FRACTURES, DISLOCATIONS, AND FRACTURE-DISLOCATIONS OF THE ELBOW
FRACTURES OF THE RADIAL HEAD: EPIDEMIOLOGY AND BIOMECHANICS
Radial head fractures are the most common fractures of the adult elbow, accounting for approximately one-third of all elbow fractures. They can occur in isolation or as a critical component of more complex elbow instability patterns, such as the "terrible triad" of the elbow (radial head fracture, coronoid fracture, and elbow dislocation) or the Essex-Lopresti injury (radial head fracture, interosseous membrane disruption, and distal radioulnar joint [DRUJ] dislocation).
Understanding the biomechanics of the radiocapitellar joint is paramount for orthopedic surgeons. The radial head is not merely a spacer; it is a critical secondary stabilizer to valgus stress. When the medial collateral ligament (MCL) is intact, the radial head transmits approximately 60% of the axial load across the elbow joint. However, in the setting of an MCL deficiency, the radial head becomes the primary restraint to valgus instability. Furthermore, the radial head acts as a vital longitudinal stabilizer of the forearm. Resection of the radial head in the presence of unrecognized interosseous membrane or MCL injuries will lead to catastrophic proximal radial migration, ulnocarpal impaction, and chronic valgus instability.
Clinical Pearl: Never resect a radial head without definitively ruling out concomitant longitudinal forearm instability (Essex-Lopresti) or medial collateral ligament disruption. If the primary stabilizers are compromised, the radial head must be fixed or replaced to prevent profound, irreversible biomechanical collapse.
CLINICAL EVALUATION AND CLASSIFICATION
Patients typically present with lateral elbow pain, swelling, and a restricted range of motion, particularly in pronation and supination. A meticulous physical examination must include palpation of the MCL, the lateral collateral ligament (LCL) complex, the entire length of the interosseous membrane, and the DRUJ.
A critical step in the evaluation of isolated radial head fractures is determining the presence of a mechanical block. This is best assessed by aspirating the intra-articular hematoma through the lateral soft spot (the center of the triangle formed by the lateral epicondyle, radial head, and olecranon tip) and injecting 5 to 10 mL of local anesthetic (e.g., 1% lidocaine). Once analgesia is achieved, the elbow is taken through a full active and passive arc of flexion-extension and pronation-supination. A persistent block to motion dictates the need for operative intervention.
The Mason classification system, modified by Broberg and Morrey, remains the most widely utilized framework for describing these fractures and guiding treatment algorithms.
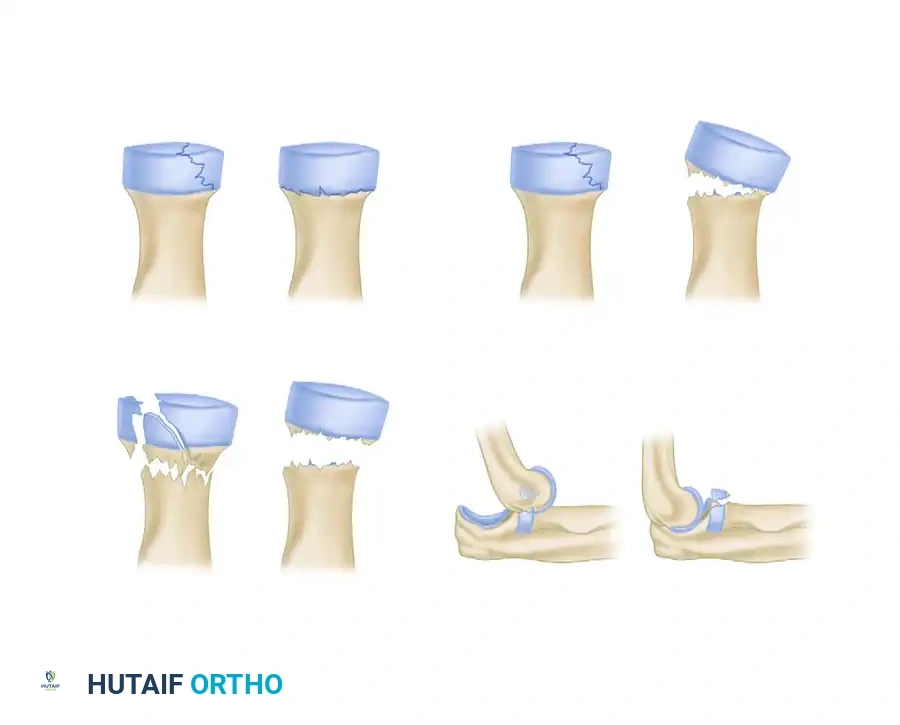
FIGURE 57-56: Mason classification of radial head and neck fractures.
