Management of Simple Elbow Dislocation
DEFINITION
Simple elbow dislocation is a dislocation of the ulnohumeral joint without concomitant fracture. Complex instability denotes the presence of a fracture associated with dislocation.The elbow is the second most commonly dislocated large joint.
PATHOANATOMY
Elbow stability is conferred by highly constrained osseous anatomy and the ligamentous anatomy. Essentially, there are three primary stabilizers of the elbow. 9,12The osseous architecture of the ulnohumeral joint, including the coronoid process and greater sigmoid notch of the ulna, and the trochlea of the humerusThe anterior band of the medial collateral ligament (aMCL) resists valgus stress. The aMCL originates on the anterior inferior face of the medial epicondyle and inserts on the sublime tubercle of the ulna.The lateral ulnar collateral ligament (LUCL) resists varus stress. The LUCL originates from an isometric point on the lateral supracondylar column and traverses across the inferior aspect of the radial head, inserting onthe supinator crest of the ulna. 8 Unlike the aMCL, the LUCL originates in the precise center of rotation of the elbow; this is important when reconstructing the ligament.Secondary stabilizers include the radial head and dynamic constraints such as the flexor and extensor muscles of the forearm.When the elbow is extended, the anterior joint capsule contributes about 15% of varus-valgus stability. 9The radial head does not resist physiologic valgus stress in the presence of an intact aMCL; however, it plays a major role in the presence of aMCL insufficiency.O'Driscoll has described the termring of disabilityto describe series of pathologic events that result in ulnohumeral dislocation.A simple elbow dislocation begins with an extension varus stress that disrupts the LUCL and progresses medially with tearing of the anterior and posterior capsules. This allows the ulna to “perch” on the distalhumerus. Further soft tissue or osseous injury results in dislocation 13 (FIG 1A).Most traumatic injuries to the LUCL result in avulsion of the ligament from the lateral humerus ( FIG 1B).As forces continue from lateral to medial across the joint, the anterior and posterior capsular tissues and eventually the medial collateral ligament (MCL) may be disrupted; however, it is theoretically possible todislocate the ulnohumeral joint with disruption of the LUCL and preservation of the aMCL. 12O'Driscoll et al 12 has proposed the termposterolateral rotatory instability(PLRI) to describe the condition of chronic LUCL insufficiency resulting in rotatory recurrent ulnohumeral instability.Fractures may occur with elbow dislocations, and the risk of recurrent instability increases significantly with complex dislocations. These fractures commonly include radial head or neck and coronoid fractures, although any fracture about the elbow may be observed.Radial head fractures are usually readily apparent on plain radiographs.Coronoid fractures may be subtle, and even a “fleck” of coronoid is often a hallmark of a more significant injury (eg, “terrible triad” injury), and its importance should not be underestimated.Recently, a variant of elbow instability termedposteromedial rotatory instability(PMRI) has been described. PMRI is the sequela of a LUCL injury and a medial coronoid facet fracture. This injury pattern is most commonly observed without radial head fracture, making it potentially very subtle on plain radiographs. A computed tomography (CT) scan can delineate this injury in detail and should be obtained if any suspicionexists ( FIG 1C-E).2,11
ETIOLOGY AND CLASSIFICATION
Most elbow dislocations occur with a fall on an outstretched arm.Forces of valgus, extension, supination, and axial compression across the joint can result in the ulna rotating away from the humerus, disrupting lateral anterior soft tissues initially, and dislocating the elbow.Simple elbow dislocations are classified by the direction of displacement of the ulna in reference to the humerus, with posterolateral dislocation the most common.Less common variants include anterior, medial, or lateral dislocations.
