INTRODUCTION TO MEDIAN NERVE PALSY RECONSTRUCTION
The median nerve is the primary motor nerve for precision pinch and the critical sensory nerve for the volar aspect of the hand. Paralysis of the median nerve, whether isolated or in combination with ulnar nerve deficits, results in profound functional impairment. Surgical reconstruction through tendon transfer is dictated by the level of the lesion—classified broadly into low and high median nerve palsies—and the presence of concomitant nerve injuries.
Successful restoration of hand biomechanics requires a deep understanding of muscle excursion, tensioning, and the synergistic actions of the wrist and digits. This comprehensive guide details the pathoanatomy, surgical indications, and operative techniques for restoring function in low, high, and combined median-ulnar nerve palsies.
LOW MEDIAN NERVE PALSY
Low median nerve palsy typically results from lesions at or distal to the wrist crease, most commonly secondary to severe carpal tunnel syndrome, lacerations, or distal radius fractures.
Pathoanatomy and Clinical Deficits
The hallmark functional deficits of a low median nerve lesion are the loss of thumb opposition and the loss of sensibility over the radial three-and-a-half digits.
* Motor Deficits: Paralysis affects the abductor pollicis brevis (APB), opponens pollicis (OP), and the superficial head of the flexor pollicis brevis (FPB). This results in an "ape hand" deformity, where the thumb rests in the plane of the palm.
* Lumbrical Paralysis: While the radial two lumbricals are paralyzed, this is of little clinical consequence provided the ulnar nerve remains intact, as the intact interossei prevent index and long finger clawing.
* Sensory Deficits: Loss of tactile gnosis in the critical pinch areas (pulp of the thumb, index, and long fingers) severely limits fine motor tasks, even if motor function is restored.
Clinical Pearl: True opposition is a complex, three-dimensional movement comprising palmar abduction, flexion, and pronation. Any tendon transfer designed to restore opposition (opponensplasty) must replicate this vector, typically pulling from the region of the pisiform toward the metacarpophalangeal (MCP) joint of the thumb.
Surgical Reconstruction: Opponensplasty
Restoration of thumb opposition is the primary surgical goal. Several donor tendons are available, provided they possess adequate excursion (approximately 3-5 cm) and power.
1. Extensor Indicis Proprius (EIP) Transfer (Burkhalter Technique)
The EIP is an excellent donor because its harvest does not result in a functional deficit (the extensor digitorum communis to the index finger remains intact), and it does not require a constructed pulley if routed correctly.
* Incision and Harvest: A transverse incision is made over the index MCP joint to detach the EIP, repairing the extensor hood. A second incision is made over the distal forearm to retrieve the tendon.
* Routing: The EIP is routed subcutaneously around the ulnar aspect of the wrist (using the ulnar border of the forearm as a dynamic pulley) and directed diagonally across the palm toward the thumb MCP joint.
* Insertion: The tendon is woven into the APB tendon and the extensor pollicis longus (EPL) over the proximal phalanx to restore both abduction and pronation.
2. Flexor Digitorum Superficialis (FDS) Transfer (Royle-Thompson / Bunnell)
The ring finger FDS provides excellent power and excursion. It is harvested in the palm, retrieved in the distal forearm, and routed through a constructed pulley (often utilizing the flexor carpi ulnaris or the transverse carpal ligament) to direct the vector of pull toward the pisiform.
Sensory Restoration
Restoration of sensibility is paramount for a functional pinch. If primary nerve repair or grafting is impossible or has failed, a neurovascular island pedicle flap (typically harvested from the ulnar border of the ring finger) can be transferred to the volar pad of the thumb. This provides durable, sensate skin to the critical pinch area.
HIGH MEDIAN NERVE PALSY
High median nerve palsy occurs with lesions proximal to the elbow or in the proximal forearm. This results in a devastating loss of both extrinsic and intrinsic hand function.
Pathoanatomy and Clinical Deficits
In addition to the intrinsic deficits seen in low median nerve palsy, high lesions cause paralysis of:
* Pronator Teres and Pronator Quadratus: Loss of active forearm pronation.
* Flexor Carpi Radialis (FCR): Weakened wrist flexion (relying solely on the ulnar-innervated flexor carpi ulnaris).
* Flexor Pollicis Longus (FPL): Inability to flex the thumb interphalangeal (IP) joint.
* Flexor Digitorum Profundus (FDP) to Index and Long Fingers: Inability to flex the distal interphalangeal (DIP) joints of the radial digits, resulting in the classic "Benediction Hand" when attempting to make a fist.