- Mason Type I: Nondisplaced or minimally displaced fractures (less than 2 mm of displacement) with no mechanical block to rotation.
- Mason Type II: Displaced fractures (greater than 2 mm) involving more than 30% of the articular surface. These may or may not have a mechanical block.
- Mason Type III: Comminuted fractures involving the entire radial head, rendering it completely displaced and mechanically unviable.
- Mason Type IV: Any radial head fracture (Type I, II, or III) associated with an elbow dislocation.
NONOPERATIVE MANAGEMENT
When it is definitively confirmed that the fracture is an isolated injury, the overarching goal of treatment is to achieve a pain-free, stable arc of motion. Most radial head fractures are treated conservatively, specifically Mason Type I and select Mason Type II fractures without a mechanical block.
Nonunion and significant secondary fracture displacement are exceedingly rare in these types. However, post-traumatic stiffness is a frequent complication if immobilization is prolonged. If the patient demonstrates no block to their range of motion following hematoma aspiration, a brief period of immobilization in a sling (1 to 3 days) followed by immediate, progressive active range of motion predictably yields excellent results.
Long-term outcome studies strongly support this approach. Lindenhovius et al. reported that the results of operative treatment at a long-term (22-year) follow-up demonstrated no appreciable advantage over the reported long-term results of nonoperative treatment for isolated, stable injuries. Furthermore, in a cohort of 49 patients with Mason Type II fractures (2 to 5 mm of displacement), Akesson et al. reported that 80% were entirely pain-free and maintained ranges of motion similar to the noninjured extremity after primary nonoperative treatment. For the minority of patients who developed late symptomatic arthrosis or mechanical symptoms, delayed radial head resection provided significant improvement.
OPERATIVE TREATMENT: INDICATIONS AND PRINCIPLES
Operative intervention is strictly indicated for:
1. Displaced Mason Type II and III fractures that are part of a complex elbow dislocation pattern (Mason Type IV).
2. Fractures presenting with a definitive mechanical block to flexion-extension or pronation-supination.
3. Fractures associated with Essex-Lopresti injuries or severe MCL tears where the radial head is required for stability.
Critical to making the decision regarding operative treatment is determining that the injury is isolated versus part of a complex dislocation, and accurately assessing the viability of the fracture fragments for internal fixation.
Surgical Approaches to the Radial Head
Two primary surgical approaches are utilized for exposing the radial head: the Kocher approach and the Kaplan approach.
1. The Kocher Approach:
This is the most common approach, utilizing the internervous plane between the anconeus (supplied by the radial nerve) and the extensor carpi ulnaris (ECU, supplied by the posterior interosseous nerve [PIN]).
* Technique: An oblique incision is made from the lateral epicondyle extending distally toward the ulnar crest. The fascia is incised, and the interval between the anconeus and ECU is developed. The LCL complex originates from the lateral epicondyle and must be protected. The joint capsule is incised anterior to the equator of the radial head to avoid iatrogenic injury to the lateral ulnar collateral ligament (LUCL).
* Risk: The PIN is at risk if the dissection proceeds too far distally (beyond the annular ligament). Pronating the forearm moves the PIN further anteriorly and medially, protecting it during the exposure.
2. The Kaplan Approach:
This approach utilizes the interval between the extensor digitorum communis (EDC) and the extensor carpi radialis brevis (ECRB). Both muscles are innervated by the radial nerve, making this an intermuscular, rather than internervous, plane.
* Advantage: It provides more direct anterior access to the radial head and coronoid process.
* Risk: The PIN crosses the operative field more proximally in this approach compared to the Kocher approach, demanding meticulous dissection.
Surgical Warning: Regardless of the approach, always pronate the forearm during lateral elbow exposures. Pronation pulls the posterior interosseous nerve (PIN) anteriorly, maximizing the safe distance from the surgical field and reducing the risk of iatrogenic nerve palsy.
TREATMENT OF MASON TYPE II FRACTURES
Open Reduction and Internal Fixation (ORIF) is the gold standard for displaced Mason Type II fractures when surgery is indicated. The objective is anatomic restoration of the articular surface and rigid fixation to allow for early mobilization.
The Concept of the "Safe Zone"
A critical anatomical concept in radial head ORIF is the "safe zone." The radial head is not perfectly circular; it is elliptical. Furthermore, not all of its circumference articulates with the lesser sigmoid notch of the ulna during forearm rotation. The safe zone is a non-articulating arc of approximately 105 to 110 degrees located on the lateral aspect of the radial head when the forearm is in neutral rotation.
Hardware (screws or plates) must be placed strictly within this safe zone. If hardware protrudes outside this area, it will impinge on the proximal radioulnar joint (PRUJ) during pronation and supination, leading to severe mechanical blocks, pain, and rapid cartilage destruction.
