INTRODUCTION AND BIOMECHANICAL PRINCIPLES
The forearm functions as a complex, highly articulated diarthrodial joint. Pronation and supination rely entirely on the precise anatomical relationship between the radius and the ulna, tethered by the interosseous membrane and the proximal and distal radioulnar joints (DRUJ). Fractures of both the radius and ulna—commonly referred to as both-bone forearm fractures—disrupt this delicate biomechanical axis.
Because even minor angular or rotational deformities can severely restrict forearm rotation, both-bone forearm fractures in adults are universally considered an absolute indication for operative intervention. Open reduction and internal fixation (ORIF) utilizing AO principles of anatomical reduction, stable internal fixation, preservation of blood supply, and early active mobilization is the gold standard of care.
Clinical Pearl: The radius possesses a natural lateral and dorsal bow that is critical for normal pronosupination. Failure to restore the magnitude and apex of the radial bow during plating will result in a mechanical block to rotation, significantly compromising functional outcomes.
PREOPERATIVE PLANNING AND SEQUENCE OF FIXATION
Meticulous preoperative evaluation of orthogonal radiographs is mandatory. The surgeon must assess the fracture pattern (transverse, oblique, comminuted, or segmental), the degree of displacement, and the presence of any associated joint dislocations (e.g., Monteggia or Galeazzi fracture-dislocations).
The sequence of fixation is a critical strategic decision that dictates the flow of the operation:
* Radius First: If anatomical reduction of the radius is readily achievable, begin with radial fixation. Restoring the complex geometry of the radius often simplifies the subsequent reduction of the ulna. Furthermore, if both fractures are extensively comminuted, the radius should be addressed first to re-establish the critical radial bow.
* Ulna First: If the radius is highly comminuted but the ulnar fracture is relatively simple (e.g., a transverse or short oblique pattern), it is advantageous to reduce and stabilize the ulna first. A rigidly fixed ulna provides a stable anatomical pillar, restoring the length and axis of the forearm, which facilitates the subsequent bridge plating of the comminuted radius.
SURGICAL ANATOMY AND APPROACHES
To minimize the risk of radioulnar synostosis, the radius and ulna must be approached through separate incisions. The choice of approach depends on the level of the fracture.
The Volar Henry Approach to the Radius
For the vast majority of fractures involving the middle and distal thirds of the radial shaft, the volar Henry approach is preferred. It utilizes the internervous plane between the flexor carpi radialis (FCR, innervated by the median nerve) and the brachioradialis (BR, innervated by the radial nerve).

Superficial dissection involves incising the deep fascia in line with the skin incision. The radial artery must be identified and protected, usually retracting it medially with the FCR.
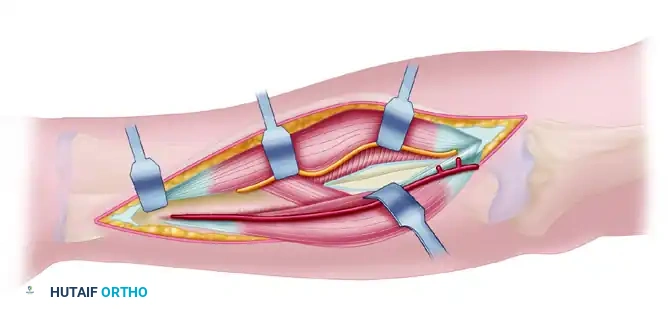
In the proximal extent of the wound, the radial recurrent artery and its venae comitantes must be ligated and divided to allow lateral retraction of the brachioradialis and the superficial branch of the radial nerve.