PATIENT HISTORY AND PHYSICAL FINDINGS

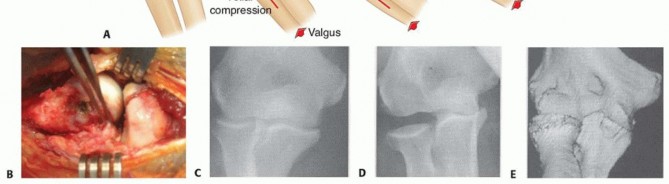
FIG 1 • A. PLRI follows a typical progression of disruption, allowing the joint to become perched and then dislocate as soft tissue injury progresses. B. Intraoperative photograph demonstrating avulsion of the origin of the LUCL after traumatic dislocation of the elbow. The origin of the LUCL and the extensor muscles are avulsed as one layer, held by the forceps. C-E. PMRI is a variant of elbow instability in which the elbow dislocates, rupturing the LUCL, and the medial coronoid sustains an impaction fracture. C,D. In this injury pattern, the radial head remains intact, making appropriate diagnosis of the severity of the injury difficult on standard radiographs. CT scans help better delineate the injury pattern. E. Impaction fracture can be seen on the 3-D CT reconstruction. (A: Adapted from O'Driscoll SW, Morrey BF, Korinek S, et al. Elbow subluxation and dislocation: a spectrum of instability. Clin Orthop Relat Res 1982;280:194; C-E: Copyright the Mayo Foundation, Rochester, MN.) Iatrogenic injury of the LUCL (during procedures such as open tennis elbow release or radial head fracture management) is a known cause of recurrent PLRI. However, these patients often complain of subtle lateral elbow pain due to subluxation of the joint with activities, such as rising from a chair, but rarely have recurrent dislocation.Examination at the time of injury requires attention to the neurovascular anatomy.Nerve injury can occur after elbow dislocation, and a thorough neurologic examination of the extremity is mandatory before any treatment of the dislocation.Most nerve injuries are neurapraxia that often resolve.The ulnar nerve is most frequently involved, although median or radial nerve injury may also occur. 14The dislocated elbow has obvious deformity, with the elbow typically held in a varus position and the forearm supinated.After initial reduction, the neurovascular status of the limb is reevaluated. Loss of neurologic function after closed reduction is rare but can be an indication for surgical exploration to rule out an entrapped nerve.Stability of the joint is assessed based on the amount of extension obtainable and association of pronation or supination with instability.It is helpful to evaluate the stability throughout the elbow range of motion while the patient is still anesthetized, as this may guide treatment (examination under anesthesia).Stressing of the lateral soft tissues is performed with the lateral pivot shift maneuver, which can be performed under anesthesia and with fluoroscopic imaging 12 (FIG 2).This test can be used to assess the degree of PLRI and may aid in determining treatment.Medial ecchymosis may be a sign of an aMCL injury and often is apparent 3 to 5 days after dislocation when the MCL has been injured.
IMAGING AND OTHER DIAGNOSTIC STUDIES
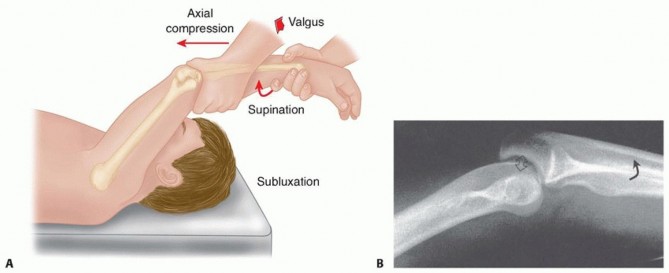
FIG 2 • A. The lateral pivot shift maneuver is performed with the patient's arm positioned overhead, and a supination valgus stress is applied. As the elbow is brought into flexion, the joint reduces, often with a clunk. B. When performed under fluoroscopy, subluxation of the radial head posterior to the capitellum can be observed, consistent with PLRI. (B: From O'Driscoll SW, Bell DF, Morrey BF. Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73[3]:440-446.) Magnetic resonance imaging (MRI) is usually not necessary in the management of acute simple dislocation;however, it can be useful in the case of recurrent PLRI.