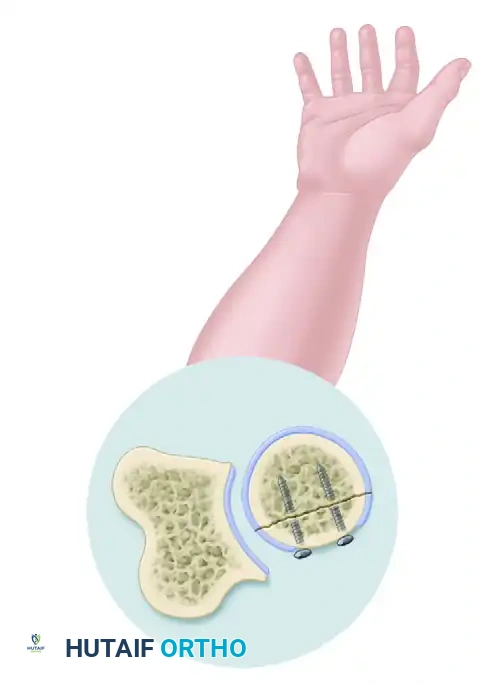
FIGURE 57-57A: "Safe zone" (area of radial head that does not articulate with ulna) for placement of fixation. View demonstrating the safe zone in a pronated position.
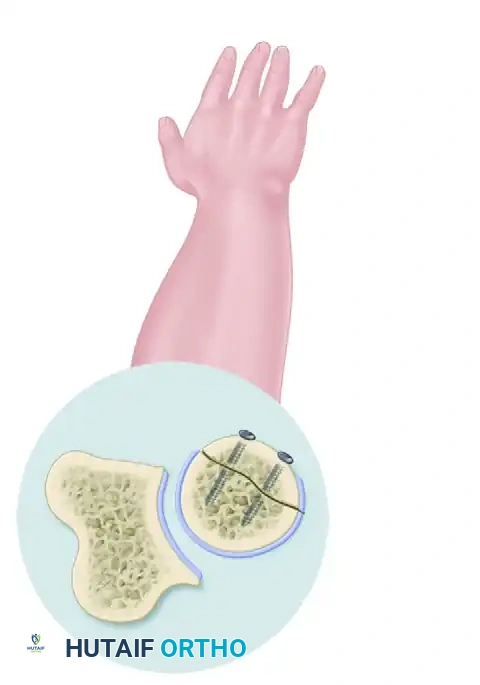
FIGURE 57-57B: View demonstrating the safe zone in a supinated position. Notice how the non-articulating portion remains accessible for hardware placement without impinging on the lesser sigmoid notch.
Intraoperatively, the safe zone can be identified by referencing the radial styloid and Lister's tubercle. The arc between these two landmarks on the distal radius corresponds to the safe zone on the proximal radius. Alternatively, it can be visualized directly by marking the anterior and posterior limits of the radial head that articulate with the ulna while taking the forearm through full pronation and supination.
Fixation Techniques
The use of mini-fragment screws (1.5 mm, 2.0 mm, or 2.4 mm headless compression screws), with or without a low-profile buttress plate placed in the safe zone, has demonstrated excellent clinical results. Headless screws are particularly advantageous as they can be buried beneath the articular cartilage, eliminating the risk of PRUJ impingement even if placed slightly outside the ideal safe zone.
If the fracture involves a small, non-articular fragment that cannot be securely fixed, partial resection of that specific fragment has been shown to provide satisfactory results, provided the remaining radial head maintains stability. However, if the remaining articular surface is insufficient to provide radiocapitellar stability, especially in the context of a complex fracture-dislocation, complete resection with radial head replacement becomes necessary.
TREATMENT OF MASON TYPE III AND IV FRACTURES
Mason Type III fractures are characterized by severe comminution. These fractures are frequently part of a more severe injury spectrum, often occurring with elbow dislocations, coronoid fractures, and ligamentous ruptures (Mason Type IV). Consequently, they are less frequently appropriate for ORIF than Type II fractures.
Radial Head Resection
Historically, complete excision of the comminuted radial head was a standard treatment. Radial head resection remains a viable option for isolated fractures in low-demand, elderly patients. However, it has been associated with highly variable and often poor results in younger, active patients.
Undiagnosed concomitant injuries play a massive role in the long-term failure of radial head resection. Long-term radiocapitellar arthrosis, chronic valgus elbow instability, and longitudinal forearm instability (proximal radial migration) have led modern orthopedic surgeons to largely abandon primary radial head resection in younger patients. While some small cohorts have reported satisfactory results at 16- to 21-year follow-ups, the risks generally outweigh the benefits.
