Introduction to Malunited Fractures
A malunited fracture is strictly defined as a fracture that has healed with the osseous fragments in a nonanatomical position. While minor degrees of malunion are common—and often represent the expected outcome in the closed, conservative management of certain fractures—they frequently remain compatible with excellent clinical function. A malunited fracture only crosses the threshold into surgical significance when the resulting deformity actively impairs the patient's biomechanical function, causes intractable pain, or precipitates early-onset arthrosis.
Whether the resulting deformity is cosmetically unsightly or clinically subtle, it can impair the musculoskeletal system through four primary mechanisms:
1. Abnormal Joint Surface Kinematics: Intra-articular or peri-articular malunions cause irregular weight transfer across the articular cartilage. This focal overloading rapidly accelerates the degradation of the joint, leading to post-traumatic osteoarthritis, particularly in the weight-bearing joints of the lower extremities.
2. Rotational and Angular Deformities: Alterations in the mechanical axis interfere with proper muscle balance, lever-arm mechanics, and gait efficiency in the lower extremities. In the upper extremities, rotational malunions severely restrict spatial positioning and fine motor function of the hand.
3. Limb Length Discrepancy: Overriding of fracture fragments, impaction, or frank bone loss during the initial trauma can result in perceptible and functionally limiting limb shortening.
4. Mechanical Block to Motion: Prominent malunited fragments or exuberant callus formation can physically impinge upon neighboring joints, restricting their physiological arc of motion.
Clinical Pearl: The objective of surgery for a malunion is strictly to restore function and prevent secondary arthrosis. Although improving the cosmetic appearance of the limb may be of paramount importance to the patient, operative intervention is rarely, if ever, justified for cosmetic reasons alone.
Etiology and Risk Factors
Malunions generally arise from either inaccurate initial reduction or ineffective immobilization during the critical phases of bone healing. While most malunions can be prevented by the skillful, evidence-based treatment of fresh fractures, they occasionally occur despite the most expert surgical or conservative management due to patient non-compliance, severe comminution, or compromised biology.
The Polytrauma Patient
Kenzora and Burgess have extensively documented the high incidence of malunion development in patients with multiple traumatic injuries. In the acute polytrauma setting, life-saving interventions and the stabilization of major long-bone or pelvic fractures take absolute precedence. Consequently, seemingly innocuous, nondisplaced fractures—particularly those around the foot, ankle, and hand—may be underappreciated or intentionally managed with benign neglect.
Furthermore, in patients with severe traumatic brain injuries, the combination of altered pain perception, inability to comply with weight-bearing restrictions, and severe spasticity frequently leads to the late displacement of initially acceptable fractures. This results in profound deformity and disability that only becomes apparent months later when the patient regains mobility and cognitive function.
Hierarchy of Deformity Correction
When evaluating a malunion and planning corrective surgery, the surgeon must adhere to a strict hierarchy regarding the acceptability of fracture reduction and the goals of reconstruction. Of the four primary characteristics that determine a successful mechanical restoration, they are prioritized as follows:
- Alignment (Axial): Restoration of the mechanical axis is of paramount importance to ensure joint surfaces are loaded orthogonally.
- Rotation: Correcting torsional deformities is critical, as rotational malalignment is poorly tolerated, especially in the lower extremity (affecting foot progression angle) and the forearm (limiting pronosupination).
- Length: Restoration of normal limb length is the third priority, often requiring complex distraction techniques if the discrepancy exceeds 2-3 centimeters.
- Apposition (Position of Fragments): The actual anatomical position or translation of the diaphyseal fragments is the least important factor, provided the mechanical axis, rotation, and length are restored.
Surgical Warning: A seemingly slight angular deformity can be profoundly disabling when the malunion involves an articular surface or is located in the immediate peri-articular metaphysis. Conversely, diaphyseal translation without angulation is often functionally asymptomatic.
Pediatric Considerations in Malunion
The management of malunited fractures in the pediatric population requires a thorough understanding of physeal growth and remodeling potential. Deformities of axial alignment in children younger than 9 years of age possess a remarkable capacity to correct spontaneously with subsequent growth.