NONOPERATIVE MANAGEMENT
Most simple dislocations may be managed nonoperatively with splinting or bracing, guided by the degree of instability determined during the examination under anesthesia after reduction. 12Once reduced, elbow stability is assessed during flexion-extension in neutral forearm rotation.If the elbow is stable throughout an arc of motion, it is immobilized in a sling or splint for 3 to 5 days for comfort and then range-of-motion exercises are initiated.If instability is present in less than 30 degrees of flexion, the forearm is pronated and stability is reassessed.If pronation confers stability, then a hinged orthosis that maintains forearm pronation is used, after 3 to 5 days of splinting, to allow protected range of motion.Elbows that sublux (confirmed by fluoroscopic imaging) in less than 30 degrees of flexion and pronation of the forearm are managed with a brief period of splinting, followed by a hinged orthosis that controls rotation of the forearm and has an extension block.Elbow instability above 30 degrees of flexion can be an indication for surgical stabilization.Hinged bracing is maintained for 6 weeks, with progressive advancement of extension and rotation, as allowed by stability of the joint.Weekly radiographs are needed to ensure maintenance of a congruent joint during the first 4 to 6 weeks.After 6 weeks, bracing is discontinued, and terminal stretching to regain motion is used if flexion contractures exist.
SURGICAL MANAGEMENT
INDICATIONS
Surgical management is indicated in elbows that are unstable, even when placed in flexion (more than 30 degrees) and pronation, elbows that recurrently subluxate or dislocate during the treatment protocol, or those with associated fractures (“complex” instability).Management of simple dislocation requires repair or reconstruction of the ligamentous structures leading to the instability. By definition, simple dislocation occurs without fracture.An algorithmic approach to ligament repair is used to stabilize the elbow. LUCL insufficiency is felt to be the primary lesion with simple dislocations and is therefore addressed first.The LUCL usually avulses from the humerus and can be repaired in the acute setting.Repair may be performed via bone tunnels in the humerus or with suture anchors, depending on the surgeon's preference.Reconstruction of the LUCL is rarely needed in acute management but is often needed in chronic instability. Reconstruction is performed with autograft (either palmaris or gracilis) or allograft.Repair or reconstruction of the LUCL typically confers stability, even in the face of MCL injury, as the intact radial head is a secondary stabilizer to valgus instability.Persistent instability after LUCL repair is rare and is more commonly observed with fracture-dislocations or chronic instability.If persistent instability exists, the MCL is repaired or reconstructed. A hinged external fixator may beplaced to protect the repair.
PREOPERATIVE PLANNING
Planning should include preparing for the possibility of reconstruction of the LUCL which requires either autograft or allograft tendon.If autograft is to be harvested, a tendon stripper is needed. For allograft, we routinely use semitendinosus tendon.P.117A hinged external fixator should be available in the rare case that the elbow remains unstable after ligamentous repair or reconstruction.A 2.0- and 3.2-mm drill bits or burrs are used to make bone tunnels for LUCL repair or reconstruction.Some surgeons prefer suture anchor repair of ligament avulsions; if desired, these should be available.Fluoroscopy is useful for confirming reduction and is required for placement of a hinged external fixator. A sterile tourniquet is used to provide a bloodless surgical field.
PATIENT POSITIONING
Patients are positioned supine with the arm on a radiolucent hand table. A small bump is placed under the scapula to aid in arm positioning.The forequarter is draped free to ensure the entire brachium is kept in the surgical field.If hamstring autograft is to be used for LUCL, the leg should be draped free, and a bump is placed under the hemipelvis to aid in exposure.
TECHNIQUES
Lateral Ulnar Collateral Ligament Repair
LATERAL ULNAR COLLATERAL LIGAMENT REPAIR
SURGICAL APPROACH AND ARTHROTOMY


TECH FIG 1 • A. Lateral column skin incision. The lateral incision is centered over the epicondyle and radiocapitellar joint and is often the primary incision, as the LUCL rupture is thought to be the primary injury in simple dislocations. B. The deep interval between the ECU and anconeus is used to gain exposure to the joint. This is often identified by a fat stripe in the fascia. Care should be taken not to violate the LUCL, which traverses in line with this interval deep to the fascia and supinator muscle. The elbow joint is then exposed by incising the proximal capsule along the lateral column of the humerus, continuing distally along the radial neck (through the supinator muscle and underling capsule) in line with the ECU-anconeus interval.The posterior interosseous nerve (PIN) is at risk with this exposure, and therefore, the forearm is kept in pronation to protect the PIN.The radiocapitellar joint and coronoid are inspected to confirm no fractures are present and that no soft tissue is interposed in the joint, preventing reduction.Once the joint is clear of debris, the ability to obtain a concentric reduction is confirmed with fluoroscopy.
