Introduction to Hip Arthroscopy
Arthroscopy of the hip has advanced significantly since its early popularization in the 1990s. Driven by a deeper understanding of femoroacetabular impingement (FAI) and labral pathology, the techniques and indications have become rigorously defined. Instrumentation has evolved from rigid, standard-length tools to specialized, flexible, and extra-length devices designed specifically for the hip's deep anatomical constraints.
Surgeons performing these procedures have advanced along a steep learning curve. Today, complex labral repairs and capsular plications are routinely performed, showing excellent long-term promise. Nonetheless, the hip joint remains inherently difficult to treat arthroscopically. The profound sphericity of the femoral head, the deep constraint of the acetabulum, the robust surrounding musculature, and the thick, unyielding capsule make accessibility to certain intra-articular areas highly challenging. Success demands a masterful understanding of traction biomechanics, three-dimensional anatomy, and meticulous portal placement.
Evidence-Based Indications
The indications for hip arthroscopy have expanded from simple diagnostics to comprehensive joint preservation. The most common clinical presentations warranting intervention include mechanical labral symptoms (buckling, locking, catching, falling episodes) and persistent inguinal pain that remains unresponsive to 4 to 6 weeks of targeted conservative treatment (activity modification, physical therapy, and intra-articular injections).
Labral Pathology and Chondral Defects
Reports by McCarthy et al. and O’Leary et al. have demonstrated 85% and 91% improvement, respectively, in hip pain and dysfunction following the arthroscopic débridement of labral defects. As techniques have evolved, labral repair and reconstruction have largely superseded simple débridement, yielding superior long-term survivorship of the joint. Good to excellent results have also been consistently reported following the arthroscopic débridement of loose bodies and focal chondral defects.
Pediatric Deformities and Avascular Necrosis
In the context of pediatric hip deformities, O’Leary et al. reported an 89% improvement in patients suffering from chronic hip pain secondary to previous Legg-Calvé-Perthes disease. For the evaluation of the joint surface in the early stages of osteonecrosis (avascular necrosis), arthroscopy serves as an invaluable adjunct. It allows for direct visualization of chondral integrity prior to more definitive procedures, such as free vascularized fibular grafting or core decompression.
Degenerative Joint Disease (Osteoarthritis)
Arthroscopic débridement for established osteoarthritis and late-stage osteonecrosis yields results similar to those seen in other arthritic joints. Generally, only about a 40% improvement of short-term duration is noted.
Surgical Warning: Arthroscopy in the setting of moderate-to-severe osteoarthritis (Tönnis Grade 2 or 3) should be viewed strictly as a stop-gap procedure. It is reserved for younger patients with mild-to-moderate degenerative joint disease who are attempting to delay total hip arthroplasty.
Trauma and Miscellaneous Indications
Arthroscopy is highly effective for the removal of intra-articular foreign bodies. Successful arthroscopic removal of bullet fragments, extraction of extruded intra-articular polymethylmethacrylate (PMMA) cement following previous surgeries, and the excision of a hypertrophic or impinging ligamentum teres have all been well documented.
Patient Positioning and Traction Biomechanics
Achieving safe and adequate joint distraction is the most critical prerequisite for successful hip arthroscopy. A minimum of 8 to 10 mm of distraction is recommended to avoid iatrogenic scuffing of the chondral surfaces or damage to the labrum during instrument insertion. Two primary patient positions are utilized: the Supine Position and the Lateral Decubitus Position.
The Supine Position (Byrd Technique)
The supine approach, popularized by J.W. Thomas Byrd, is the most widely utilized setup globally. It allows for excellent orientation and easy conversion to an open anterior approach if necessary.
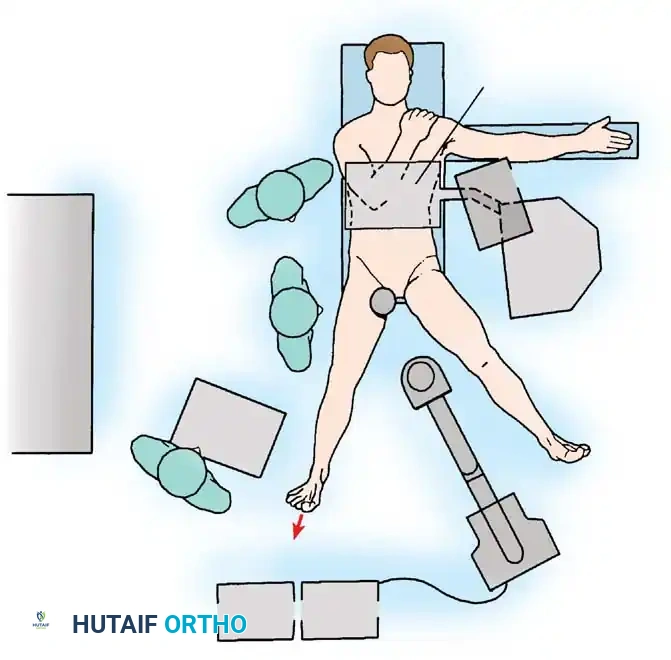
Surgical Technique 48-38: Supine Positioning
- Table Setup: Place the anesthetized patient supine on a specialized fracture table or a dedicated hip distraction system. Ensure complete skeletal muscle relaxation via paralytic agents to minimize the traction force required.