Deep dissection requires the elevation of the supinator muscle. To protect the posterior interosseous nerve (PIN) within the supinator, the muscle must be detached from its ulnar and volar insertions and reflected laterally.
The Dorsal Thompson Approach to the Proximal Radius
If a fracture requires fixation proximal to the biceps tuberosity, the dorsal Thompson approach is indicated. This approach exploits the internervous plane between the extensor carpi radialis brevis (ECRB, radial nerve) and the extensor digitorum communis (EDC, PIN). Extreme caution must be exercised to identify and protect the PIN as it emerges from the supinator muscle.
Approach to the Ulnar Shaft
The ulna is approached via its subcutaneous border, utilizing the internervous plane between the flexor carpi ulnaris (FCU, ulnar nerve) and the extensor carpi ulnaris (ECU, PIN).
The volar or distal aspect of the ulna is chosen for dissection based on which aspect has sustained more traumatic soft tissue stripping.
Surgical Warning: Avoid placing the plate directly on the subcutaneous crest of the ulna. Prominent hardware in this location frequently leads to soft tissue irritation, pain, and the eventual need for hardware removal. Position the plate on the volar or dorsal surface of the ulna whenever possible.
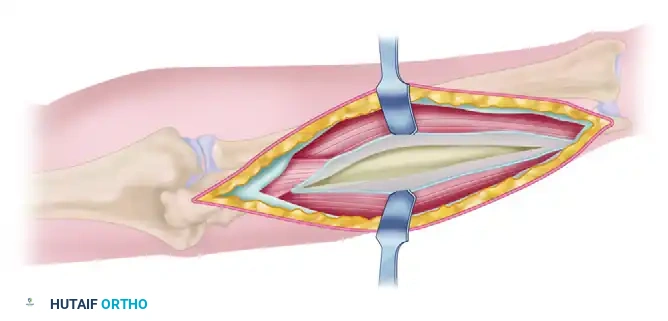
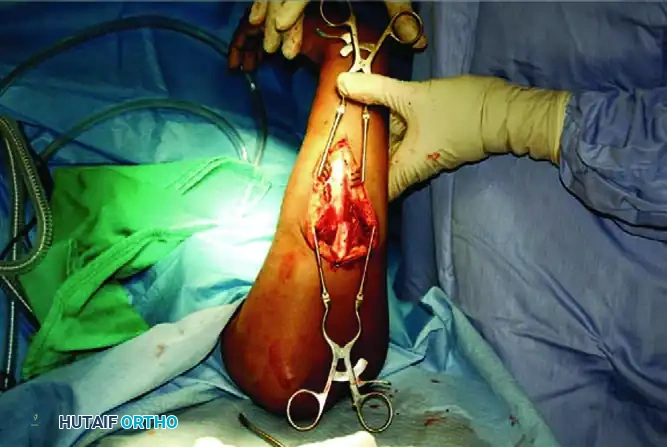
SURGICAL TECHNIQUE: STEP-BY-STEP ORIF
1. Exposure and Debridement
Following the chosen surgical approaches, expose the fracture sites. It is imperative to preserve the periosteum along the proximal and distal segments to maintain the osteogenic potential of the bone. Do not strip the periosteum beyond what is absolutely necessary for plate application. Débride the fracture edges, meticulously removing interposed hematoma, muscle, and devitalized debris to allow for intimate cortical contact.
2. Restoring Length
In cases where the fracture has been in a shortened position for an extended period, achieving length can be challenging. Options for attaining length include:
* Chemical paralysis (maximizing neuromuscular blockade).
* Mechanical distraction using a push-pull screw technique in the shaft combined with a lamina spreader.
* Careful, sequential soft tissue releases.
3. Fracture Reduction and Plate Application
The fixation strategy is dictated by the fracture morphology:
- Transverse Fractures: Achieve absolute stability using a 3.5-mm limited-contact dynamic compression plate (LC-DCP). Ensure axial compression is achieved across the fracture site.
- Fractures with a Butterfly Fragment: Anatomically reduce the butterfly fragment and stabilize it with 2.0-mm or 2.4-mm lag screws to convert the complex fracture into a simple one. Follow this with the application of a neutralization plate.
- Oblique Fractures: Reduce the fracture and achieve interfragmentary compression using a 2.0-mm, 2.4-mm, or 2.7-mm lag screw placed perpendicular to the fracture plane. Protect this lag screw with a 3.5-mm limited-contact neutralization plate.

- Extensively Comminuted Fractures: Attempting anatomical reduction of highly comminuted fragments devitalizes the bone and leads to nonunion. Instead, utilize a bridge plating technique. Use a plate of appropriate length to span the zone of comminution, securing it with at least three bicortical screws (six cortices) in the intact proximal and distal segments.
- Note: If the span of the plate on the radius is longer than 6 or 7 holes, adding a lateral contour to the plate is essential to match the native radial bow.

4. Ulnar Fixation and Final Assessment
After the radius is secured, proceed to the ulna using the same plating strategies (compression, neutralization, or bridge plating). Once both bones are rigidly stabilized, assess forearm pronation and supination clinically. The motion should be smooth and unimpeded.
Confirm adequate reduction, restoration of the radial bow, and proper hardware placement with orthogonal fluoroscopy. Ensure no screws are penetrating the radioulnar joints.