LIGAMENT REPAIR
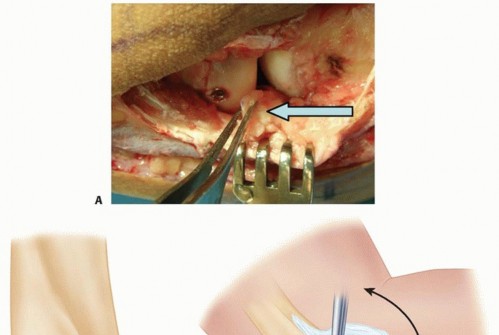
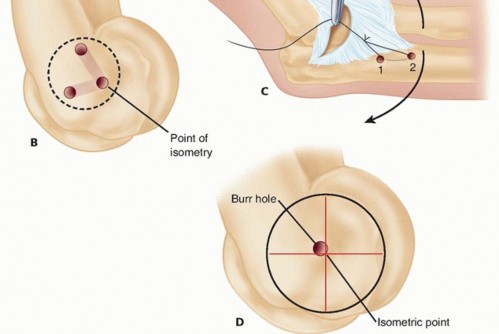
TECH FIG 2 • A. The origin of the LUCL, which often avulses during elbow dislocation, is identified by a fold of tissue on the deep surface of the capsule. The isometric point of the joint is in the center of rotation of the capitellum (B), and confirmation is made using the previously placed sutures in the ligament remnant to ensure that an isometric repair will be obtained (C). D. It is important to make the humeral tunnel so that the most anterior aspect of the tunnel is placed at the isometric point. Exit holes for the humeral tunnel are made anterior and posterior to the lateral supracondylar ridge (B). The isometric origin on the humerus is then identified in the center of the capitellum, not the lateral epicondyle ( TECH FIG 2B,C).Confirmation of the isometric point is made by clamping the limbs of the running suture at the point of isometry and then flexing and extending the elbow to confirm proper placement.A 2.0-mm burr is used to make a humeral bone tunnel.It is critical to make the most anterior aspect of the bone tunnel at the isometric point, not the center of the tunnel, as this small translation can result in a lax LUCL repair ( TECH FIG 2D).Two “exit” tunnels (in a Y configuration), one anterior and one posterior to the lateral column, are thenmade with a 2.0-mmdrill bit or burr, connected to the distal humeral tunnel at the isometric point.P.119Once the humeral tunnels are completed, the limbs of the running suture are passed through the humeral tunnels.The joint is concentrically reduced with fluoroscopic confirmation, and the LUCL repair sutures are then tied with the joint reduced and the elbow in 30 degrees of flexion and neutral rotation.The elbow is ranged through an arc of motion to assess stability, with careful attention placed on the radial head's articulation with the capitellum, looking for posterior sag in extension, indicating either a lax LUCL or a nonisometric repair.If the elbow is stable through an arc of motion, the extensor origin is repaired with interrupted, heavy (no. 0) nonabsorbable suture, and the skin is closed in layers.1. Lateral Ulnar Collateral Ligament ReconstructionOccasionally, the native LUCL is damaged beyond repair (more often with iatrogenic PLRI than with primary instability) or attenuated after recurrent or chronic elbow instability, and reconstruction is necessary.Autograft palmaris, autograft gracilis, or allograft may be used.Autograft and allograft options should be discussed with the patient and decisions made preoperatively. We routinely use semitendinosus allograft unless the patient desires autograft.
BONE TUNNEL PREPARATION
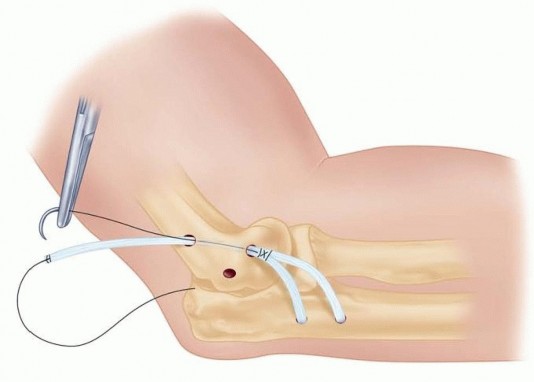
TECH FIG 3 • The insertion of the LUCL is the supinator crest of the ulna. Reconstruction uses an ulnar tunnel in the supinator crest made at the level of the radial head. Holes are made about 1 cm apart and connected to form a tunnel. Furthermore, the docking tunnel is widened using a 3.4-mm burr to be able to accept both limbs of the graft.It is important to widen the docking hole anterior and proximal to the isometric point, as the most posterior aspect of the tunnel needs to be at the isometric point.