Surgical Reconstruction Strategy
Reconstruction must restore extrinsic finger flexion, thumb flexion, and thumb opposition.
Surgical Warning: Do not attempt to restore all functions simultaneously if joint contractures are present. Passive range of motion must be maximized through therapy prior to any tendon transfer.
1. Restoration of Finger Flexion (Index and Long Fingers)
* FDP Tenodesis: The paralyzed median-innervated FDP tendons of the index and long fingers can be sutured side-to-side to the intact, ulnar-innervated FDP tendons of the ring and small fingers. This provides mass flexion of the digits.
* ECRL Transfer: For greater independent power, the Extensor Carpi Radialis Longus (ECRL) can be transferred to the FDP of the index and middle fingers. The ECRL is detached from the base of the second metacarpal, retrieved in the forearm, and woven into the paralyzed FDP tendons.
2. Restoration of Thumb Flexion
* Brachioradialis (BR) to FPL Transfer: The BR is the ideal motor for restoring thumb flexion due to its strength.
* Technique: The BR is detached from the radial styloid. It is critical to free the BR proximally from its fascial attachments to the forearm to ensure adequate excursion (at least 3 cm). The BR is then woven into the FPL tendon at the musculotendinous junction in the distal forearm.
3. Restoration of Thumb Opposition
As with low median nerve palsy, the EIP transfer routed around the ulnar border of the wrist remains the procedure of choice, as it avoids utilizing volar flexors that may already be compromised or utilized for other transfers.
COMBINED LOW MEDIAN AND ULNAR NERVE PALSY (AT THE WRIST)
Combined median and ulnar nerve lesions at the wrist represent one of the most challenging reconstructive scenarios in orthopedic hand surgery.
Pathoanatomy: The Intrinsic-Minus Hand
This combined lesion results in complete anesthesia of the palm and total paralysis of all intrinsic muscles of the hand (lumbricals, interossei, thenar, and hypothenar muscles).
* Claw Hand Deformity: Without the intrinsic muscles to flex the MCP joints and extend the IP joints, the extrinsic extensors hyperextend the MCP joints, and the extrinsic flexors hyperflex the IP joints.
* Loss of Power Grip and Pinch: The hand loses its ability to cup, the thumb cannot adduct or oppose, and pinch strength is reduced to a fraction of normal. If left untreated, severe skin and joint contractures develop, resulting in a rigid, non-functional clawhand.
Surgical Reconstruction of Power Grip (Burkhalter Principles)
Burkhalter revolutionized the approach to the intrinsic-minus hand by emphasizing the restoration of power grip through strategic tendon insertions. He noted that inserting transferred tendons directly into the proximal phalanx diaphysis of the involved fingers resulted in a more secure attachment and provided a significantly greater lever arm beyond the MCP joint compared to traditional lateral band insertions.
For motor units, Burkhalter utilized the Brachioradialis (BR) or the Extensor Carpi Radialis Longus (ECRL), extended by free tendon grafts (such as plantaris or toe extensors).
Biomechanical Advantage of the Burkhalter Modification:
The tendons are brought dorsally and passed through the intermetacarpal area, volar to the transverse metacarpal ligament, before attaching to the bone. This specific routing ensures that as the MCP joint flexes, the moment arm of the transfer actually increases, thereby maximizing force application where it is needed most for power grip.


Figure A & B: The Burkhalter modification of the Stiles-Bunnell transfer. Notice how the distance of the moment arm increases with increased flexion of the metacarpophalangeal joint. Force applied distally varies with the square of the distance.
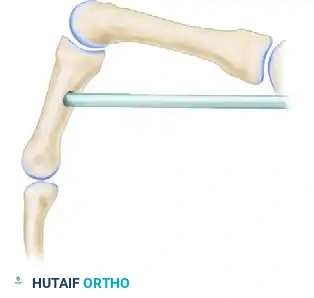
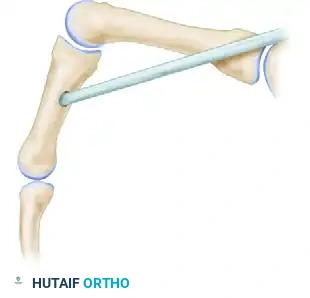
Figure C & D: Demonstration of the intermetacarpal route for this transfer. The moment arm dynamically increases with increasing flexion of the metacarpophalangeal joint, optimizing the biomechanics for power grip restoration.