- Perineal Post Placement: Place a heavily padded perineal post, intentionally lateralizing it against the medial thigh of the operative leg.
Clinical Pearl: Lateralizing the perineal post is a critical safety maneuver. It adds a slight transverse component to the traction vector, pushing the femoral head laterally to help break the suction seal, and significantly lessens the likelihood of direct compression and subsequent neurapraxia of the pudendal nerve.
- Limb Positioning: Position the operative hip in extension, approximately 25 degrees of abduction, and neutral rotation.
- Flexion Avoidance: Slight flexion may relax the anterior capsule (iliofemoral ligament) and facilitate distraction, but it places increased traction on the sciatic nerve, drawing it closer to the joint and making it vulnerable to injury. Significant flexion must be avoided.
- Rotation: Neutral rotation is paramount during initial portal placement to protect the sciatic nerve posteriorly, although dynamic freedom of rotation during the procedure aids in exposing different regions of the femoral head and cam lesions.
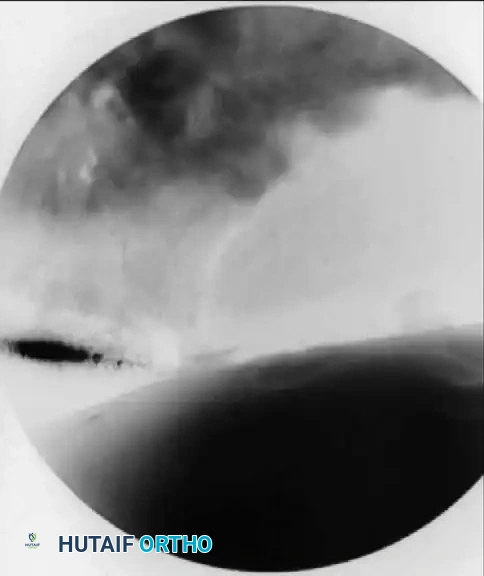
- Distraction: Apply traction to the operative extremity. Confirm adequate distraction of the joint space fluoroscopically before proceeding with portal placement.
The Lateral Decubitus Position (Glick Technique)
Glick et al. pioneered the lateral decubitus position, arguing that the supine anterior approach made viewing the posterior aspect of the hip difficult. This position utilizes gravity to assist in lateralizing the femoral head.

Surgical Technique 48-39: Lateral Decubitus Positioning
- Patient Orientation: Place the patient in the lateral decubitus position with the affected hip superior. Ensure the perineal post is meticulously padded to prevent pressure sores or pudendal nerve injury.
- Limb Positioning: Place the foot of the affected leg in the traction boot. Abduct the hip between 20 and 45 degrees, and maintain extension. As with the supine position, flexion is contraindicated due to sciatic nerve tension and the difficulty it creates for anterior instrument insertion.
- Traction Application: Attach a spring scale to the footpiece to measure the distraction weight. Glick noted that the average amount of traction necessary to distract the hip 8 mm is approximately 50 lbs. The perineal post can be pushed upward against the medial thigh to assist in lateral distraction.
- Preparation: Prepare and drape the hip widely to allow access as far anteriorly as the femoral artery and slightly past the posterior aspect of the greater trochanter.