GRAFT PREPARATION
One end of the graft is freshened and tubularized using a no. 2 nonabsorbable suture in a running Krackow fashion.The graft is then passed through the ulnar bone tunnels using the passage suture previously placed.The limb of the graft with locking suture is then fully docked into the humeral origin, and the joint is reduced.The final length of the graft is determined by tensioning the graft and identifying the point at which the free limb of the graft meets the isometric origin. This point is marked on the graft.Care should be taken to ensure appropriate graft tension and length by fully docking the first limb and then marking the free limb at the point of initial contact with the humerus, thereby allowing some overlap of graft limbs in the humeral tunnel but minimizing the likelihood of slack in the final construct.The marked graft end is then freshened and tubularized in an identical fashion as the other limb.
FINAL RECONSTRUCTION
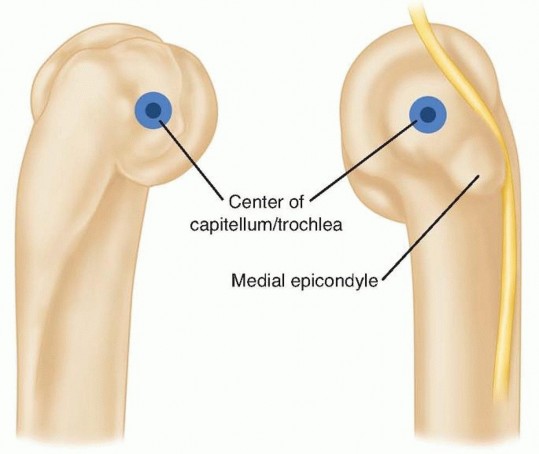
TECH FIG 4 • The center of rotation of the elbow, along which an axis pin for hinged fixators is placed, is identified by the center of the capitellum and just anteroinferior to the medial epicondyle. After placement of the axis pin, the humeral and ulnar pins are placed after confirmation of concentric reduction of the elbow is made.Once the external fixator is fully constructed, the elbow is taken through an arc of motion, and maintenance of reduction is confirmed.Fixators are kept on for 6 to 8 weeks.Meticulous pin care is necessary to minimize pin tract infections or loosening.
PEARLS AND PITFALLS
LUCL avulsion is the primary ligamentous injury in most simple dislocations of the elbow.If the radial head and coronoid are intact (as is the case in a simple dislocation), the MCL rarely needs to be repaired or reconstructed, as the radial head acts as a secondary stabilizer in the elbow with a repaired lateral ligament complex.The LUCL origin can be identified by a capsular fold of tissue. This is the point at which repair sutures should be placed, not at the origin of the more superficial extensor tendons.The isometric origin of the LUCL is in the center of the capitellum, as projected onto the lateral column, and repair or reconstruction needs to be brought to this point to have an isometric ligament.Bone tunnels in the humerus for repair or reconstruction are made so the anteroinferior aspect of the tunnel is at the isometric origin.A hinged external fixator may be necessary in management of elbow dislocation, especially chronic or recurrent situations, and should be available.All hinged fixators are constructed around the axis of rotation of the elbow, identified by a line between the isometric point on the lateral capitellum, and the center of rotation of the trochlea on the medial aspect of the joint.Stiffness is the most common adverse sequela of elbow dislocation, and therefore, range of motion should be started as soon as soft tissue and skin healing allows, with care taken to avoid varus or valgus stress.
POSTOPERATIVE CARE
P.121After operative stabilization without external fixation, the elbow is splinted in 90 degrees of flexion for 3 to 5 days to allow wound healing.Range-of-motion exercises are then begun in flexion, extension, and rotation, with care taken to avoid varus or valgus stress.A hinged orthosis can be helpful in protecting the ligament repair or reconstruction.Active and passive motion is continued for 6 weeks, when strengthening is added.Residual contractures, often loss of extension, can be managed with static splinting and terminal stretching.Most patients return to full activity by 4 to 6 months.