Surgical Warning: Before any resection of the radial head is performed, elbow valgus instability and longitudinal forearm instability MUST be definitively ruled out. Intraoperative fluoroscopic stress testing is mandatory.
Open Reduction and Internal Fixation (ORIF)
ORIF can be performed with good results in highly selected patients with Type III fractures. Ikeda et al. reported greater grip strength and better functional scores in 15 patients treated with ORIF compared to 13 patients treated with radial head resection for Mason Type III fractures.
The ideal candidate for ORIF in a comminuted fracture follows the "Rule of Threes":
1. The fracture consists of three or fewer major articular fragments.
2. Each fragment is large enough to accept a mini-fragment screw for stable fixation.
3. There is minimal metaphyseal bone loss or impaction.
If these criteria cannot be met, attempting ORIF often leads to hardware failure, nonunion, or avascular necrosis of the fragments. In such cases, excision and prosthetic replacement should be immediately considered.
Radial Head Arthroplasty (Replacement)
Prosthetic replacement with metallic implants (modular monopolar or bipolar designs) has provided excellent results at short- to mid-term follow-up and is the treatment of choice for unsalvageable radial head fractures in the setting of elbow instability. The prosthesis acts as a crucial spacer, restoring the valgus buttress and longitudinal stability of the forearm while the ligaments heal.
Surgical Technique for Arthroplasty:
1. Excision: The comminuted fragments are carefully excised. The native radial head should be reconstructed on the back table to accurately gauge the size of the implant required.
2. Preparation: The radial neck is prepared with a broach. Care must be taken to preserve as much native radial neck as possible to maintain the insertion of the biceps tendon and the annular ligament.
3. Sizing: This is the most critical step. The implant must not "overstuff" the radiocapitellar joint. Overstuffing increases pressure on the capitellum, leading to rapid cartilage wear, severe stiffness, and chronic pain. The articular surface of the implant should sit perfectly flush with, or 1 to 2 mm proximal to, the lateral edge of the coronoid articular surface.
4. Implantation: A smooth-stemmed, loose-fitting implant is often preferred as it allows for micro-motion and self-alignment during forearm rotation, reducing stress at the stem-bone interface.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Regardless of whether the patient undergoes ORIF or Arthroplasty, the postoperative protocol is centered on early, controlled mobilization to prevent the most common complication: elbow stiffness.
- Phase I (Days 1-7): The elbow is immobilized in a posterior splint at 90 degrees of flexion for soft tissue rest. If the LCL was repaired, the forearm is placed in pronation to relax the lateral repair.
- Phase II (Weeks 1-6): The splint is removed, and a hinged elbow brace is applied. Active and active-assisted range of motion exercises for flexion and extension are initiated. Pronation and supination are performed with the elbow flexed to 90 degrees. Passive stretching is strictly avoided to prevent heterotopic ossification and hardware failure.
- Phase III (Weeks 6-12): Weaning from the brace begins. Strengthening exercises are gradually introduced once radiographic evidence of fracture healing (in ORIF) or clinical stability is confirmed.
COMPLICATIONS
The surgical management of radial head fractures is technically demanding, and complications can significantly impact patient outcomes.
* Stiffness: The most common complication. Loss of terminal extension (10 to 15 degrees) is frequent but rarely functionally limiting. Severe stiffness may require late arthroscopic or open capsular release.
* Posterior Interosseous Nerve (PIN) Palsy: Usually transient, resulting from aggressive retraction. Meticulous technique and forearm pronation during exposure mitigate this risk.
* Hardware Impingement: Occurs if ORIF hardware is placed outside the safe zone, requiring secondary surgery for hardware removal.
* Radiocapitellar Arthrosis: Can occur late due to initial cartilage trauma, malunion, or overstuffing of a radial head prosthesis.
* Heterotopic Ossification (HO): More common in complex fracture-dislocations. Prophylaxis with NSAIDs (e.g., Indomethacin) or single-dose radiation may be considered in high-risk patients.
📚 Medical References
- radial head fractures treated with a modular metallic radial head arthroplasty: study of outcomes, J Bone Joint Surg 88A:2192, 2006.
- Gschwend N, Loehr J, Ivosevic-Radovanovic D, et al: Semiconstrained elbow prostheses with special reference to the GSB III prosthesis, Clin Orthop Relat Res 232:104, 1988.
- Gschwend N, Scheier NH, Bähler AR: Long-term results of GSB III elbow arthroplasty, J Bone Joint Surg 81B:1005, 1999.
- Gschwend N, Simmen BR, Matejovsky Z: Late complications in elbow arthroplasty, J Shoulder Elbow Surg 5:86, 1996.
- Gutow AP, Wolfe SW: Infection following total elbow arthroplasty, Hand Clin 10:521, 1994.
