Ligament Stabilization of the Unstable Thumb Carpometacarpal Joint
DEFINITION
Thumb carpometacarpal (CMC) joint instability can occur as a result of ligament laxity or trauma.Regardless of the cause, injury to the stabilizing ligaments surrounding the CMC joint leads to instability and dorsoradial subluxation or dislocation of the thumb metacarpal.
ANATOMY
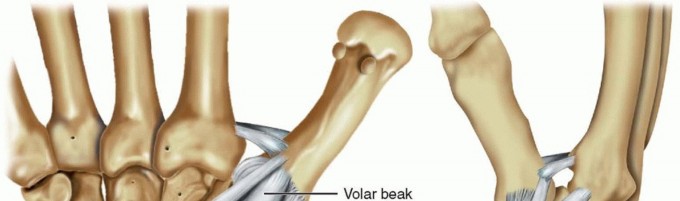
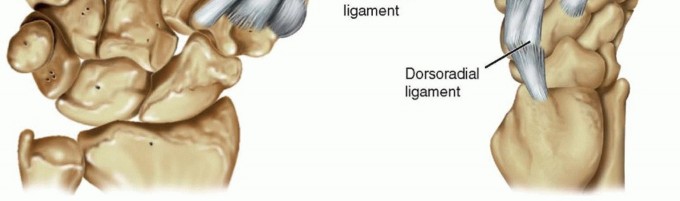
FIG 1 • The stabilizing ligaments of the thumb CMC joint. Of these, the dorsoradial and volar beak ligaments are the most important in preventing dorsoradial subluxation of the thumb metacarpal. The dorsoradial ligament originates from the dorsoradial tubercle of the trapezium and inserts onto the dorsal base of the thumb metacarpal. It is the thickest, widest, shortest, and strongest of the CMCligaments.5
PATHOGENESIS
The biconcave-convex nature of the thumb CMC joint allows for a wide range of thumb motion but is inherently unstable.8 Laxity or incompetence of the supporting ligaments, especially the dorsoradial ligaments, will causeinstability of the thumb CMC joint.12,15 Especially in middle-aged women, the cause of the laxity is often idiopathic.In addition, there is a population of patients who have inherent ligament laxity, such as those with collagen disorders such as Ehlers-Danlos syndrome.In the setting of trauma, acute thumb CMC joint dislocation occurs with axial loading and flexion of the thumb metacarpal. In all reported cases, the dislocation occurs in a dorsoradial direction.14,15
NATURAL HISTORY
Ligamentous laxity at the thumb CMC joint may cause degenerative changes to the joint cartilage and lead to arthritis,corresponding to higher stages in the Eaton-Littler staging system.3P.400If the ligamentous laxity is symptomatic and causing pain, ligament reconstruction can be successful in reducing pain in over 90% of patients. Ligament reconstruction has also been shown to potentially halt theprogression of arthritis.6For traumatic dislocations, a stable reduction is important for thumb function. If the thumb CMC joint remains unstable, functions such as key pinch and grasp may be compromised.Open ligament reconstruction of these unstable thumb CMC joint dislocations may decrease the incidence of recurrent instability and joint degeneration compared to closed reduction and pinning.14
PATIENT HISTORY AND PHYSICAL FINDINGS
NONTRAUMATIC LIGAMENTOUS LAXITY
The history should include questions about ligament laxity involving other joints. Metabolic diseases such as Ehlers-Danlos syndrome are notable.Radiographic findings often do not correlate with symptomatology. Therefore, it is important to elicit from the patient the exact symptoms and their severity.Any history of previous nonoperative treatments should be noted. If splinting and steroid injections have not been attempted, it may be beneficial to attempt these treatment modalities before discussing surgery.The physical examination should determine the degree of subluxation and reducibility of the thumb CMC joint. The thumb metacarpophalangeal (MCP) joint should also be examined for possible hyperextension laxity.Pinch strength and opposition should be tested and compared to the contralateral side.The hand should also be evaluated for concomitant carpal tunnel syndrome, flexor carpi radialis tunnel syndrome, and de Quervain tenosynovitis, as these may also need to be addressed.
