can help with establishing a prognosis for the maintenance of correction obtained at surgery.The effect of the new disease-modifying medication is not known.P.1087It is possible that the soft tissue correction obtained at surgery may now last longer and therefore theprocedure should be entertained earlier and more often.Ideally, earlier surgery will solve the correctable mechanical problem and will end the cycle of deformity.
POSITIONING
The procedure is performed using tourniquet control. The hand is supported by a hand table.
APPROACH
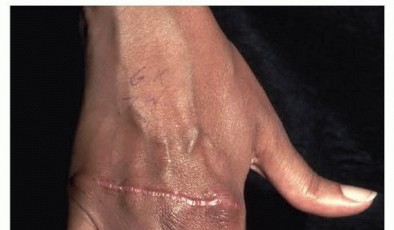
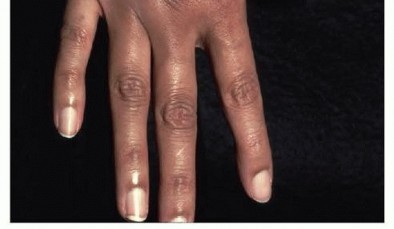
FIG 4 • A transverse incision is used to expose the MCP joints when performing an extensor tendon centralization.
TECHNIQUE
EXPOSURE


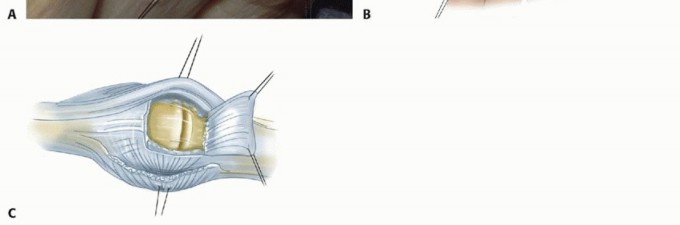
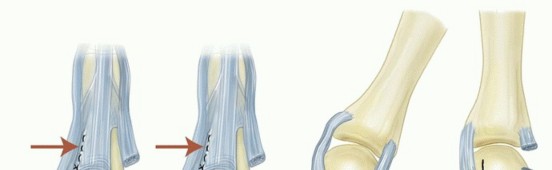
TECH FIG 1 • A. The extensor tendons are exposed through a transverse skin incision. The extensor tendons are subluxated ulnarly. B. The junctura tendinae are released as needed. C. The capsule is opened by creating a distally based dorsal capsular flap.
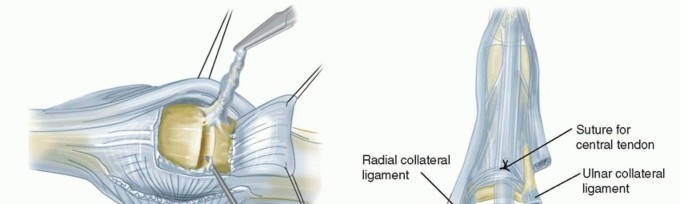
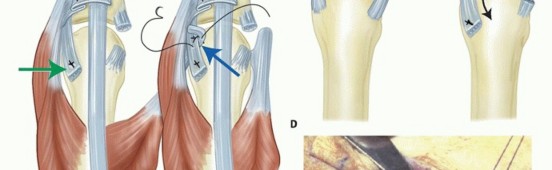
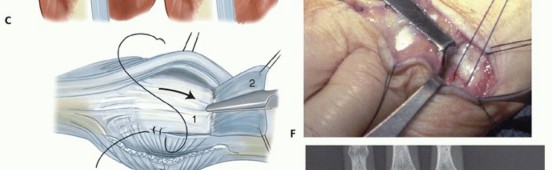
TECH FIG 2 • A. An MCP joint synovectomy is performed. B. The ulnar intrinsic tendon is sectioned and the ulnar collateral ligament is released. The central tendon is centralized and sutured to the proximal phalanx.(continued)

PEARLS AND PITFALLS
Patient selection and control of the disease process are the most important factors.Joints with fixed deformities and cartilage loss are best treated with replacement arthroplasty. Proximal joint and distal joint correction must be performed before MCP joint surgery.Intrinsic transfers do not improve the long-term outcome of this procedure. Intrinsic lengthening is used only in patients with SLE.
POSTOPERATIVE CARE
The postoperative dressing is removed at about 10 to 14 days and the sutures are removed.2,4An orthoplast splint with the MCP joints extended and slightly overcorrected, usually in slight radial deviation, is applied until 4 weeks postoperatively. PIP joint motion is encouraged.At 4 weeks postoperatively, if Kirschner wires were inserted, they are removed. Splinting is then continued for 2 additional weeks.At 6 weeks postoperatively, hand therapy is started, concentrating on active MCP joint extension. Active MCP flexion is also started. Protective splinting is continued for another 2 weeks in between exercises and at night.To increase the postoperative flexion, the PIP joint is occasionally splinted in extension, concentrating the flexion force at the MCP joint.Dynamic splinting can be used to support extension and maintain digital alignment during the early healing stage but is usually not necessary.At 8 weeks postoperatively, daytime splinting is decreased and gradual return to functional activities is encouraged.Nighttime extension splinting is continued for 3 months.
OUTCOMES
MCP joint extension and ulnar drift are improved postoperatively.4 MCP flexion is usually slightly less than it was preoperatively.Strength is not significantly improved.Maintenance of correction is usually good with slight increase in ulnar drift, usually without recurrent subluxation.When the deformity is seen early and is still passively correctable with preserved joints, extensor tendon centralization and MCP joint synovectomy (as needed) is often beneficial, improving patient function.As with all joint procedures for deformities resulting from inflammatory arthritis, the procedure itself does not stop the progression of the disease. However, the new generation of disease-modifying medications combined with surgery may result in long-lasting correction of joint deformity.
COMPLICATIONS
InfectionWound healing problemsLoss of motionRecurrent ulnar drift with tendon subluxationRadial subluxation of the extensor tendon (seen in SLE)Progressive joint destruction from the arthritis and need for joint replacement
REFERENCES
- Abboud JA, Beredjiklian PK, Bozentka DJ. Metacarpophalangeal joint arthroplasty and rheumatoid arthritis. J Am Acad Orthop Surg 2003;11:184-191.
- Nalebuff EA. Surgery for systemic lupus erythematosus arthritis of the hand. Hand Clin 1996;12:591-602.
- Wilson RL, Carlblom ER. The rheumatoid metacarpohalangeal joint. Hand Clin 1989;5:223-237.
- Wood VE, Ichtertz DR, Yahiku H. Soft tissue metacarpophalangeal reconstruction for treatment of rheumatoid hand deformity. J Hand Surg Am 1989;14(2 pt 1):163-174.
