DEFINITION
Extrinsic elbow contracture refers to elbow stiffness secondary to fibrosis, thickening, and, occasionally, ossification of the elbow capsule and periarticular soft tissues. In contrast to intrinsic contracture, the articular surface is either uninvolved or minimally involved, without the presence of intra-articular adhesions or articular cartilage destruction.Although a distinction is made between extrinsic and intrinsic causes of contracture, these entities often overlap.
ANATOMY
The elbow is a compound uniaxial synovial joint comprising three highly congruous articulations.The ulnohumeral joint is a ginglymus, or hinge, joint. The radiocapitellar and proximal radioulnar joints are gliding joints.All three articulations exist within a single capsule and are further stabilized by the proximity of the articular surface and capsule to the intracapsular ligaments and overlying extracapsular musculature.
PATHOGENESIS
The propensity for elbow stiffness after even trivial elbow trauma is well recognized. After even seemingly trivial injuries, the capsule can undergo structural and biochemical alterations leading to thickening, decreased compliance, and loss of motion.Causes of extrinsic elbow contracture include capsular contracture, damage to and fibrosis of the flexor-extensor muscular origins, collateral ligament scarring, heterotopic bone, and skin contracture.Prolonged immobilization after trauma may be a separate risk factor for the development of stiffness.
NATURAL HISTORY
Little consensus exists regarding the natural history of capsular contracture. It is felt that appropriate recognition and treatment of acute elbow injuries, avoidance of prolonged immobilization, and early active range of motion may limit the severity of posttraumatic extrinsic contracture.Patients typically do not tolerate elbow stiffness well because adjacent joints do not provide adequate compensatory motion.Morrey10 showed that the performance of most activities of daily living requires a functional arc of motion from 30 to 130 degrees.Vasen and colleagues11 have demonstrated that volunteers with uninjured elbows may adapt to a functional arc of motion from 70 to 120 degrees to perform 12 tasks of daily living.Patients typically request treatment for elbow contracture when loss of extension approaches 40 degrees and flexion does not exceed 120 degrees.Patients who do not improve with a concerted effort at nonoperative treatment often require surgical release.Stiffness of the elbow typically is incited by soft tissue trauma, hemarthrosis, and the patient's response to pain. Elbow trauma may cause tearing and contusion of the periarticular soft tissues. The patient typically holds the injured elbow in a flexed position to reduce pain. A fibrous tissue response then ensues within the hematoma and damaged muscular tissues. This fibrous tissue may ossify. In addition, overly aggressive therapy may further exacerbate these injuries, potentiating the cycle of pain, swelling, and limitation in motion that leads ultimately to frank contracture.Collateral ligament injury may contribute to contracture. Primary fibrosis may develop within the collateral ligaments because of the initial injury. Alternatively, secondary fibrosis may result from immobilization and scar formation.Significant injury to the anterior joint capsule and the overlying brachialis muscle may also result in capsular hypertrophy and fibrotic reaction contributing to ankylosis. This is particularly common in association with fracture-dislocations of the elbow.
PATIENT HISTORY AND PHYSICAL FINDINGS
The cause of contracture should generally be easily elucidated from the history. Particular notation should be made of concomitant injuries, including closed head injury or associated burn injury.The duration and possible progression of symptoms should be noted.The impact of the contracture on the patient's upper extremity function and any limitations in activities of daily living should be noted.Any previous treatment for contracture should be elucidated. This should include the appropriateness, duration, and results of prior physical therapy, splinting, intra-articular injections, and surgeries.For patients with prior elbow surgery, the presence and type of any residual internal fixation devices should be noted. In addition, attention should be paid to any remote history of elbow infection.Physical examination should include a general physical examination as well as a detailed examination of the involved extremity.Attention must be paid to the examination of the skin and soft tissue envelope about the elbow, with notation made of prior incisions, skin grafts, flaps, or areas of wound breakdown.P.1183Elbow motion should be measured with a goniometer and active and passive motion should be compared.Notation should be made whether motion improves with the forearm in full pronation, which may suggest posterolateral rotatory instability.Although rare, symptomatic incompetence of the ulnar collateral ligament may elucidated by examination.Strength of the involved limb should be assessed, as a joint without adequate strength is unlikely to maintain motion after release.Because many posttraumatic and inflammatory contractures about the elbow are associated with ulnar nerve symptoms, a careful neurologic examination should be performed. A positive Tinel test over the cubital tunnelas well as a positive elbow flexion test should increase the suspicion for concomitant ulnar nerve pathology.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Anteroposterior (AP) and lateral radiographs are often all that is needed for preoperative planning (FIG 1).Cross-sectional imaging with computed tomography is helpful in visualizing the articular surfaces, particularly after fracture.We advocate the use of computed tomography for preoperative planning in cases of moderate to severe heterotopic ossification.Extracapsular contracture is typically not painful through the remaining arc of motion and is not painful at rest. If pain is a significant component of the patient's symptoms, serologic workup for infection, including a complete blood count, erythrocyte sedimentation rate, and C-reactive protein, is indicated.