TRAUMATIC INJURIES
In addition to the evaluation cited for nontraumatic laxity, the history and physical examination should include the following:Time and nature of the injury Status of the thumb before injuryStability of joint reduction: This is of major concern in the physical examination because assessment of stability will determine the treatment path.Associated MCP joint collateral ligament injury and stability Other associated hand injuries are important to note as well. Tests to perform include the ballottement test and the grind test.Tenderness associated with dorsal pressure indicates symptomatic subluxation.Crepitance and pain are positive indicators of CMC pathology.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Anteroposterior (AP), lateral, and oblique views of both thumbs should be obtained.A true AP (Robert) view is taken with the forearm in maximal pronation and the dorsum of the thumb resting on the imaging table. The beam is then angled 15 degrees from distal to proximal.5A true lateral film of the thumb is one in which the sesamoids volar to the thumb MCP joint overlap each other.A 30-degree oblique stress view of the thumb CMC joint is performed by pressing the radial side of the thumb tips together. This maneuver will subluxate the thumb metacarpal base radially, therebydemonstrating the degree of laxity in the radial direction.17
DIFFERENTIAL DIAGNOSIS
de Quervain tenosynovitisFlexor carpi radialis tunnel syndrome C6 radiculopathyTrigger thumb
NONOPERATIVE MANAGEMENT
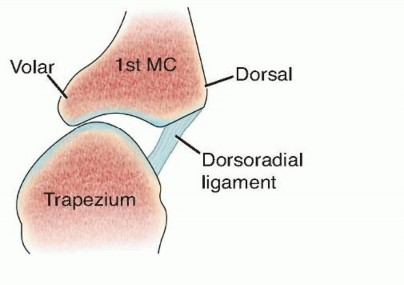
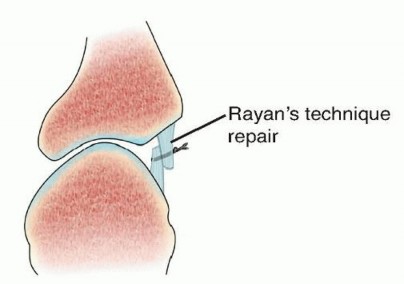
FIG 2 • Rayan's technique for thumb CMC stabilization: the dorsoradial ligament is imbricated and tightened and the CMC joint is pinned with a .045 K-wire for 4 weeks.13
SURGICAL MANAGEMENT
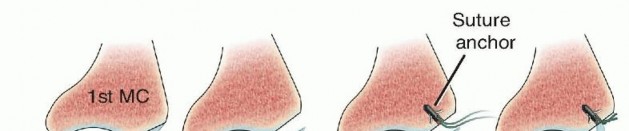
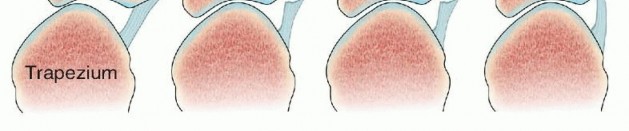
FIG 3 • The technique favored by Rosenwasser: the dorsoradial ligament is advanced into a suture anchor placed into the thumb metacarpal base in order to stabilize the CMC joint. The joint is immobilized in a thumb spica splint for 4 weeks, no pin is used. When the injury pattern results in fracture-dislocations such as unstable Bennett and Rolando fractures, percutaneous pinning or open reduction and internal fixation may be the treatment of choice.
PREOPERATIVE PLANNING
Plain films should be reviewed.In the case of acute trauma, associated fractures and hand injuries should be addressed.A preoperative Allen test should be performed because all procedures involving the thumb CMC joint are in close vicinity to the radial artery and iatrogenic injury may occur.
POSITIONING
The procedure is performed with the patient supine and the arm on a standard hand table.The operating table should be turned away from the anesthesia machines to allow the surgeon and assistant to sit across from each other at the hand table.