- Hanyu T, Nakazono K, Ishimkawa H: Humeral shaft fracture after a total elbow arthroplasty, J Shoulder Elbow Surg 7:541, 1998.
- Harrington IJ, Sekyi-Otu A, Barrington TW, et al: The functional outcome with metallic radial head implants in the treatment of unstable elbow fractures: a long-term review, J Trauma 50:46, 2001.
- Harrington IJ, Tountas AA: Replacement of the radial head in the treatment of unstable elbow fractures, Injury 12:405, 1981.
- Hildebrand KA, Patterson SD, Regan WD, et al: Functional outcome of semiconstrained total elbow arthroplasty, J Bone Joint Surg 82A:1379, 2000.
- Ikavalko M, Belt EA, Kautiainen H, et al: Revisions for aseptic loosening in Souter-Strathclyde elbow arthroplasty: incidence of revisions of different components used in 522 consecutive cases, Acta Orthop Scand 73:257, 2002.
- Inglis AE: Revision surgery following a failed total elbow arthroplasty, Clin Orthop Relat Res 170:213, 1982.
- Inglis AE, Inglis AE Jr, Figgie MM, et al: Total elbow arthroplasty for fl ail and unstable elbows, J Shoulder Elbow Surg 6:29, 1997.
- Inglis AE, Pellici PM: Total elbow replacement, J Bone Joint Surg 62A:1252, 1980.
- Jensen CH, Jacobsen S, Ratchke M, et al: The GSB III elbow prosthesis in rheumatoid arthritis: a 2to 9-year follow-up, Acta Orthop 77:143, 2006.
- Jensen SL, Deutch SR, Olsen BS, et al: Laxity of the elbow after experimental excision of the radial head and division of the medial collateral ligament: effi cacy of ligament repair and radial head prosthetic replacement: a cadaver study, J Bone Joint Surg 85B:1006, 2003.
- Kamineni S, Morrey BF: Distal humeral fractures treated with noncustom total elbow replacement: surgical technique, J Bone Joint Surg 87A(suppl 1 pt 1):41, 2005.
- Kay RM, Eckardt JJ: Total elbow allograft for twice-failed total elbow arthroplasty, Clin Orthop Relat Res 303:135, 1994.
- Kelly EW, Coghlan J, Bell S: Fiveto thirteen-year follow-up of the GSB III total elbow arthroplasty, J Shoulder Elbow Surg 13:434, 2004.
- Khatri M, Stirrat AN: Souter-Strathclyde total elbow arthroplasty in rheumatoid arthritis: medium-term results, J Bone Joint Surg 87B:950, 2005.
- King GJW, Adams RA, Morrey BF: Total elbow arthroplasty: revision with use of a noncustom semiconstrained prosthesis, J Bone Joint Surg 79A:394, 1997.
- King GJW, Zarzour ZDS, Rath DA, et al: Metallic radial head arthroplasty improves valgus stability of the elbow, Clin Orthop Relat Res 368:114, 1999.
- Knight DJ, Rymaszewski LA, Amis AA, et al: Primary replacement of the fractured radial head with a metal prosthesis, J Bone Joint Surg 75B:572, 1993.
- Kozak TK, Adams RA, Morrey BF: Total elbow arthroplasty in primary osteoarthritis of the elbow, J Arthroplasty 13:837, 1998.
- Kraay MJ, Figgie MP, Inglis AE, et al: Primary semiconstrained total elbow arthroplasty, J Bone Joint Surg 76B:636, 1994.
- Kudo H: Nonconstrained elbow arthroplasty for mutilans deformity in rheumatoid arthritis, J Bone Joint Surg 80B:234, 1998.
- Kudo H, Iwano K: Total elbow arthroplasty with a non-constrained surface-replacement prosthesis in patients who have rheumatoid arthritis: a long-term follow-up study, J Bone Joint Surg 72A:355, 1990.
- Kudo H, Iwano K, Nishino J: Cementless or hybrid total elbow arthroplasty with titanium-alloy implants, J Arthroplasty 9:269, 1994.
- Kudo H, Iwano K, Nishino J: Total elbow arthroplasty with use of a nonconstrained humeral component inserted without cement in patients who have rheumatoid arthritis, J Bone Joint Surg 81A:1268, 1999.
- Kudo H, Iwano K, Watanabe S: Total replacement of the rheumatoid elbow with a hingeless prosthesis, J Bone Joint Surg 62A:277, 1980.
- Lee BP, Adams RA, Morrey BF: Polyethylene wear after total elbow arthroplasty, J Bone Joint Surg 87A:1080, 2005.
- Lee DH: Impaction allograft bone-grafting for revision total elbow arthroplasty, J Bone Joint Surg 81A:1008, 1999.
