INTRODUCTION TO LESSER TOE ABNORMALITIES
Deformities of the lesser toes represent a complex spectrum of biomechanical failures, most notably driven by metatarsophalangeal (MTP) joint instability. Historically underappreciated, this condition has emerged as a well-recognized and frequently encountered clinical entity in orthopedic foot and ankle surgery. The pathology ranges in severity from acute, localized synovitis of the MTP joint to chronic, rigid deformities, including hammer toe, claw toe, and the multi-planar crossover toe deformity.
Successful management of these conditions requires a profound understanding of forefoot kinematics, intrinsic and extrinsic muscle balance, and the static ligamentous restraints that govern MTP joint stability. This comprehensive guide provides a postgraduate-level analysis of the etiology, biomechanics, clinical diagnosis, and step-by-step surgical management of lesser toe MTP joint instability.
ETIOLOGY AND PATHOGENESIS
The etiology of MTP joint instability is multifactorial, encompassing anatomic predispositions, biomechanical overload, and systemic factors. The second MTP joint is overwhelmingly the most common site of pathology.
Epidemiologically, lesser toe deformities are predominantly observed in women over the age of 50. The chronic use of constrictive, high-heeled footwear forces the MTP joints into prolonged hyperextension, placing immense strain on the plantar plate and collateral ligaments. Additionally, athletes subjected to repetitive hyperextension of the toes (e.g., dancers, sprinters) are at a high risk for chronic overuse injuries and microtrauma to the stabilizing structures.
Associative Factors and the Crossover Toe Deformity
Coughlin’s extensive review of crossover toe deformities—which invariably involve a significant element of MTP synovitis and capsular attenuation—identified a classic triad of associative factors:
1. Female gender, specifically older than 50 years of age.
2. The presence of hallux valgus.
3. Degenerative changes within the first metatarsophalangeal joint.
While hallux valgus is frequently associated with second MTP joint instability, it is critical to understand that the instability is rarely caused by direct mechanical pressure from the deviated hallux. Instead, the instability is primarily driven by attritional changes in the lateral collateral ligament, the joint capsule, and the plantar plate. These degenerative changes are the sequelae of chronic synovitis and altered forefoot loading.
The Metatarsal Length Debate
A long-standing debate in foot and ankle biomechanics centers on the role of an excessively long second metatarsal in the genesis of MTP instability and synovitis.
Clinical Pearl: The correlation between second metatarsal length and MTP pathology is highly dependent on the radiographic measurement technique utilized. Treatment decisions regarding metatarsal shortening osteotomies must account for this variability.
The traditional technique for measuring second metatarsal length, as described by Morton, involves drawing a reference line across the articular surfaces of the first and third metatarsals.

Conversely, the Hardy and Clapham method utilizes a different geometric analysis, relying on the longitudinal axis of the second metatarsal and its relationship to the first metatarsal, yielding a distinctly different assessment of relative length.

Bhutta et al. demonstrated that the perceived correlation between a "long" second metatarsal and MTP pathology fluctuates based on the chosen measurement method. This is not merely an academic distinction; it directly dictates surgical decision-making, specifically whether a Weil osteotomy or other metatarsal shortening procedure is indicated to decompress the joint.
Alternative Etiologies
Beyond biomechanical overload, other etiologies of MTP instability include:
* Systemic Arthropathies: Rheumatoid arthritis and seronegative spondyloarthropathies cause aggressive, erosive synovitis that rapidly destroys the plantar plate and collateral ligaments.
* Neuromuscular Disease: Conditions such as Charcot-Marie-Tooth disease lead to intrinsic minus foot deformities, causing profound muscular imbalance and secondary MTP dislocation.
* Acute Trauma: High-energy axial loading or forced hyperextension can cause acute, traumatic disruptions of the plantar plate and collateral ligaments, often termed "turf toe" of the lesser digits.
ANATOMY AND BIOMECHANICS
A masterful grasp of the second MTP joint anatomy is non-negotiable for the operating surgeon. Normal toe position is dictated by a delicate equilibrium between dynamic musculotendinous forces and static ligamentous restraints.
Dynamic Restraints
The extrinsic and intrinsic musculature govern the dynamic stability of the MTP joint.