APPROACH
A number of techniques have been described for ligament reconstruction of the thumb CMC joint using a variety of different tendons, including the flexor carpi radialis, palmaris longus, extensor carpi radialis longus, extensor pollicis brevis, and abductor pollicis longus (APL).The technique presented here is the classic volar ligament reconstruction described by Eaton and Littler.4This method effectively reconstructs both the volar and dorsal ligaments using the flexor carpi radialis.
TECHNIQUES
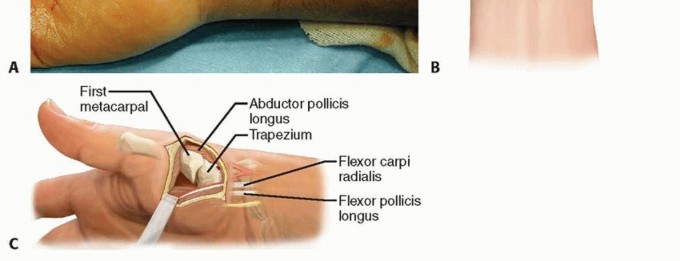
Modified Wagner Approach to the Thumb Carpometacarpal Joint


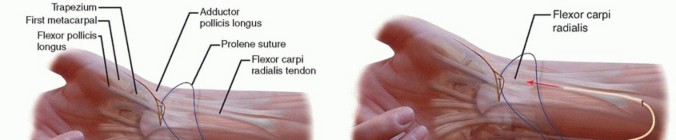

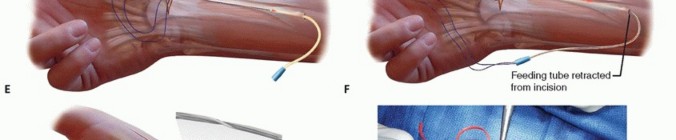
TECH FIG 2 •(continued)C. A longitudinal split is made through the flexor carpi radialis distally and a 0 Prolene suture is passed through it. D. A pediatric feeding tube is passed from the proximal to the distal wound. E. The Prolene suture is then passed through the feeding tube from distal to proximal. F. The feeding tube is removed, leaving the Prolene suture ends in the proximal wound. G. The two suture ends are pulled, thereby dividing the flexor carpi radialis tendon in half until the proximal wound is reached. The flexor carpi radialis tendon spirals, so the distal radial half corresponds to the proximal ulnar half of the tendon. H. The split flexor carpi radialis tendon is delivered into the distal wound.
Metacarpal Tunnel Placement and Flexor Carpi Radialis Graft Passage and Fixation
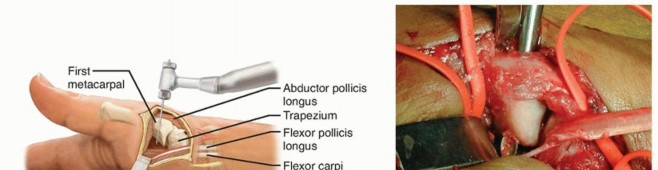


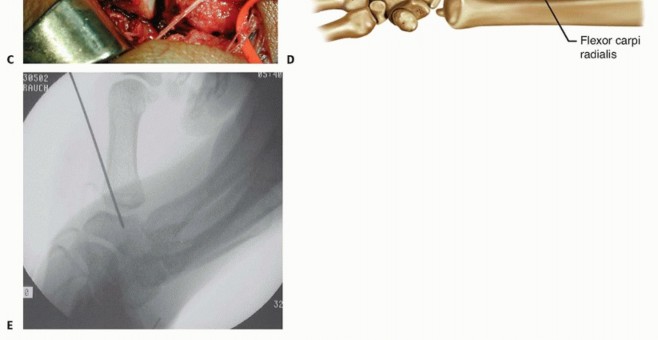
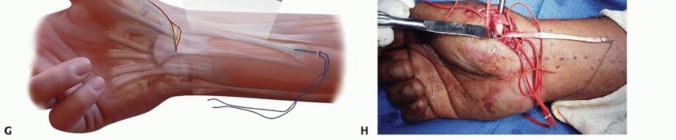
TECH FIG 3 • A. The tunnel is drilled from dorsal to volar, staying parallel and 1 cm distal to the metacarpal articular base. B. A curette is shown in the metacarpal tunnel to illustrate its size and direction. C. The flexor carpi radialis graft is passed through the tunnel from volar to dorsal. D. The flexor carpi radialis graft is passed underneath and sutured to the APL, the remaining flexor carpi radialis, and back dorsally to the APL if the graft length permits. E. A 0.045 Kirschner wire is drilled from the thumb metacarpal into the trapezium to protect the ligament repair.