5. Closure
Irrigate the wounds copiously. Close the deep fascia only if it does not create compartment tension; otherwise, leave it open. Close the subcutaneous tissues and skin in a standard fashion.
GALEAZZI FRACTURE-DISLOCATIONS: "THE FRACTURE OF NECESSITY"
A Galeazzi fracture-dislocation is defined as a fracture of the distal or middle third of the radial shaft coupled with a dislocation or subluxation of the distal radioulnar joint (DRUJ). Historically termed the "fracture of necessity" by Campbell, this injury mandates operative intervention, as closed reduction and cast immobilization yield an unacceptably high rate of unsatisfactory results, including chronic DRUJ instability and severe functional impairment.
Pathoanatomy and Diagnosis
Similar to Monteggia lesions, Galeazzi fracture-dislocations frequently go unrecognized in the emergency department. Isolated fractures of the radial shaft are exceedingly rare; therefore, any displaced fracture of the distal third of the radius must raise a high index of suspicion for an associated DRUJ injury.
Galeazzi fracture-dislocations are classified based on the direction of the radial displacement, which dictates the deforming muscle forces and the direction of DRUJ instability.
Radiographic indicators of a DRUJ injury include:
1. Fracture at the base of the ulnar styloid.
2. Widening of the DRUJ space on a true anteroposterior (AP) radiograph.
3. Dorsal or volar dislocation of the ulna relative to the radius on a true lateral view of the wrist.
4. More than 5 mm of radial shortening relative to the ulna when compared with the contralateral, uninjured wrist.
Surgical Management of Galeazzi Injuries
Open reduction of the radial shaft fracture through an anterior Henry approach and rigid internal fixation with a 3.5-mm AO dynamic compression plate is the definitive treatment of choice in adults.
Clinical Pearl: Rigid, anatomical fixation of the radial shaft fracture is the most critical step in managing a Galeazzi injury. In the majority of cases, restoring the exact length and alignment of the radius will spontaneously reduce the DRUJ dislocation.
Assessing and Managing the DRUJ:
Once the radius is plated, the DRUJ must be evaluated for stability throughout the full arc of pronosupination.
* Stable DRUJ: If the DRUJ is stable after radial fixation, the forearm should be splinted in the position of greatest stability (traditionally supination) for 6 weeks. However, recent evidence suggests that immobilization in a neutral rotation for 2 weeks may be equally effective for stable joints.
* Unstable DRUJ: If the joint remains unstable despite anatomical radial fixation, it must be addressed. The forearm is placed in full supination (which tightens the volar radioulnar ligaments and reduces the joint), and the DRUJ is temporarily transfixed with two parallel Kirschner wires (K-wires). These wires should engage four cortices to provide adequate stability and allow for easy removal in the event of breakage.
* Alternative Soft Tissue Management: Alternatively, if there is a large, displaced ulnar styloid fragment, it can be fixed with a tension band or lag screw, which often restores the integrity of the triangular fibrocartilage complex (TFCC). Direct open repair of the TFCC soft tissues is another viable option.
* Irreducible DRUJ: An irreducible DRUJ after radial fixation is a surgical emergency indicating soft tissue interposition (commonly the ECU tendon or the median nerve). This requires an immediate open dorsal approach to the DRUJ to extract the interposed tissue and reduce the joint.
Prognostic Note: In a comprehensive 7-year follow-up study of 40 patients with DRUJ instability following radial shaft fracture fixation, Korompilias et al. demonstrated that persistent instability was significantly more frequent with fractures located closer to the joint (Type I fractures) compared to more proximal diaphyseal fractures (Type II or III). The location of the radial fracture is a reliable predictor of the likelihood of postoperative DRUJ instability.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative protocol must balance the need for soft tissue healing with the prevention of joint stiffness.
* Immobilization: Typically, for isolated both-bone forearm fractures with rigid fixation, only a bulky soft dressing is necessary. Splinting is reserved for cases where the elbow or wrist joint is involved, if the patient is non-compliant, or if the bone quality/fixation is questionable.
* Early Mobilization: Active and active-assisted range-of-motion (ROM) exercises for the fingers, wrist, and elbow are initiated 3 to 7 days after surgery. Early rotation prevents capsular contractures and promotes tendon gliding.
* Weight-Bearing Restrictions: Heavy lifting, pushing, and pulling are strictly prohibited until definitive radiographic evidence of fracture consolidation is observed, typically between 8 to 12 weeks postoperatively.
COMPLICATIONS AND PITFALLS
Despite meticulous technique, complications can arise:
1. Radioulnar Synostosis: Cross-union between the radius and ulna is a devastating complication that abolishes forearm rotation. Risk factors include operating through a single incision, severe crush injuries, and delayed surgery. Prevention relies on utilizing separate surgical approaches and minimizing periosteal stripping.
2. Nonunion: Often the result of inadequate fixation, failure to utilize bone grafts in severe bone loss, or excessive soft tissue stripping (devascularization). Treatment requires revision ORIF with autologous bone grafting.
3. Hardware Failure: Plate bending or screw pullout can occur if the patient is non-compliant with weight-bearing restrictions or if bridge plates are too short to withstand the lever-arm forces of the forearm.
4. Nerve Injury: The PIN is at highest risk during the dorsal Thompson approach and proximal Henry approach. The superficial radial nerve is at risk during the distal Henry approach. Meticulous dissection and gentle retraction are paramount.