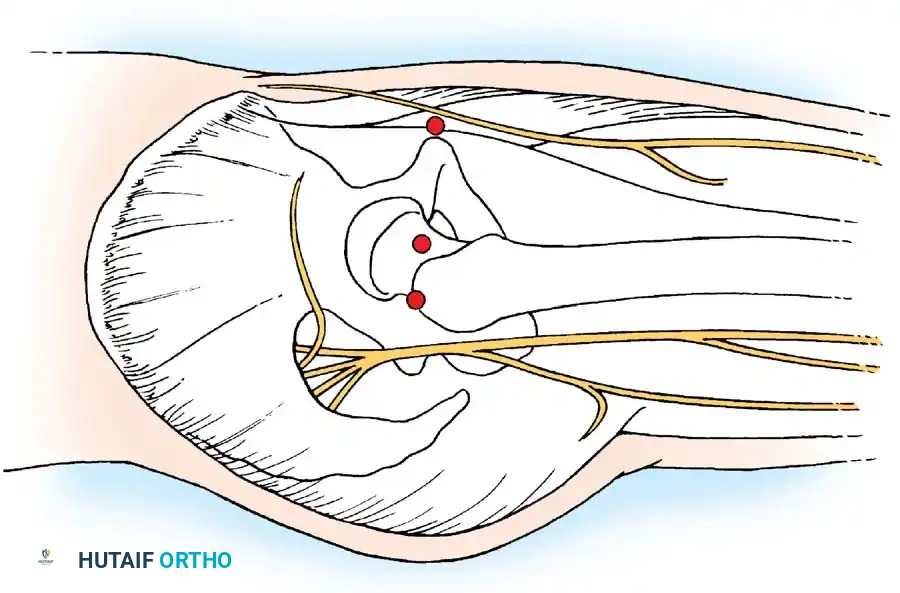
Arthroscopic Portal Anatomy and Safe Zones
Accurate portal placement is the cornerstone of safe hip arthroscopy. The hip is surrounded by major neurovascular structures, making adherence to anatomical landmarks non-negotiable.

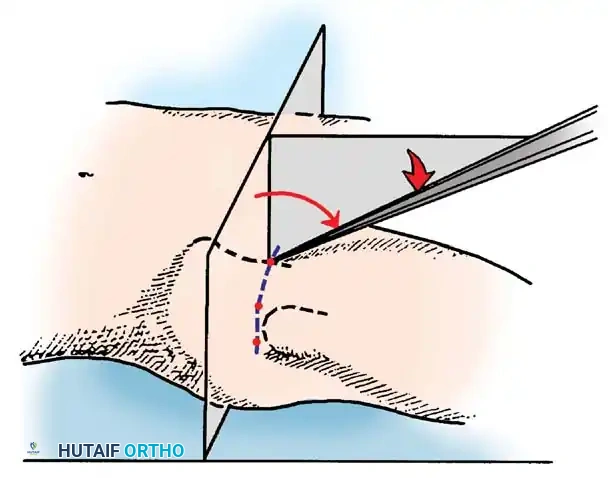
1. The Anterolateral Portal (The Viewing Portal)
This is typically the first portal established, as it lies within the primary "safe zone."
- Location: Positioned just superior and anterior to the tip of the greater trochanter.
- Trajectory: An 18-gauge spinal needle is advanced toward the femoral head along a line 45 degrees medial and 45 degrees proximal.
- Anatomy Traversed: Penetrates the gluteus medius muscle.
- Structures at Risk: The superior gluteal nerve traverses approximately 4.4 cm cephalad to this portal. Staying close to the trochanteric tip ensures safety.
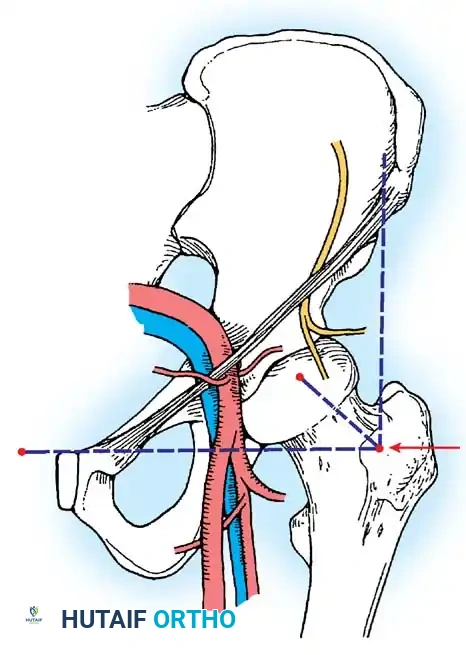
2. The Anterior Portal
Used primarily as a working portal for the anterior labrum and cam decompression.
- Location: Placed at the intersection of a vertical line drawn inferiorly from the anterior superior iliac spine (ASIS) and a transverse horizontal line drawn from the superior margin of the greater trochanter. Extended medially, this line sits just superior to the symphysis pubis.
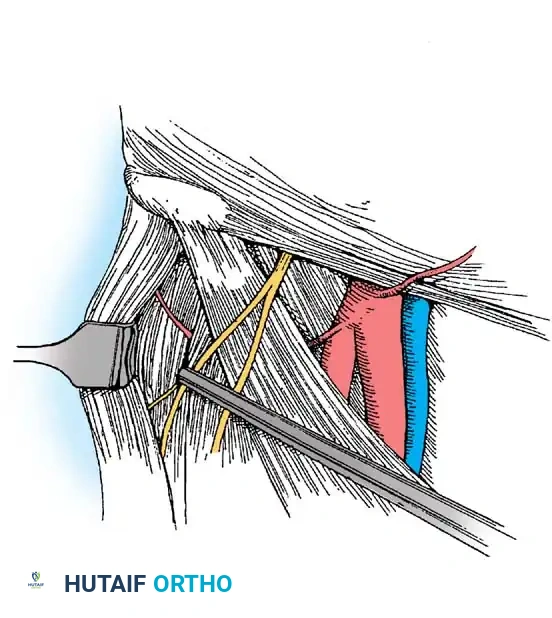
- Anatomy Traversed: Penetrates the sartorius and rectus femoris muscles before entering the anterior capsule.