The Extensor Mechanism:
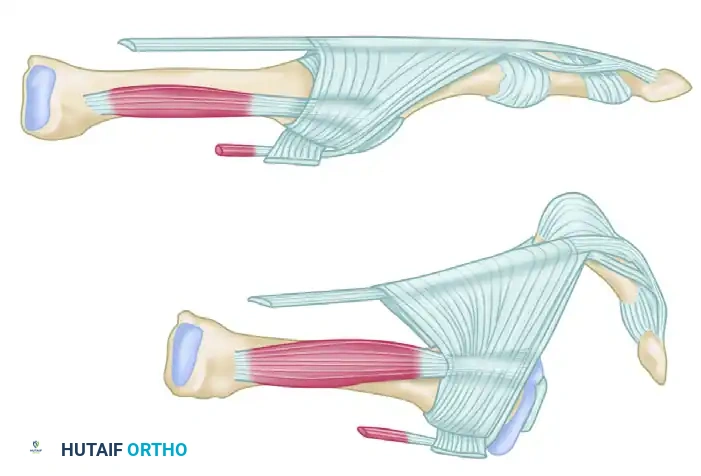
The most powerful extension force on the MTP joint is delivered by the extensor digitorum longus (EDL) tendon. The EDL extends the MTP joint via a fibroaponeurotic sling (the extensor hood) that traverses plantarly to attach to the plantar plate and the joint capsule, effectively suspending the proximal phalanx.
Crucially, the EDL tendon can only extend the interphalangeal (IP) joints if the MTP joint is held in a neutral or flexed position. If the MTP joint is chronically locked in an extended position (e.g., due to high-heeled shoes or capsular contracture), the EDL loses its mechanical advantage at the IP joints and becomes a pure, unmitigated deforming force, driving further dorsal subluxation of the MTP joint.
The Intrinsic Musculature:
Flexion of the MTP joint is primarily the function of the intrinsic muscles. The second toe possesses a unique anatomical configuration: it has two dorsal interossei and zero plantar interossei.
Under normal physiological conditions, the axis of pull of these intrinsic muscles is located plantar to the center of rotation of the MTP joint, allowing them to act as effective plantar flexors. However, as the MTP joint becomes chronically hyperextended, the line of action of these tendons migrates dorsal to the center of rotation.
Biomechanics Pitfall: Once the intrinsic tendons subluxate dorsal to the MTP joint's center of rotation, they undergo a paradoxical functional shift. They cease to be plantar flexors and instead become powerful deforming forces that exacerbate dorsal subluxation and dislocation.
The Lumbrical Muscle:
The lumbrical muscle to the second toe is located on the medial side of the joint. It normally passes plantar to the deep transverse intermetatarsal ligament, acting as a plantar flexor of the MTP joint and an extensor of the IP joints. In the setting of chronic MTP extension, the lumbrical becomes mechanically ineffective as a plantar flexor. Furthermore, because it acts as an unopposed adductor, its medial pull contributes significantly to the medial deviation seen in crossover toe deformities.
Static Restraints
The primary static restraints preventing dorsal and varus/valgus instability are the collateral ligament complex and the plantar plate.
The plantar plate is a robust, fibrocartilaginous structure that originates from the metatarsal neck and inserts firmly into the base of the proximal phalanx. It is the primary stabilizer against dorsal translation of the proximal phalanx. Chronic irritation, repetitive hyperextension, and subsequent synovitis lead to joint effusion. This inflammatory milieu causes attritional degeneration, progressive lengthening, and eventual macroscopic rupture of the plantar plate and the lateral collateral ligament, culminating in multi-planar instability.
CLINICAL EVALUATION AND DIAGNOSIS
The diagnosis of MTP joint instability is primarily clinical, demanding a meticulous history and a structured physical examination.
Patient History
Patients typically present with an insidious onset of pain localized to the plantar aspect of the forefoot, often described as feeling like "walking on a marble." Initially, the pain is strictly mechanically mediated, occurring only during weight-bearing activities. As the plantar plate attenuates and the joint subluxates, the inflammatory cycle worsens, and patients may begin to experience intractable pain even at rest.