OUTCOMES
Most series have reported the results of closed management of simple dislocation.Mehlhoff and colleagues 7 reported the results of 52 simple dislocations managed, with most patients having normal elbows. Length of immobilization, especially greater than 3 weeks, was found to be more likely to result in persistent loss of extension.Similarly, Eygendaal and colleagues 3 reported the long-term results of 50 patients after closed management of simple dislocations. Sixty-two percent of patients described their elbow function as good or excellent, and 24 of 50 (48%) patients had loss of extension of 5 to 10 degrees.Some series have examined the surgical management of PLRI, often as a result of recurrent instability after traumatic dislocation.Nestor and colleagues 10 reported the results of 11 patients with recurrent PLRI managed with either repair or reconstruction of the LUCL. Ten of 11 (91%) remained stable and 7 of 11 (64%) had an excellent result.More recently, Sanchez-Sotelo and colleagues 15 reported the results of 44 patients treated for recurrent PLRI (9 occurred after simple dislocation). Thirty-two (75%) of the patients had an excellent result by Mayo score.Lee and Teo 5 found that in patients with chronic PLRI, reconstruction offered more predictable outcomes than repair.
COMPLICATIONS
Stiffness 3,7Heterotopic ossification 6 Neurovascular injury14Recurrent instability 3,7 Compartment syndrome Hematoma or infection
REFERENCES
- Dodson CC, Thomas A, Dines JS, et al. Medial ulnar collateral ligament reconstruction of the elbow in throwing athletes. Am J Sports Med 2006;34:1926-1932.
- Doornberg JN, Ring DC. Fracture of the anteromedial facet of the coronoid process. J Bone Joint Surg Am 2006;88(10): 2216-2224.
- Eygendaal D, Verdegaal SH, Obermann WR, et al. Posterolateral dislocation of the elbow joint. Relationship to medial instability. J Bone Joint Surg Am 2000;82(4):555-560.
- Jupiter JB, Ring D. Treatment of unreduced elbow dislocations with hinged external fixation. J Bone Joint Surg Am 2002;84-A(9): 1630-1635.
- Lee BP, Teo LH. Surgical reconstruction for posterolateral rotatory instability of the elbow. J Shoulder Elbow Surg 2003;12: 476-479.
- Linscheid RL, Wheeler DK. Elbow dislocations. JAMA 1965;194: 1171-1176.
- Mehlhoff TL, Noble PC, Bennett JB, et al. Simple dislocation of the elbow in the adult. Results after closed treatment. J Bone Joint Surg Am 1988;70(2):244-249.
- Morrey BF, An KN. Functional anatomy of the ligaments of the elbow. Clin Orthop Relat Res 1985;(201):84-90.
- Morrey BF, Tanaka S, An KN. Valgus stability of the elbow. A definition of primary and secondary constraints. Clin Orthop Relat Res 1991;(265):187-195.
- Nestor BJ, O'Driscoll SW, Morrey BF. Ligamentous reconstruction for posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1992;74(8):1235-1241.
- O'Driscoll SW. Acute, recurrent, and chronic elbow instabilities. In: Norris TR, ed. Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont: American Academy of Orthopaedic Surgeons, 2002:313-323.
- O'Driscoll SW, Bell DF, Morrey BF. Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73(3):440-446.
- O'Driscoll SW, Morrey BF, Korinek S, et al. Elbow subluxation and dislocation. A spectrum of instability. Clin Orthop Relat Res 1992;(280):186-197.
- Rana NA, Kenwright J, Taylor RG, et al. Complete lesion of the median nerve associated with dislocation of the elbow joint. Acta Orthop Scand 1974;45:365-369.
- Sanchez-Sotelo J, Morrey BF, O'Driscoll SW. Ligamentous repair and reconstruction for posterolateral rotatory instability of the elbow. J Bone Joint Surg Br 2005;87(1):54-61.
- Tan V, Daluiski A, Capo J, et al. Hinged elbow external fixators: indications and uses. J Am Acad Orthop Surg 2005;13:503-514.