This spontaneous remodeling is highly predictable if the deformity meets two criteria:
* It is located near a joint (peri-articular metaphysis).
* The angulation is in the primary plane of motion of that adjacent joint (e.g., flexion/extension plane of the knee or wrist).
Similarly, a translational offset in an epiphysis will usually correct itself spontaneously through physeal growth, provided the physis itself was not irreversibly damaged (e.g., Salter-Harris crush injuries leading to physeal bar formation). However, rotational deformities and intra-articular step-offs do not remodel and require anatomical surgical correction regardless of the child's age.
Radiographic Evaluation and Trigonometric Analysis
Standard anteroposterior (AP) and lateral radiographs are the foundation of malunion evaluation. However, the surgeon must recognize that most deformities are oblique—existing in a plane that is neither purely coronal nor purely sagittal. The AP and lateral views merely represent two-dimensional projections of a three-dimensional deformity.
To accurately plan a corrective osteotomy, the true plane and magnitude of the maximal deformity must be calculated. Ries and O’Neill developed a highly effective trigonometric analysis of deformity, designing a graphical method to determine the true maximal angulation based on standard orthogonal radiographs.
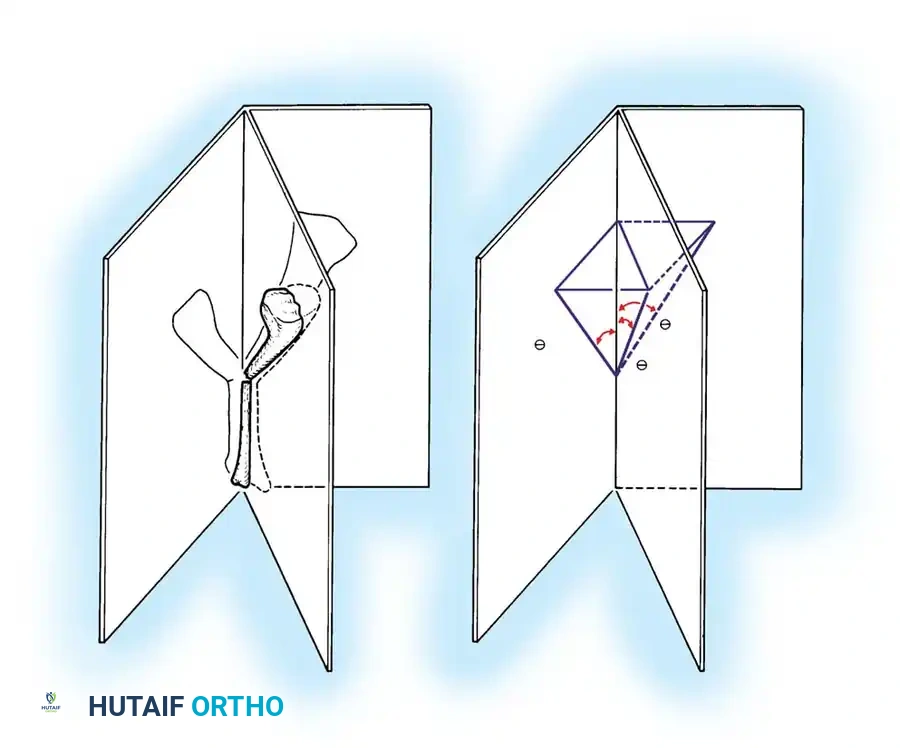
Fig. 55-1 Ries and O’Neill method for determining bony deformity from anteroposterior and lateral radiographs. A, Tibial fracture angulated in a plane between the anteroposterior (AP) and lateral (LAT) planes. B, Angles formed by the tibial fracture. CAD is the angle shown on the anteroposterior view, CAB is the angle shown on the lateral view, and CAE is the angle in the true plane (T) of the deformity. (Redrawn from Ries M, O’Neill D: A method to determine the true angulation of long bone deformity, Clin Orthop Relat Res 218:191, 1987.)