- Little CP, Graham AJ, Carr AJ: Total elbow arthroplasty: a systematic review of the literature in the English language until the end of 2003, J Bone Joint Surg 87B:437, 2005.
- Little CP, Graham AJ, Karatzas G, et al: Outcomes of total elbow arthroplasty for rheumatoid arthritis: comparative study of three implants, J Bone Joint Surg 87A:2439, 2005.
- Loebenberg MI, Adams R, O’Driscoll SW, et al: Impaction grafting in revision total elbow arthroplasty, J Bone Joint Surg 87A:99, 2005.
- London JT: Resurfacing total elbow arthroplasty, Orthop Trans 2:217, 1978.
- Lyall HA, Cohen B, Clatworthy M, et al: Results of the SouterStrathclyde total elbow arthroplasty in patients with rheumatoid arthritis, J Arthroplasty 9:279, 1994.
- MacAusland WR: Replacement of the lower end of the humerus with a prosthesis: a report of four cases, West J Surg Obstet Gynecol 62:557, 1954.
- Mackay I, FitzGerald B, Miller JH: Silastic radial head prosthesis in rheumatoid arthritis, Acta Orthop Scand 53:63, 1982.
- Malone AA, Taylor AJN, Fyfe IS: Successful outcome of the Souter-Strathclyde elbow arthroplasty, J Shoulder Elbow Surg 13:548, 2004.
- Marra G, Morrey BF, Gallay SH, et al: Fracture and nonunion of the olecranon in total elbow arthroplasty, J Shoulder Elbow Surg 15:486, 2006.
- Morrey BF, Adams RA: Semiconstrained arthroplasty for the treatment of rheumatoid arthritis of the elbow, J Bone Joint Surg 74A:479, 1992.
- Morrey BF, Askew RPT, Chao EY: Silastic prosthetic replacement for the radial head, J Bone Joint Surg 63A:454, 1981.
- Morrey BF, Bryan RS: Infection after total elbow arthroplasty, J Bone Joint Surg 65A:330, 1983.
- Morrey BF, Bryan RS, Dobyns JH, et al: Total elbow arthroplasty: a fi ve-year experience at the Mayo Clinic, J Bone Joint Surg 63A:1050, 1981.
- Morrey BF, Chao EY: Biomechanical study of the elbow following excision of the radial head, J Bone Joint Surg 61A:63, 1979.
- O’Driscoll SW, King GJ: Treatment of instability after total elbow arthroplasty, Orthop Clin North Am 32:679, 2001.
- Phillips NJ, Ali A, Stanley D: Treatment of primary degenerative arthritis of the elbow by ulnohumeral arthroplasty: a long-term follow-up, J Bone Joint Surg 85B:347, 2003.
- Pierce TD, Herndon JH: The triceps-preserving approach to total elbow arthroplasty, Clin Orthop Relat Res 354:144, 1998.
- Pöll RG, Rozing PM: Use of the Souter-Strathclyde total elbow prosthesis in patients who have rheumatoid arthritis, J Bone Joint Surg 73A:1227, 1991.
- Pritchard RW: Long-term follow-up study: semi-constrained elbow prosthesis, Orthopedics 4:151, 1981.
- Pritchard RW: Anatomic surface elbow arthroplasty: a preliminary report, Clin Orthop Relat Res 179:223, 1983.
- Pritchard RW: Total elbow joint arthroplasty in patients with rheumatoid arthritis, Semin Arthritis Rheum 21:24, 1991.
- Ramsey ML, Adams RA, Morrey BF: Instability of the elbow treated with semiconstrained total elbow arthroplasty, J Bone Joint Surg 81A:38, 1999.
- Ruth JT, Wilde AH: Capitellocondylar total elbow replacement, J Bone Joint Surg 74A:95, 1992.
- Sanchez-Sotelo J, O’Driscoll S, Morrey BF: Periprosthetic humeral fractures after total elbow arthroplasty: treatment with implant revision and strut allograft augmentation, J Bone Joint Surg 84A:1642, 2002.
- Schemitsch EH, Ewald FC, Thornhill TS: Results of total elbow arthroplasty after excision of the radial head and synovectomy in patients who had rheumatoid arthritis, J Bone Joint Surg 78A:1541, 1996.
- Schlein AP: Semiconstrained total elbow arthroplasty, Clin Orthop Relat Res 121:222, 1976.
- Souter WA: Arthroplasty of the elbow: with particular reference to metallic hinge arthroplasty in rheumatoid patients, Orthop Clin North Am 4:395, 1973.
- Sperling JW, Pritchard DJ, Morrey BF: Total elbow arthroplasty after resection of tumors at the elbow, Clin Orthop Relat Res 367:256, 1999.