- Structures at Risk: The Lateral Femoral Cutaneous Nerve (LFCN) and the ascending branch of the lateral femoral circumflex artery.
Surgical Warning: To avoid transecting the LFCN, use a superficial skin incision only. Bluntly dissect and spread the subcutaneous tissues with a hemostat down to the capsule before passing the cannula. The blunt trocar will safely push the nerve aside.
3. The Posterolateral Portal
Used for viewing the posterior labrum and removing posterior loose bodies.
- Location: Just superior to the margin of the greater trochanter at its posterior border.
- Trajectory: Directed slightly cephalad and anteriorly, converging toward the anterolateral portal.
- Anatomy Traversed: Traverses the gluteus medius and minimus muscles.
- Structures at Risk: The sciatic nerve. It is imperative to have the hip in neutral rotation while establishing this portal to maximize the distance between the portal tract and the sciatic nerve.
Step-by-Step Surgical Technique: Joint Access and Diagnostic Arthroscopy
- Initial Access: Establish the anterolateral portal first using a 6-inch, 17-gauge or 18-gauge spinal needle under continuous fluoroscopic guidance.
- Capsular Penetration: If excessive resistance is met during needle placement, redirect it under fluoroscopic control, aiming slightly more parallel to the femoral head and away from the cartilaginous edge of the acetabulum to prevent iatrogenic labral puncture.
- Venting the Joint: Distend the joint with 30 to 50 mL of sterile saline. A reverse flow of fluid signals successful entrance into the intra-articular space and breaks the vacuum seal, allowing the joint to distract fully.
- Cannula Insertion: Pass a flexible nitinol guidewire through the needle, withdraw the needle, and pass the cannulated obturator and sheath assembly over the wire. Never use excessive force, which could score the femoral head.
- Establishing Secondary Portals: Pass a spinal needle into the joint to create the anterior and posterolateral portals, directly observing the needle's entry with a 70-degree arthroscope from the anterolateral portal. Verify all placements with fluoroscopy.
- Fluid Management: Place the outflow in the posterolateral portal to maintain a clear visual field.
- Diagnostic Sweep: Alternate the 70-degree and 30-degree scopes between the anterolateral and anterior portals.
- 70-degree scope: Best for viewing the labrum, the peripheral gutter, and the periphery of the femoral head.
- 30-degree scope: Ideal for viewing the central weight-bearing portion of the acetabulum, the ligamentum teres, and the superior acetabular fossa.

- Capsulotomy: Pass an arthroscopic knife through the anterior cannula and perform a controlled interportal capsulotomy (incising the capsule transversely parallel to the labrum). This allows for significantly greater maneuverability of instruments.
Management of Labral Injuries (Technique 48-40)
Labral injuries most commonly result from traumatic hyperextension and external rotation of the hip, or repetitive microtrauma secondary to FAI. Lesions most frequently involve the anterior and anterosuperior margins of the labrum.
Tears are broadly divided into:
* Type I: Peripheral capsulolabral detachment (often amenable to repair).
* Type II: Intrasubstance tears or complex maceration (often requiring débridement or reconstruction).
Because the blood supply to the labrum is located peripherally (similar to the meniscus of the knee), peripheral detachments have excellent healing potential when anatomically repaired.

Labral Repair Technique
- Positioning for Repair: Place the patient in the modified supine position: 10 degrees of flexion, 15 degrees of internal rotation, 10 degrees of lateral tilt, and neutral abduction.
- Distraction Protocol: Using an extra-wide perineal post, place the leg first in abduction and apply traction to break the vacuum seal. Then, adduct the leg over the post to force the femoral head laterally. Apply straight, in-line traction until 8 to 10 mm of joint space is achieved (typically requiring 25 to 50 lbs of force). Apply gentle countertraction to the contralateral limb.
- Accessory Portals: Three portals are typically required for complex arthroscopic labral repair: the anterolateral, the anterior, and a Distal Lateral Accessory (DLA) portal. The DLA portal provides the optimal trajectory for drilling suture anchors into the acetabular rim without penetrating the articular cartilage.
- Bed Preparation: Use interchangeable, flexible cannulas and curved shaver blades to lightly decorticate the acetabular rim, exposing a bleeding bone bed to stimulate a healing response.