Further advancing this concept, Harper, Canale, and Cobb published detailed trigonometric analyses of angulation osteotomies. By identifying the true plane of the deformity, the surgeon can execute a single-cut osteotomy (such as a closing wedge or opening wedge) oriented perfectly perpendicular to the true plane, thereby correcting both the AP and lateral angulations simultaneously. Advanced preoperative planning today often supplements these trigonometric principles with 3D computed tomography (CT) reconstructions and computer-aided design (CAD) software to map the Center of Rotation of Angulation (CORA).
Timing of Surgical Intervention
The timing of corrective surgery is a critical variable that significantly impacts the outcome. As a general rule, operative treatment for the malunion of diaphyseal fractures should not be considered until 6 to 12 months after the initial injury. This delay allows for:
* Complete resolution of the initial soft-tissue envelope trauma.
* Maturation of the fracture callus.
* Maximization of functional rehabilitation, which may reveal that the malunion is actually well-tolerated and does not require surgery.
Exceptions to the Rule:
In cases of intra-articular malunions, delayed intervention is contraindicated. Surgery must be undertaken as soon as the soft tissues permit (often within weeks) to restore articular congruity before irreversible chondral damage and post-traumatic arthrosis occur.
Preoperative Optimization
Before committing to surgery, the surgeon must meticulously evaluate the degree of regional osteoporosis and soft-tissue atrophy resulting from disuse. A strategic decision must be made regarding whether early surgery is preferable, or if a period of intensive, active physical rehabilitation is required to optimize bone density and soft-tissue compliance prior to osteotomy and internal fixation.
Surgical Strategies and Step-by-Step Approaches
Corrective surgery directly at the site of the malunion (anatomical correction) is the gold standard but is not always feasible due to poor soft-tissue coverage, compromised vascularity, or severe bone loss. In such instances, alternative strategies must be employed.
1. Corrective Osteotomy at the Apex of Deformity
When local conditions permit, an osteotomy at the CORA is performed.
* Opening Wedge Osteotomy: Restores length but creates a cortical void requiring structural bone grafting (autograft or allograft). It relies heavily on the integrity of the periosteal hinge on the concave side.
* Closing Wedge Osteotomy: Highly stable with excellent bone-to-bone contact, but inherently shortens the limb. Best utilized when the limb is already at length or slightly long.
* Dome Osteotomy: Allows for angular and rotational correction without altering limb length or creating a large gap, though technically demanding to execute.
General Step-by-Step Approach:
1. Positioning and Exposure: The patient is positioned on a radiolucent table. An extensile approach is utilized, avoiding previous compromised incisions if possible. Meticulous soft-tissue handling is paramount to preserve periosteal blood supply.
2. Guidewire Placement: Under fluoroscopic guidance, K-wires are placed to mark the planned osteotomy trajectory based on preoperative trigonometric calculations.
3. The Osteotomy: Using an oscillating saw under continuous saline irrigation (to prevent thermal necrosis), the bone is cut.
4. Mobilization and Reduction: The fragments are mobilized. Soft-tissue releases (e.g., fractional lengthening of contracted muscles) may be required to achieve the new position.
5. Rigid Internal Fixation: The corrected alignment is stabilized using absolute stability constructs (e.g., dynamic compression plates) for diaphyseal corrections, or locking plates for metaphyseal/osteoporotic bone.
6. Bone Grafting: Any resulting defects are packed with cancellous autograft (typically harvested from the iliac crest or proximal tibia) to stimulate osteogenesis.
2. Compensatory Procedures
If the malunion site is biologically hostile (e.g., heavily irradiated tissue, severe scarring), a compensatory osteotomy can be performed at a distant, healthy site. While this creates a secondary deformity, it realigns the overall mechanical axis of the limb parallel to the joint line, restoring functional weight-bearing.
3. Salvage Procedures
In cases where the malunion has already resulted in end-stage joint destruction, or where pain is the predominant and intractable symptom, corrective osteotomy alone will fail. In these scenarios, arthrodesis (joint fusion) or total joint arthroplasty becomes the necessary salvage procedure to provide a stable, painless limb.