- Street DM, Stevens PS: A humeral replacement prosthesis for the elbow: results in ten elbows, J Bone Joint Surg 56A:1147, 1974.
- Swanson AB, Jaeger SH, LaRochelle D: Comminuted fractures of the radial head: the role of silicone-implant replacement arthroplasty, J Bone Joint Surg 63A:1039, 1981.
- Swanson AB, Swanson G, Masada K, et al: Constrained total elbow arthroplasty, J Arthroplasty 6:203, 1991.
- Tanaka N, Kudo H, Iwano K, et al: Kudo total elbow arthroplasty in patients with rheumatoid arthritis: a long-term follow-up study, J Bone Joint Surg 83A:1506, 2001.
- Thillemann TM, Olsen BS, Johannsen HV, et al: Long-term results with the Kudo type 3 total elbow arthroplasty, J Shoulder Elbow Surg 15:485, 2006.
- Trail IA, Nuttal D, Stanley JK: Survivorship and radiological analysis of the standard Souter-Strathclyde total elbow arthroplasty, J Bone Joint Surg 81B:80, 1999.
- Trail IA, Nuttal D, Stanley JK: Comparison of survivorship between standard and long-stem Souter-Strathclyde total elbow arthroplasty, J Shoulder Elbow Surg 11:373, 2002.
- Trepman E, Ewald FC: Early failure of silicone radial head implants in the rheumatoid elbow, J Arthroplasty 6:59, 1991.
- Trepman E, Vella IM, Ewald FC: Radial head replacement in capitellocondylar total elbow arthroplasty, J Arthroplasty 6:67, 1991.
- van der Lugt JC, Geskus RB, Rozing PM: Primary SouterStrathclyde total elbow prosthesis in rheumatoid arthritis: surgical technique, J Bone Joint Surg 87A(suppl 1 pt 1):67, 2005.
- Van Glabbeek F, Van Riet RP, Baumfi eld JA, et al: Detrimental effects of overstuffi ng or understuffi ng with a radial head replacement in the medial collateral-ligament defi cient elbow, J Bone Joint Surg 86A:2629, 2004.
- Wadsworth TG: A new technique of total elbow replacement, Eng Med 10:69, 1980.
- Weiland AJ, Weiss APC, Wills RP, et al: Capitellocondylar total elbow replacement: a long-term follow-up study, J Bone Joint Surg 71A:217, 1989.
- Wolfe SW, Figgie MP, Inglis AE, et al: Management of infection about total elbow prostheses, J Bone Joint Surg 72A:198, 1990.
- Wretenberg PF, Mikhail WE: Late dislocation after total elbow arthroplasty, J Shoulder Elbow Surg 8:178, 1999.
- Yamaguchi K, Adams RA, Morrey BF: Infection after total elbow arthroplasty, J Bone Joint Surg 80A:481, 1998.
- Yamaguchi K, Adams RA, Morrey BF: Semiconstrained total elbow arthroplasty in the context of treated previous infection, J Shoulder Elbow Surg 8:461, 1999.
- Yanni ON, Fearn CB, Gallannaugh SC, Joshi R: The RoperTuke total elbow arthroplasty: 4to 10-year results of an unconstrained prosthesis, J Bone Joint Surg 82B:705, 2000.
- Resection Arthroplasty Albee FH: Arthroplasty of the elbow, J Bone Joint Surg 15:979, 1933.
- Baer WS: Preliminary report of animal membrane in producing mobility in ankylosed joint, Am J Orthop Surg 7:3, 1909.
- Baer WS: Arthroplasty with the aid of animal membrane, Am J Orthop Surg 16:1, 1918.
- Buzby BF: End results of excision of the elbow, Ann Surg 103:625, 1936.
- Campbell WC: Arthroplasties, J Orthop Surg 19:430, 1921.
- Campbell WC: Arthroplasty of the elbow, Ann Surg 76:615, 1922.
- Campbell WC: Mobilization of joints with bony ankylosis: an analysis of 110 cases, JAMA 93:976, 1924.
- Campbell WC: Operative orthopaedics, St Louis, 1939, Mosby. Cheng SL, Morrey BF: Treatment of the mobile, painful arthritic elbow by distraction interposition arthroplasty, J Bone Joint Surg 82B:233, 2000.
- Froimson AI, Silva JE, Richey D: Cutis arthroplasty of the elbow, J Bone Joint Surg 58A:863, 1976.
- Hass J: Functional arthroplasty, J Bone Joint Surg 26:297, 1944.
- Hausman MR, Birnbaum PS: Interposition elbow arthroplasty, Tech Hand Up Extrem Surg 8:181, 2004.
- Henderson MS: What are the real results of arthroplasty? Am J Orthop Surg 16:30, 1918.
- Henderson MS: Arthroplasty, Minn Med 8:97, 1925.