- Anchor Placement: Drill and place knotless or knotted suture anchors along the acetabular rim. Pass the sutures around or through the labral tissue using specialized suture-passing devices, and tie them down to restore the anatomical suction seal of the hip joint.
- Loose Body Removal: If loose bodies are present, use extra-length graspers to remove larger fragments piecemeal, carefully observing their retraction through the cannulas to prevent losing fragments in the soft tissues.
Postoperative Protocol
Postoperative rehabilitation is critical to the success of hip arthroscopy.
* Weight-Bearing: Following isolated débridement, patients may bear weight as tolerated. Following labral repair or microfracture, patients are typically restricted to 20 lbs flat-foot weight-bearing for 3 to 6 weeks to protect the repair.
* Bracing: A hip orthosis may be used to limit flexion to 90 degrees and prevent external rotation and extension, which place stress on the anterior capsule and labral repair.
* Physical Therapy: Early passive range of motion (often utilizing a CPM machine) is initiated immediately to prevent capsular adhesions. Active therapy progresses through isometric strengthening, core stabilization, and eventually sport-specific training by 3 to 4 months postoperatively.
📚 Medical References
- Hip arthroscopy by the lateral approach, Arthroscopy 3:4, 1987.
- Glueck CJ, Brandt G, Gruppo R, et al: Resistance to activated protein C and Legg-Perthes disease, Clin Orthop Relat Res 338:139, 1997.
- Glueck CJ, Crawford A, Roy D, et al: Association of antithrombotic factor defi ciencies and hypofi brinolysis with Legg-Perthes disease, J Bone Joint Surg 78A:3, 1996.
- Grezegorzewski A, Bowen R, Guille JT, et al: Treatment of the collapsed femoral head by containment in Legg-Calvé-Perthes disease, J Pediatr Orthop 23:15, 2003.
- Gu Y, Da Paz Junior AC: Can an enlarged acetabulum cover the femoral head well in Legg-Calvé-Perthes disease? J Pediatr Orthop 8B:173, 1999.
- Guille JT, Lipton GE, Szoke G, et al: Legg-Calvé-Perthes disease in girls: a comparison of the results with those seen in boys, J Bone Joint Surg 80A:1256, 1998.
- Guille JT, Lipton GE, Tsirikos AI, et al: Bilateral Legg-CalvéPerthes disease: presentation and outcome, J Pediatr Orthop 22:458, 2002.
- Guilleminet M, Barbier JM: Osteochondritis dissecans of the hip, J Bone Joint Surg 22:327, 1940.
- Hallel T, Salvati E: Osteochondritis dissecans following Legg-Calvé-Perthes disease, J Bone Joint Surg 58A:708, 1976.
- Harrison MH, Bassett CA: Three results of a double-blind trial of pulsed electromagnetic frequency in the treatment of Perthes’ disease, J Pediatr Orthop 17:264, 1997.
- Harry JD, Gross RH: A quantitative method for evaluating results of treating Legg-Perthes syndrome, J Pediatr Orthop 7:671, 1987.
- Hayek S, Kenet G, Lubetsky A, et al: Does thrombophilia play an aetiological role in Legg-Calvé-Perthes disease? J Bone Joint Surg 81B:686, 1999.
- Henderson RC, Renner JB, Sturdivant MC, et al: Evaluation of magnetic resonance imaging in Legg-Perthes disease: a prospective, blinded study, J Pediatr Orthop 10:289, 1990.
- Herceg MB, Cutright MT, Weiner DS: Remodeling of the proximal femur after upper femoral varus osteotomy for the treatment of Legg-Calvé-Perthes disease, J Pediatr Orthop 24:654, 2004.
- Herring JA: Management of Perthes’ disease, J Pediatr Orthop 16:1, 1996.
- Herring JA, Hotchkiss BL: Instructional case: Legg-Perthes disease versus multiple epiphyseal dysplasia, J Pediatr Orthop 7:341, 1987.
- Herring JA, Kim HT, Browne R: Legg-Calvé-Perthes disease: Part I. Classifi cation of radiographs with use of the modifi ed lateral pillar and Stulberg classifi cations, J Bone Joint Surg 86A:2103, 2004.
- Herring JA, Kim HT, Browne R: Legg-Calvé-Perthes disease: Part II. Prospective multicenter study of the effect of treatment on outcome, J Bone Joint Surg 86A:2121, 2004.
- Herring JA, Neustadt JB, Williams JJ, et al: The lateral pillar classifi cation of Legg-Calvé-Perthes disease, J Pediatr Orthop 12:143, 1992.
- Herring JA, Williams JJ, Neustadt JN, et al: Evolution of femoral head deformity during the healing phase of Legg-CalvéPerthes disease, J Pediatr Orthop 13:41, 1993.