Physical Examination
Visual inspection may or may not reveal a frank hammer toe or crossover deformity in the early stages. However, subtle signs of joint effusion are usually present.
Key Inspection Findings:
* Loss of Contour: Swelling of the MTP joint often manifests as a loss of the normal, defined contour of the long extensor tendon when compared to adjacent, asymptomatic toes.
* Plantar Callus: As the proximal phalanx subluxates dorsally, the metatarsal head is driven plantarly, leading to a prominent, painful plantar keratosis (callus) directly beneath the metatarsal head.
Palpation and Provocative Testing:
A palpable effusion is frequently present. Point tenderness is classically elicited on the dorsofibular aspect of the joint (indicating lateral collateral ligament attenuation) or directly over the plantar plate, just proximal to the metatarsal head.
The most critical and consistent physical finding in MTP instability is a positive Lachman Test (Drawer Sign) of the MTP joint. This test assesses the integrity of the plantar plate and collateral ligaments.
To perform the Lachman test:
1. The examiner stabilizes the metatarsal head securely with one hand.
2. The other hand grasps the base of the proximal phalanx.
3. A pure dorsal translation force is applied to the proximal phalanx while maintaining the joint in a neutral alignment.

(Starting position for the Lachman test, demonstrating stabilization of the metatarsal and grasping of the proximal phalanx.)

(Positive Lachman test demonstrating significant dorsal translation and subluxation of the proximal phalanx, indicative of plantar plate incompetence.)

(Alternative view: Starting position for examination of MTP joint stability.)

(Alternative view: Positive test with visible and palpable dorsal subluxation of the joint.)
A positive test is characterized by excessive dorsal translation, a "mushy" or absent endpoint, and reproduction of the patient's pain. Range of motion testing will typically reveal limited plantar flexion compared to the contralateral, healthy toe, secondary to dorsal contracture.
Imaging Modalities
While the diagnosis is primarily clinical, imaging is essential for surgical planning.
* Weight-Bearing Radiographs: AP, lateral, and oblique views are mandatory. They allow assessment of metatarsal length, joint congruity, the presence of degenerative joint disease, and the degree of dorsal/medial/lateral subluxation.
* Magnetic Resonance Imaging (MRI): Advanced imaging using a small receiver coil (as described by Yao et al.) is highly sensitive and specific for evaluating the integrity of the plantar plate. MRI can differentiate between interstitial tearing, complete rupture, and isolated synovitis, aiding in the decision between conservative management and surgical repair.
SURGICAL MANAGEMENT
When conservative measures (e.g., taping, orthotics with metatarsal pads, stiff-soled shoes, NSAIDs) fail to provide relief, surgical intervention is indicated. The goal of surgery is to restore joint congruity, re-establish dynamic muscle balance, and repair static restraints.
Indications for Surgery
- Intractable pain at the MTP joint unresponsive to 3-6 months of conservative care.
- Progressive deformity (crossover toe, severe hammer toe) interfering with shoe wear.
- Frank dislocation of the MTP joint.
- MRI-confirmed high-grade or complete rupture of the plantar plate in a symptomatic patient.
Patient Positioning and Anesthesia
The patient is placed in the supine position. A regional ankle block or popliteal block is highly recommended for postoperative pain control, supplemented with monitored anesthesia care (MAC) or general anesthesia. A calf or ankle tourniquet is applied to ensure a bloodless surgical field.
Step-by-Step Surgical Approach
Surgical correction must be tailored to the specific pathology, often requiring a stepwise release of contracted structures followed by skeletal realignment and ligamentous repair.
Step 1: Soft Tissue Release (Extensor Lengthening and Capsulotomy)
- Incision: A dorsal longitudinal incision is made centered over the second MTP joint, extending from the distal metatarsal shaft to the mid-proximal phalanx.
- Dissection: Full-thickness flaps are elevated to protect the dorsal cutaneous nerves.
- Extensor Tendon Management: The EDL tendon is identified. If a severe extension contracture is present, a Z-lengthening of the EDL is performed. The extensor digitorum brevis (EDB) is typically tenotomized.