- Hurri L, Pulkki T, Vainio K: Arthroplasty of the elbow in rheumatoid arthritis, Acta Chir Scand 127:459, 1964.
- Ikävalko M, Belt EA, Kautiainen H, et al: Revisions for aseptic loosening in Souter-Strathclyde elbow arthroplasty: incidence of revisions of different components used in 522 consecutive cases, Acta Orthop Scand 73:257, 2002.
- Knight RA, Van Zandt IL: Arthroplasty of the elbow: an endresult study, J Bone Joint Surg 34A:610, 1952.
- Lee DH: Posttraumatic elbow arthritis and arthroplasty, Orthop Clin North Am 30:141, 1999.
- Lexer E: Über Gelenktransplantationen, Arch Klink Chir 90:263, 1909.
- Ljung P, Larsson K, Rydholm U: Interposition arthroplasty of the elbow with rheumatoid arthritis, J Shoulder Elbow Surg 5:81, 1996.
- MacAusland WR: The mobilization of elbow by free fascia transplantation with report of 31 cases, Surg Gynecol Obstet 33:223, 1921.
- MacAusland WR: Arthroplasty of the elbow, N Engl J Med 235:97, 1947.
- Morrey BF: Posttraumatic contracture of the elbow: operative treatment, including distraction arthroplasty, J Bone Joint Surg 72A: 601, 1990.
- Murphy JB: Ankylosis: arthroplasty, clinical and experimental, JAMA 44:1573, 1905.
- Murphy JB: Arthroplasty, Ann Surg 57:593, 1913.
- Oka Y: Debridement arthroplasty for osteoarthrosis of the elbow: 50 patients followed mean 5 years, Acta Orthop Scand 71:185, 2000.
- Oka Y, Ohta K, Saitoh I: Debridement arthroplasty for osteoarthritis of the elbow, Clin Orthop Relat Res 351:127, 1998.
- [Ollier L: Traité des résections et des opérations conservatrices qu’on peut pratiques sur le systéme osseux, Paris, 1885-1889, G Masson.
Payr E: Über die operative mobilizierung ankylosierter Gelenke, Munich, Med Wochenschr 37:1921, 1910.](https://pubmed.ncbi.nlm.nih.gov/?term=Ollier%20L%3A%20Trait%C3%A9%20des%20r%C3%A9sections%20et%20des%20op%C3%A9rations%20conservatrices%20qu%E2%80%99on%20peut%20pratiques%20sur%20le%20syst%C3%A9me%20osseux%2C%20Paris%2C%201885-1889%2C%20G%20Masson.%0A%0APayr%20E%3A%20%C3%9Cber%20die%20operative%20mobilizierung%20ankylosierter%20Gelenke%2C%20Munich%2C%20Med%20Wochenschr%2037%3A1921%2C%201910.)
- Putti V: Arthroplasty, J Orthop Surg 19:419, 1921.
- Silva JF: Old dislocations of the elbow, Ann R Coll Surg Engl 22:363, 1958.
- Speed JS, Smith H: Arthroplasty: a review of the past ten years, Int Abstr Surg Gynecol Obstet 70:224, 1940.
- Tsuge K, Mizuseki T: Debridement arthroplasty for advanced primary osteoarthritis of the elbow, J Bone Joint Surg 76B:641, 1994.
- Tsuge K, Murakami T, Yasunaga Y, et al: Arthroplasty of the elbow: twenty years’ experience of a new approach, J Bone Joint Surg 69B:116, 1987.
- Uuspaa V: Anatomical interposition arthroplasty with dermal graft: a study of 51 elbow arthroplasties on 48 rheumatoid patients, Z Rheumatol 46:132, 1987.
- Vainio K: Arthroplasty of the elbow and hand in rheumatoid arthritis: a study of 131 operations. In Chapchal G, ed: Synovectomy and arthroplasty in rheumatoid arthritis, Stuttgart, 1967, Georg Thieme Verlag. Verneuil A: De la creation d’une fausse articulation par section ou resection partielle de l’os maxillaire inferieur, comme moyen de remedier l’ankylose orale de fausse de la machoire inferieur, Arch Gen Med 15:284, 1860.
- Wada T, Isogai S, Ishii S, et al: Débridement arthroplasty for primary osteoarthritis of the elbow, J Bone Joint Surg 86A:233, 2004.
- Wada T, Isogai S, Ishii S, et al: Débridement arthroplasty for primary osteoarthritis of the elbow: surgical technique, J Bone Joint Surg 87A(suppl 1 part 1):95, 2005.
- Wright PE, Stewart MJ: Fascial arthroplasty of the elbow. In Morrey BF, ed: The elbow and its disorders, Philadelphia, 1985, Saunders.