- Hoikka V, Poussa M, Yrjönen T, et al: Intertrochanteric varus osteotomy for Perthes’ disease: radiographic changes after 2to 16-year follow-up of 126 hips, Acta Orthop Scand 62:549, 1991.
- Hosokawa M, Kim WC, Kubo T, et al: Preliminary report on usefulness of magnetic resonance imaging for outcome prediction in early-stage Legg-Calvé-Perthes disease, J Pediatr Orthop 8B:161, 1999.
- Hresko MT, McDougall PA, Gorlin JB, et al: Prospective reevaluation of the association between thrombotic diathesis and Legg-Calvé-Perthes disease, J Bone Joint Surg 84A:1613, 2002.
- Ippolito E, Tudisco C, Farsetti P: The long-term prognosis of unilateral Perthes’ disease, J Bone Joint Surg 69B:243, 1987.
- Ishida A, Kuwajima SS, Filho FL, et al: Salter innominate osteotomy in the treatment of severe Legg-Calvé-Perthes disease, J Pediatr Orthop 24:257, 2004.
- Ismail AM, Macnicol MF: Prognosis in Perthes’ disease: a comparison of radiological predictors, J Bone Joint Surg 80B:310, 1998.
- Jacobs R, Moens P, Fabry G: Lateral shelf acetabuloplasty in the early stage of Legg-Calvé-Perthes disease with special emphasis on the remaining growth of the acetabulum: a preliminary report, J Pediatr Orthop 13B:21, 2004.
- Joseph B: The fl exion-adduction test: an early sign of hip disease, J Pediatr Orthop 10B:180, 2001.
- Joseph B, Mulpuri K, Varghese G: Perthes’ disease in the adolescent, J Bone Joint Surg 83B:715, 2001.
- Joseph B, Nair S, Rao N, et al: Optimal timing for containment surgery for Perthes disease, J Pediatr Orthop 23:601, 2003.
- Joseph B, Srinivas G, Thomas R: Management of Perthes disease of late onset in southern India: the evaluation of a surgical method, J Bone Joint Surg 78B:625, 1996.
- Kahle WK, Coleman SS: The value of the acetabular teardrop fi gure in assessing pediatric hip disorders, J Pediatr Orthop 12:586, 1992.
- Kamegaya M, Shinada Y, Moriya H, et al: Acetabular remodeling in Perthes’ disease after primary healing, J Pediatr Orthop 12:308, 1992.
- Kamhi E, MacEwen GD: Osteochondritis dissecans in LeggCalvé-Perthes disease, J Bone Joint Surg 57A:506, 1975.
- Kealey WD, Mayne EE, McDonald W, et al: The role of coagulation abnormalities in the development of Perthes’ disease, J Bone Joint Surg 82B:744, 2000.
- Keenan WN, Clegg J: Perthes’ disease after “irritable hip:” delayed bone age shows the hip is a “marked man,” J Pediatr Orthop 16:20, 1996.
- Kelly FB Jr, Canale ST, Jones RR: Legg-Calvé-Perthes disease: long-term evaluation of non-containment treatment, J Bone Joint Surg 62A:400, 1980.
- Kiepurska A: Late results of treatment of Perthes’ disease by a functional method, Clin Orthop Relat Res 272:76, 1991.
- Kim HT, Wenger DR: “Functional retroversion” of the femoral head in Legg-Calvé-Perthes disease and epiphyseal dysplasia: analysis of head-neck deformity and its effect on limb position using three-dimensional computed tomography, J Pediatr Orthop 17:240, 1997.
- Kim HT, Wenger DR: Surgical correction of “functional retroversion” and “functional coxa vara” in late Legg-Calvé-Perthes disease and epiphyseal dysplasia: correction of deformity defi ned by new imaging modalities, J Pediatr Orthop 17:247, 1997.
- Kitakoji T, Hattori T, Iwata H: Femoral varus osteotomy in Legg-Calvé-Perthes disease: points at operation to prevent residual problems, J Pediatr Orthop 19:76, 1999.
- Kocaoglu M, Kilicoglu OI, Goksan SB, et al: Ilizarov fi xator for treatment of Legg-Calvé-Perthes disease, J Pediatr Orthop 8B:276, 1999.
- Koczewski P, Napiontek M: Perthes’ disease or late avascular necrosis after developmental dislocation of the hip? Acta Orthop Scand 72:331, 2001.
- Kruse RW, Guille JT, Bowen JR: Shelf arthroplasty in patients who have had Legg-Perthes disease, J Bone Joint Surg 64A:1338, 1991.
- Kumar D, Bache CE, O’Hara JN: Interlocking triple pelvic osteotomy in severe Legg-Calvé-Perthes disease, J Pediatr Orthop 22:464, 2002.