DIFFERENTIAL DIAGNOSIS
Conversion disorder InfectionInflammatory arthropathy Intracapsular contracture
NONOPERATIVE MANAGEMENT
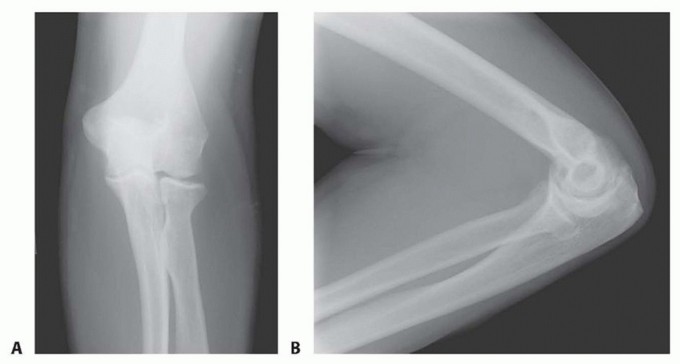
FIG 1 • Routine preoperative AP (A) and lateral (B) radiographs are obtained in all cases. Contracture may occur after subtle injury. This patient developed stiffness after nonoperative treatment of a nondisplaced radial neck fracture.A short-term oral prednisone taper can be very effective in difficult cases. In addition, one can consider an intra-articular cortisone injection to decrease inflammation and joint synovitis.Rarely, when patients exhibit guarding and involuntary co-contraction, biofeedback may be a helpful adjunct. Dynamic splints, which apply a constant tension to the soft tissues, may be helpful.5These braces improve range of motion through soft tissue creep. They tend to be more painful to wear andmay cause unwanted inflammation.Patient-adjusted static braces appear to be more effective. These braces use the principle of passive progressive stretch, allowing for stress relaxation of the soft tissues. They are applied for much shorter periods of time and are better tolerated by patients.
SURGICAL MANAGEMENT
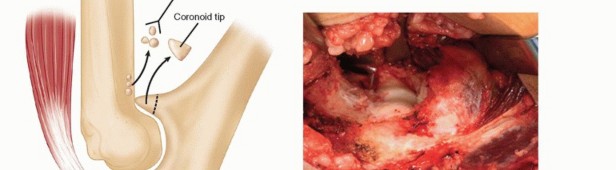
To improve elbow flexion, one must release any soft tissue structures posteriorly that might be tethering the joint. These include the posterior joint capsule (including the posterior bundle of the ulnar collateral ligament) and the triceps muscle and tendon, which can become adherent to the humerus.1,6,8,9Any bony or soft tissue impingement also must be removed anteriorly, including osteophytes off the coronoid process and any bony or soft tissue overgrowth in both the coronoid and radial fossae.There must be a concavity above the humeral trochlea to accept both the coronoid centrally and the radial head laterally for full flexion to occur.Similarly, to improve elbow extension, posterior impingement must be removed between the olecranon tip and the olecranon fossa.Anteriorly, any tethering soft tissues must be released, namely the anterior joint capsule and any adhesions between the brachialis and the humerus.4,7
PREOPERATIVE PLANNING
All radiographic studies should be reviewed.The presence and type of any retained implants is noted.Range-of-motion and pivot shift testing is performed under anesthesia as well as under live fluoroscopy.P.1184
POSITIONING
Patients are positioned supine with the arm on a hand table.The patient's torso is brought to the edge of the operating table to ensure adequate elbow exposure for fluoroscopic imaging.A towel bump may be placed under the medial elbow.