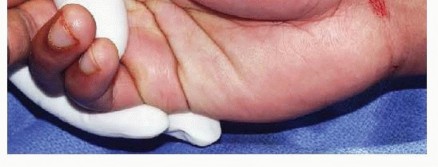
TECH FIG 4 • Final wound closure with nylon sutures.
PEARLS AND PITFALLS
|Indications ▪ In the setting of stage I or II basal joint disease and ligament laxity, the status of the articular cartilage must be carefully assessed intraoperatively. If significant cartilage damage is present, arthroplasty may be preferred.Approach ▪ Care must be taken to identify and preserve the superficial radial sensory nerve and lateral antebrachial cutaneous nerve branches to prevent neuroma formation.Flexor carpi ▪ The entire insertion of the flexor carpi radialis onto the second metacarpal radials graft base must be left intact.harvest ▪ Transect the proximal portion of the graft near the musculotendinous junction to ensure that adequate graft length will be obtained.||1. Once the graft harvest is completed, the graft should occasionally bemoistened through the remainder of the procedure to prevent desiccation and tenocyte injury.Metacarpal ▪ Start with a small-diameter tunnel. Gradually increase the diameter of the tunnel tunnel until the graft fits snugly through it.placement ▪ When creating the tunnel, be careful not to injure the insertion of the APL onto the radial base of the thumb metacarpal.Flexor carpi ▪ It is important to set the appropriate graft tension. After placing a few periosteal radialis graft sutures to hold the graft, make sure that the thumb can still be brought back into passage and a neutral position.fixation ▪ Before weaving the graft under the APL and around the intact flexor carpi radialis tendons, check an image to ensure that the CMC is adequately reduced.2. Braided synthetic suture such as Ethibond is soft and may be less palpable than stiffer suture such as Prolene.|------
POSTOPERATIVE CARE
AP, lateral, and oblique films or fluoroscopic mini C-arm views are obtained intraoperatively to evaluate CMC joint congruency and Kirschner wire placement.The thumb spica splint is left in place for 2 weeks. At 2 weeks of follow-up, the dressings are taken down, sutures are removed, and a new thumb spica splint is applied.At 5 weeks of follow-up, the Kirschner wire is removed and a removable thumb splint is used for protection. The splint can be removed for therapy, which can be started at this time.Therapy should start with active range-of-motion exercises of the wrist, thumb CMC, MCP, and interphalangeal joints. Thumb abduction, flexion, and opposition are emphasized.Strengthening exercises can be started at 2 months after surgery, and full activity without restrictions can begin at 3 months.
OUTCOMES
When performed for stage I basal joint disease, ligament reconstruction has been shown to improve pain and establish joint stability.In a number of long-term follow-up studies of over 5 years, 87% to 100% of patients demonstrated joint stability against stress testing, 29% to 67% of patients reported no pain, and 83% to 100% reported marked improvement in pain. Interestingly, only 0% to 37% of patients progressed to a higher stage ofarthritis.6,9Freedman et al6 reviewed their long-term results of 24 thumbs that underwent ligament reconstruction for stage I or II disease. After a minimum of 10 years of follow-up, 29% of patients reported no pain, 54% reported pain with strenuous activity only, and 17% of patients had pain during activitiesP.406of daily living. When tested against stress, 87% demonstrated joint stability.Simonian and Trumble14 found that 89% of patients who underwent ligament reconstruction after traumatic thumb CMC dislocation had no pain with work at 2 years of follow-up. Also, none of the patients in this treatment group had any evidence of joint instability, and no revision procedures were required.This is in contrast to 50% of patients who had residual joint instability and pain after closed reduction and percutaneous pinning. Of this treatment group, 38% required revision surgery and underwent ligament reconstruction. Twelve percent of these patients required CMC arthrodesis.