- Kuwajima SS, Crawford AH, Ishida A, et al: Comparison between Salter’s innominate osteotomy and augmented acetabuloplasty in the treatment of patients with severe Legg-Calvé-Perthes disease: analysis of 90 hips with special reference to roentgenographic sphericity and coverage of the femoral head, J Pediatr Orthop 11:17, 2002.
- Lack W, Feldner-Busztin H, Ritschl P, et al: The results of surgical treatment for Perthes’ disease, J Pediatr Orthop 9:197, 1989.
- Lamer S, Dorgeret S, Khairouni A, et al: Femoral head vascularisation in Legg-Calvé-Perthes disease: comparison of dynamic gadolinium-enhanced subtraction MRI with bone scintigraphy, Pediatr Radiol 32:580, 2002.
- Landin LA, Danielsson LG, Wattsgard C: Transient synovitis of the hip: its incidence, epidemiology and relation to Perthes’ disease, J Bone Joint Surg 69B:238, 1987.
- Lecuire F: The long-term outcome of primary osteochondritis of the hip (Legg-Calvé-Perthes disease, J Bone Joint Surg 84B:636, 2002.
- Lee DY, Seong SC, Choi IH, et al: Changes of blood fl ow of the femoral head after subtrochanteric osteotomy in LeggPerthes’ disease: a serial scintigraphic study, J Pediatr Orthop 12:731, 1992.
- Leitch JM, Paterson DC, Foster BK: Growth disturbance in Legg-Calvé-Perthes disease and the consequences of surgical treatment, Clin Orthop Relat Res 262:178, 1991.
- Lindholm TS, Osterman K: Internal fi xation of the fragments of osteochondritis dissecans in the hip using bone transplants, J Bone Joint Surg 62B:43, 1980.
- Lloyd-Roberts GC, Catterall A, Salamon PB: A controlled study of the indications for and the results of femoral osteotomy in Perthes disease, J Bone Joint Surg 58B:31, 1976.
- Loder RT, Farley FA, Hensinger RN: Physeal slope in Perthes disease, J Bone Joint Surg 77B:736, 1995.
- Macnicol MF, Makris D: Distal transfer of the greater trochanter, J Bone Joint Surg 73B:838, 1991.
- Madan S, Fernandes J, Taylor JF: Radiological remodeling of the acetabulum in Perthes’ disease, Acta Orthop Belg 69:412, 2003.
- Mahnken AH, Staatz G, Ihme N, et al: MR signal intensity characteristics in Legg-Calvé-Perthes disease, Acta Radiol 43:329, 2002.
- Martinez AG, Weinstein SL: Recurrent Legg-Calvé-Perthes disease: case report and review of the literature, J Bone Joint Surg 73A:1081, 1991.
- Martinez AG, Weinstein SL, Dietz FR: The weight-bearing abduction brace for the treatment of Legg-Perthes’ disease, J Bone Joint Surg 74A:12, 1992.
- Matan AJ, Stevens PM, Smith JT, et al: Combination trochanteric arrest and intertrochanteric osteotomy for Perthes’ disease, J Pediatr Orthop 16:10, 1996.
- Maxted MJ, Jackson RK: Innominate osteotomy in Perthes’ disease: a radiological survey of results, J Bone Joint Surg 67B:399, 1985.
- Maxwell SL, Lappin KJ, Kealey WD, et al: Arthrodiastasis in Perthes’ disease, J Bone Joint Surg 86B:244, 2004.
- Mazda K, Pennecot GF, Zeller R, et al: Perthes’ disease after the age of twelve years: role of the remaining growth, J Bone Joint Surg 81B:696, 1999.
- McElwain JP, Regan BF, Dowling F, et al: Derotation varus osteotomy in Perthes disease, J Pediatr Orthop 5:195, 1985.
- Meeham PL, Angel D, Nelson JM: The Scottish Rite abduction orthosis for the treatment of Legg-Perthes disease: a radiographic analysis, J Bone Joint Surg 74A:2, 1992.
- Meiss L: Prognosis in Perthes’ disease, J Bone Joint Surg 81B:180, 1999.
- Moberg A, Hansson G, Kaniklides C: Results after femoral and innominate osteotomy in Legg-Calvé-Perthes disease, Clin Orthop Relat Res 334:257, 1997.
- Mose K: Legg-Calvé-Perthes disease, Copenhagen, 1964, Universitetsforlaget i Aarhus. Mukherjee A, Fabry G: Evaluation of the prognostic indices in Legg-Calvé-Perthes disease: statistical analysis of 116 hips, J Pediatr Orthop 10:153, 1990.
- Neyt JG, Weinstein SL, Spratt KF, et al: Stulberg classifi cation system for evaluation of Legg-Calvé-Perthes disease: intrarater and interrater reliability, J Bone Joint Surg 81A:1209, 1999.