Advanced Reconstruction: The Ilizarov Method
For the most complex malunions—particularly those complicated by active infection, infected nonunions, severe soft-tissue compromise, or massive bone loss—conventional open reduction and internal fixation techniques are often contraindicated. In these challenging scenarios, the principles pioneered by Gavriil Ilizarov utilizing circular external fixation and distraction osteogenesis are invaluable.
Biomechanics of Circular Fixation
The Ilizarov apparatus utilizes tensioned fine wires (1.5 to 1.8 mm) attached to external rings. This construct provides a unique biomechanical environment: it is axially dynamic (promoting micromotion and bone healing) but highly stable against shear and torsional forces.
Intercalary Limb Regeneration
Through the use of various hinged constructs and threaded rods, the Ilizarov frame allows for the simultaneous and gradual restoration of alignment, rotation, and length.
* A corticotomy (a low-energy osteotomy preserving the medullary blood supply and periosteum) is performed.
* After a latency period of 7 to 10 days, gradual distraction is initiated at a rate of approximately 1 mm per day (divided into four 0.25 mm increments).
* This tension-stress effect stimulates the generation of new woven bone (regenerate) parallel to the vector of distraction.
Clinical Pearl: The Ilizarov technique requires a profound understanding of spatial frame design, meticulous pin-site care, and intensive patient counseling. The psychological burden on the patient is high, and rigorous, daily physical therapy is mandatory to prevent severe joint contractures during the lengthening phase.
While highly demanding, circular fixation techniques have revolutionized the surgical approach to malunions, offering impressive, limb-saving results in situations that historically would have culminated in amputation.
Postoperative Protocols and Rehabilitation
The postoperative management of a corrected malunion is dictated by the method of fixation and the quality of the host bone.
- Internal Fixation: If rigid plate osteosynthesis is achieved, early active and passive range of motion of adjacent joints is initiated immediately to prevent stiffness. Weight-bearing is typically restricted (touch-down only) until radiographic evidence of bridging callus is observed, usually around 6 to 8 weeks postoperatively.
- External Fixation (Ilizarov): Patients are encouraged to bear weight as tolerated immediately, as axial loading stimulates regenerate bone consolidation. Intensive physical therapy focuses on maintaining joint mobility against the increasing tension of the lengthening soft tissues.
In all cases, the ultimate success of malunion surgery relies not only on precise intraoperative execution but on a structured, phased rehabilitation program designed to restore muscle strength, proprioception, and normal gait kinematics.
📚 Medical References
- Malunited fractures of the forearm in children, J Bone Joint Surg 64B:364, 1982.
- Galeazzi R: Di una particulare sindrome: traumatica delle scheletro dell avambraccio, Attie Mem Soc Lombardi di Chir 2:12, 1934.
- Greenbaum B, Zionts LE, Ebramzadeh E: Open fractures of the forearm in children, J Orthop Trauma 15:111, 2001.
- Gupta RP, Danielsson LG: Dorsally angulated solitary metaphyseal greenstick fractures in the distal radius: results after immobilization in pronated, neutral, and supinated position, J Pediatr Orthop 10:90, 1990.
- Hirayama T, Takemitsu Y, Yagihara K, et al: Operation for chronic dislocation of the radial head in children: reduction by osteotomy of the ulna, J Bone Joint Surg 69B:639, 1987.
- Holdsworth BJ, Sloan JP: Proximal forearm fractures in children: residual disability, Injury 14:174, 1982.
- Holmes JR, Louis DS: Entrapment of pronator quadratus in pediatric distal-radius fractures: recognition and treatment, J Pediatr Orthop 14:498, 1994.
- Houshian S, Holst AK, Larsen MS, et al: Remodeling of SalterHarris type II epiphyseal plate injury of the distal radius, J Pediatr Orthop 24:472, 2004.
- Hurst LC, Dubrow EN: Surgical treatment of symptomatic chronic