COMPLICATIONS
Residual joint instabilityResidual pain, likely due to untreated arthritis involving surrounding joint articulations, such as the scaphotrapezial jointRadial artery injurySuperficial radial nerve or lateral antebrachial cutaneous nerve injury Pin tract infection
REFERENCES
- Bettinger PC, Linscheid RL, Berger RA, et al. An anatomic study of the stabilizing ligaments of the trapezium and trapeziometacarpal joint. J Hand Surg Am 1999;24(4):786-798.
- Birman MV, Danoff JR, Yemul KS, et al. Dorsoradial ligament imbrication for thumb carpometacarpal joint instability. Tech Hand Up Extrem Surg 2014;18(2):66-71. doi:10.1097/BTH.0000000000000035.
- Eaton RG, Glickel SZ, Littler JW. Tendon interposition arthroplasty for degenerative arthritis of the trapeziometacarpal joint of the thumb. J Hand Surg Am 1985;10(5):645-654.
- Eaton RG, Littler JW. Ligament reconstruction for the painful thumb carpometacarpal joint. J Bone Joint Surg Am 1973;55(8):1655-1666.
- Edmunds JO. Traumatic dislocations and instability of the trapeziometacarpal joint of the thumb. Hand Clin 2006;22:365-392.
- Freedman DM, Eaton RG, Glickel SZ. Long-term results of volar ligament reconstruction for symptomatic basal joint laxity. J Hand Surg Am 2000;25:297-304.
- Glickel SZ, Gupta S. Ligament reconstruction. Hand Clin 2006;22: 143-151.
- Imaeda T, An KN, Cooney WP III. Functional anatomy and biomechanics of the thumb. Hand Clin 1992;8:9-15.
- Lane LB, Eaton RG. Ligament reconstruction for the painful “prearthritic” thumb carpometacarpal joint. Clin Orthop Relat Res 1987;(220):52-57.
- Lin JD, Karl JW, Strauch RJ. Trapeziometacarpal joint stability: the evolving importance of the dorsal ligaments. Clin Orthop Relat Res 2014;472:1138-1145.
- Pellegrini VD Jr. Osteoarthritis of the trapeziometacarpal joint: the pathophysiology of articular cartilage degeneration. I. Anatomy and pathology of the aging joint. J Hand Surg Am 1991;16:967-974.
- Pellegrini VD Jr. Pathomechanics of the thumb trapeziometacarpal joint. Hand Clin 2001;17:175-184.
- Rayan G, Do V. Dorsoradial capsulodesis for trapeziometacarpal joint instability. J Hand Surg Am 2013;38:382-387.
- Simonian PT, Trumble TE. Traumatic dislocation of the thumb carpometacarpal joint: early ligamentous reconstruction versus closed reduction and pinning. J Hand Surg Am 1996;21:802-806.
- Strauch RJ, Behrman MJ, Rosenwasser MP. Acute dislocation of the carpometacarpal joint of the thumb: an anatomic and cadaver study. J Hand Surg Am 1994;19:93-98.
- Swigart CR, Eaton RG, Glickel SZ, et al. Splinting in the treatment of arthritis of the first carpometacarpal joint. J Hand Surg Am 1999;24:86-91.
- Tomaino MM, King J, Leit M. Thumb basal joint arthritis. In: Green DP, ed. Green's Operative Hand Surgery, ed 5. Philadelphia: Elsevier/Churchill Livingstone, 2005:461-485.
- Van Brenk B, Richards RR, Mackay MB, et al. A biomechanical assessment of ligaments preventing dorsoradial subluxation of the trapeziometacarpal joint. J Hand Surg Am 1998;23:607-611.