- Noonan KJ, Price CT, Kupiszewski SJ, et al: Results of femoral varus osteotomy in children older than 9 years of age with Perthes disease, J Pediatr Orthop 21:198, 2001.
- Paterson DC, Leitch JM, Foster BK: Results of innominate osteotomy in the treatment of Legg-Calvé-Perthes disease, Clin Orthop Relat Res 266:96, 1991.
- [Pécasse GABM, Ekjer H, Haverkamp D, et al: Intertrochanteric osteotomy in young adults for sequelae of Legg-Calvé-
Perthes disease—a long term follow-up, Int Orthop 28:44, 2004.](https://pubmed.ncbi.nlm.nih.gov/?term=P%C3%A9casse%20GABM%2C%20Ekjer%20H%2C%20Haverkamp%20D%2C%20et%20al%3A%20Intertrochanteric%20osteotomy%20in%20young%20adults%20for%20sequelae%20of%20Legg-Calv%C3%A9-%0A%0APerthes%20disease%E2%80%94a%20long%20term%20follow-up%2C%20Int%20Orthop%2028%3A44%2C%202004.)
- Petrie JG, Bitenc I: The abduction weight-bearing treatment in Legg-Calvé-Perthes disease, J Bone Joint Surg 49A:1483, 1967 (abstract). Pinto MR, Peterson HA, Berquist TH: Magnetic resonance imaging in early diagnosis of Legg-Calvé-Perthes disease, J Pediatr Orthop 9:19, 1989.
- Price CT, Day DD, Flynn JC: Behavioral sequelae of bracing versus surgery for Legg-Calvé-Perthes disease, J Pediatr Orthop 8:285, 1988.
- Quain S, Catterall A: Hinge abduction of the hip: diagnosis and treatment, J Bone Joint Surg 68B:61, 1986.
- Raney EM, Grogan DP, Hurley ME, et al: The role of proximal femoral valgus osteotomy in Legg-Calvé-Perthes disease, Orthopedics 25:513, 2002.
- Reinker KA: Early diagnosis and treatment of hinge abduction in Legg-Perthes disease, J Pediatr Orthop 16:3, 1996.
- Richards BS, Coleman S: Subluxation of the femoral head in coxa plana, J Bone Joint Surg 69A:1312, 1987.
- Ritterbusch JF, Shantharam SS, Gelinas C: Comparison of lateral pillar classifi cation and Catterall classifi cation of Legg-CalvéPerthes disease, J Pediatr Orthop 13:200, 1993.
- Robben SG, Lequin MH, Diepstraten AF, et al: Doppler sonography of the anterior ascending cervical arteries of hip: evaluation of healthy and painful hips in children, AJR Am J Roentgenol 174:1629, 2000.
- Roberts JM, Yngve DA: Acetabular hypertrophy in Legg-CalvéPerthes disease, J Pediatr Orthop 5:416, 1985.
- Robinson HJ, Putter H, Sigmond MB, et al: Innominate osteotomy in Perthes disease, J Pediatr Orthop 8:426, 1988.
- Rowe SM, Chung JY, Moon ES, et al: Dysplasia epiphysealis capitis femoris—Meyer dysplasia, J Pediatr Orthop 25:18, 2005.
- Rowe SM, Chung JY, Moon ES, et al: Computed tomographic fi ndings of osteochondritis dissecans following Legg-CalvéPerthes disease, J Pediatr Orthop 23:356, 2003.
- Rowe SM, Kim HS, Yoon TR: Osteochondritis dissecans in Perthes’ disease: report of 7 cases, Acta Orthop Scand 60:545, 1989.
- Rowe SM, Moon ES, Song EK, et al: The correlation between coxa magna and fi nal outcome in Legg-Calvé-Perthes disease, J Pediatr Orthop 25:22, 2005.
- Rowe SM, Moon ES, Yoon TR, et al: Fate of the osteochondral fragments in osteochondritis dissecans after Legg-CalvéPerthes’ disease, J Bone Joint Surg 84B:1025, 2002.
- Salter RB: Experimental and clinical aspects of Perthes’ disease, J Bone Joint Surg 48B:393, 1966 (abstract). Salter RB, Thompson GH: Legg-Calvé-Perthes disease: the prognostic signifi cance of the subchondral fracture and a twogroup classifi cation of the femoral head involvement, J Bone Joint Surg 66A:479, 1984.
- Schmid OA, Hemmer S, Wünsche P, et al: The adult hip after femoral varus osteotomy in patients with unilateral LeggCalvé-Perthes disease, J Pediatr Orthop 12B:33, 2003.
- Segev E, Ezra E, Weintroub S, et al: Treatment of severe late onset Perthes’ disease with soft tissue release and articulated