Burkhalter also applied this same diaphyseal bony attachment when transferring a split FDS of the ring finger, serving as a highly effective modification of the classic Stiles-Bunnell transfer.
Restoration of Thumb Adduction and Pinch
A critical component of the combined palsy is the loss of the adductor pollicis. Without it, key pinch (Froment's sign) is impossible. Several authors have proposed robust solutions:
1. Brown’s Techniques for Adduction:
* FDS Transfer: Brown suggested using the ring finger FDS, brought deep to the finger flexors across the palm, to replicate the transverse head of the adductor pollicis.
* EIP Transfer: Alternatively, the EIP can be brought into the palm around the third metacarpal, running transversely across the palm parallel to the paralyzed adductor muscle, and attached to the MCP joint area of the thumb.
* Arthrodesis: Occasionally, arthrodesis of the thumb IP joint is advised to increase the absolute power of pinch. This is sometimes accompanied by advancing the A1 pulley at the MCP joint (sectioning it proximally) to provide a greater angle of approach for the FPL, thereby increasing its mechanical advantage.
2. Omer’s Techniques for Adduction and Abduction:
* BR Transfer: Omer frequently transferred the brachioradialis tendon, prolonged with a free graft, through the third interosseous space to restore thumb adduction.
* Index Abduction: To restore abduction of the index finger (replacing the first dorsal interosseous to stabilize the finger during pinch), Omer freed the radial half of the EIP insertion, split the tendon, and anchored it to the insertion of the first dorsal interosseous.
Restoration of Digital Balance (Claw Correction)
To correct the clawing of the fingers, the MCP joints must be actively flexed to allow the extrinsic extensors to extend the IP joints.
- Brand’s Transfer (Modified by Brown): Brown advocated for a transfer of the ECRL tendon, prolonged by a four-tailed free graft, routed volar to the deep transverse metacarpal ligament to restore MCP flexion.
- Omer’s Digital Balance Transfers: Omer suggested using the middle finger FDS split into four tails, or the ECRL prolonged by a graft. Other possibilities include splitting the EIP or the Extensor Digiti Quinti Proprius (EDQ) into two tails each, attaching them to the radial digits (2nd and 3rd) and ulnar digits (4th and 5th), respectively.
Restoration of Thumb Opposition in Combined Palsy
Because the median nerve is out, standard FDS transfers are unavailable. Omer suggested using the Extensor Carpi Ulnaris (ECU) tendon, prolonged by the Extensor Pollicis Brevis (EPB) tendon or a palmaris longus free graft, routed around the ulnar border of the wrist to restore opposition. If dynamic transfers are insufficient due to a lack of available donors, carpometacarpal (CMC) joint fusion is highly recommended to place the thumb in a permanent, stable position of function for pinch.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The success of complex tendon transfers relies as much on meticulous postoperative rehabilitation as on surgical execution.
Phase 1: Immobilization (Weeks 0-4)
Postoperatively, the hand and forearm are immobilized in a custom orthosis.
* For opponensplasties, the thumb is immobilized in maximum palmar abduction and opposition.
* For intrinsic replacements (claw corrections), the wrist is placed in neutral to 30 degrees of extension, the MCP joints are immobilized in 70-90 degrees of flexion, and the IP joints are left fully extended.
* Strict elevation and edema control are mandatory to prevent stiffness.
Phase 2: Early Mobilization (Weeks 4-6)
At 4 weeks, the cast or rigid splint is removed, and a removable thermoplastic splint is fabricated.
* Active range of motion (AROM) exercises are initiated.
* Motor Re-education: This is the most critical phase. Patients must be taught to fire the donor muscle to achieve the new action. For example, if the ECRL was transferred for finger flexion, the patient is instructed to attempt wrist extension to initiate finger flexion. Biofeedback and mirror therapy are highly effective adjuncts.
Phase 3: Strengthening and Integration (Weeks 6-12)
- Passive range of motion (PROM) is gently introduced if tendon gliding is restricted, though care must be taken not to stretch out the transfer.
- Progressive resistive exercises (PREs) begin at 8 weeks.
- Dynamic splinting may be utilized if mild contractures develop, but the primary focus remains on integrating the transferred tendons into functional, subconscious movement patterns for power grip and precision pinch.
Pitfall: Over-tensioning a tendon transfer can lead to joint contractures, while under-tensioning results in a lag and failure to restore function. Tendons should generally be tensioned such that the resting posture of the hand mimics the normal physiological cascade under anesthesia.