- Capsulotomy: A dorsal capsulotomy is performed. If the toe is deviated medially (crossover), a thorough release of the medial capsule and the medial lumbrical tendon is executed to correct the transverse plane deformity.
Step 2: Joint Decompression (The Weil Osteotomy)
If the joint remains subluxated or if the second metatarsal is excessively long, a Weil osteotomy is the gold standard for joint decompression.
1. Exposure: The collateral ligaments are released off the metatarsal head to allow full exposure of the articular surface.
2. Osteotomy: Using a sagittal saw, an osteotomy is made parallel to the plantar aspect of the foot. The cut begins in the dorsal half of the metatarsal head and exits proximally in the plantar metatarsal shaft.
3. Translation: The capital fragment is translated proximally (typically 2 to 5 mm) to decompress the joint and relax the intrinsic musculature.
4. Fixation: The osteotomy is provisionally pinned and then rigidly fixed with one or two small fragment screws (e.g., 2.0 mm or 2.7 mm) directed from dorsal-proximal to plantar-distal.
5. Resection: The overhanging dorsal bony prominence of the proximal fragment is resected flush with the metatarsal head to prevent dorsal impingement.
Surgical Warning: Ensure the Weil osteotomy cut is strictly parallel to the plantar weight-bearing surface. An excessively steep cut will result in plantar displacement of the metatarsal head, leading to severe postoperative transfer metatarsalgia.
Step 3: Plantar Plate Repair
With the joint decompressed, attention is turned to the plantar plate.
1. Visualization: A joint distractor or a McGlamry elevator is used to expose the plantar aspect of the metatarsal head and the torn plantar plate.
2. Preparation: The torn edge of the plantar plate is debrided to healthy, bleeding tissue. The base of the proximal phalanx is decorticated to create a bleeding bone bed for healing.
3. Suture Passage: Using a specialized suture passing device (e.g., Viper or Mini-Scorpion), heavy non-absorbable sutures (e.g., #0 or 2-0 FiberWire) are passed through the plantar plate in a mattress fashion.
4. Bone Tunnels: Two drill holes are made from dorsal to plantar through the base of the proximal phalanx.
5. Tensioning and Tying: The suture limbs are passed through the bone tunnels. The toe is held in 10 to 15 degrees of plantar flexion, and the sutures are tied over the dorsal bony bridge of the proximal phalanx, securely advancing the plantar plate into the bony footprint.
Step 4: K-Wire Stabilization
To protect the repair, a 0.045-inch or 0.062-inch Kirschner wire is driven antegrade through the proximal phalanx and then retrograde across the MTP joint into the metatarsal shaft, holding the joint in neutral alignment and slight plantar flexion.
Postoperative Protocol
- Weeks 0-2: The patient is placed in a bulky, compressive dressing and a rigid postoperative shoe. Weight-bearing is strictly limited to the heel. Elevation is critical to minimize edema.
- Weeks 2-4: Sutures are removed. The K-wire remains in place. The patient may begin flat-foot weight-bearing in a stiff-soled surgical shoe.
- Weeks 4-6: The K-wire is removed in the clinic. The patient is transitioned to a supportive athletic shoe. Aggressive physical therapy is initiated, focusing on active and passive plantar flexion of the MTP joint to prevent dorsal contracture.
- Weeks 6-12: Progressive return to normal activities and footwear. Taping the toe in slight plantar flexion (plantar flexion strapping) is continued for up to 3 months to protect the healing plantar plate.
COMPLICATIONS AND PITFALLS
Even with meticulous surgical technique, complications can arise:
* Floating Toe Deformity: The most common complication following a Weil osteotomy. It occurs due to the dorsal shift of the intrinsic muscle axis. Concomitant plantar plate repair and aggressive postoperative plantar flexion exercises mitigate this risk.
* Transfer Metatarsalgia: Caused by excessive shortening or plantar displacement of the metatarsal head during osteotomy.
* Recurrent Deformity: Often due to failure to recognize and release a contracted lumbrical or failure to adequately repair the lateral collateral ligament complex.
* Stiffness: MTP joint stiffness is nearly universal postoperatively. Patients must be counseled preoperatively that the goal is a stable, pain-free joint, not necessarily a joint with normal physiological range of motion.