APPROACH
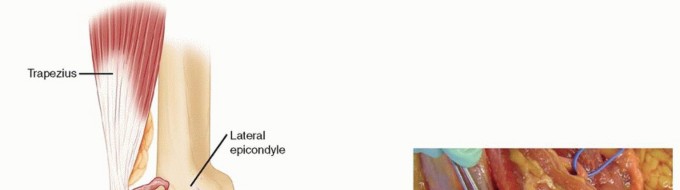
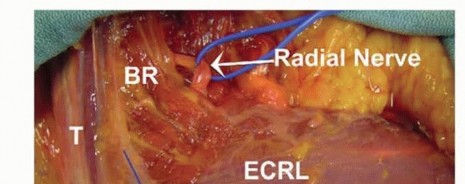
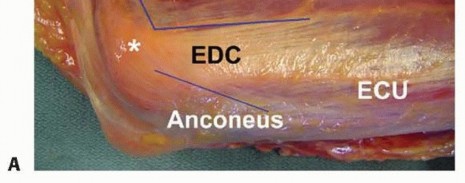
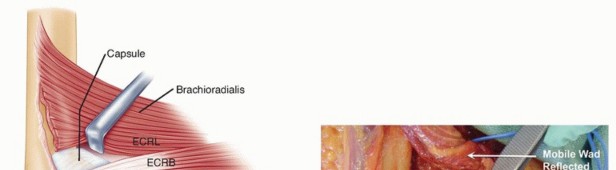
A direct posterior skin incision or a lateral incision is used.A direct posterior incision has been criticized for an increased propensity toward postoperative seromaformation.It has the advantage of being a utilitarian incision that allows access to the medial and lateral sides simultaneously.Advantages to the lateral exposure include its simplicity, less extensor and flexor-pronator disruption, and access to all three joint articulations.The main disadvantage of the lateral exposure is the inability to address the ulnar nerve and posterior bundle of the ulnar collateral ligament when indicated.The deep interval for exposure of the anterior capsule lies between the extensor carpi radialis longus (ECRL) proximally and the extensor carpi radialis brevis (ECRB) distally. Posterior access is achieved between the triceps and the humerus.
TECHNIQUE
SURGICAL APPROACH
POSTERIOR RELEASE


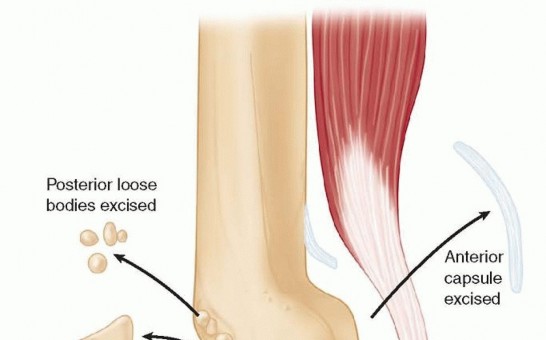
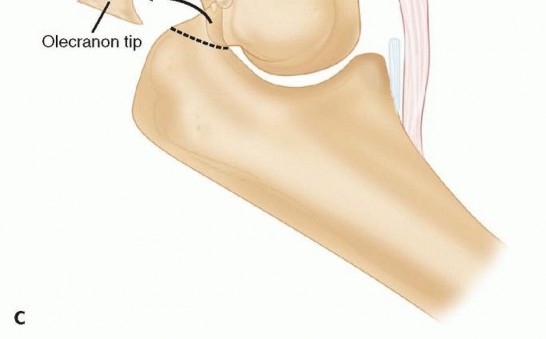
TECH FIG 1 •(continued)C. Visualization of the posterior compartment permits débridement of the posterior joint, including removing impinging tissue of osteophytes in the olecranon fossa and the tip of the olecranon.
ANTERIOR RELEASE
PEARLS AND PITFALLS
Indications ▪ The importance of prolonged postoperative rehabilitation cannot be stressed enough. A program of active and passive range of motion, weighted elbow stretches with wrist weights, formal therapy, and patient-adjusted elbow bracing is common for 3-6 months after surgery.1. Postoperative gains may easily be lost in the patient who is not fully committed to rehabilitation or who does not have access to regular supervised therapy.Ulnar nerve ▪ Patients with preoperative signs and symptoms of ulnar nerve irritability should undergo neurolysis and transposition of the ulnar nerve. Although no strict guidelines exist, patients with preoperative flexion less than 100 degrees generally undergo concurrent ulnar nerve release even in the absence of preoperative symptoms.2. Care should be observed when manipulating the elbow following all soft tissue releases from the lateral approach to regain flexion. Residual limitations in flexion are likely due to contracture of the posterior bundle of the ulnar collateral ligament. Forced manipulation can cause a traction injury to the ulnar nerve.Median nerve and brachial artery1. These structures are generally well protected by the brachialis muscle. Their safety is increased if dissection proceeds in the interval between the elbow capsule and the brachialis.Radial nerve injury1. The posterior interosseous nerve may be encountered as extracapsular dissection proceeds distal to the radiocapitellar joint. Care must be taken with more distal dissection, and a firm understanding of neural anatomy is mandatory before attempting capsular release. Except in cases of significant anterolateral heterotopic ossification, we do not routinely dissect and isolate the radial nerve from proximal to distal.Iatrogenic posterolateral rotatory instability2. Instability may be induced with overly aggressive dissection about the lateral condyle. Care should be taken to stay anterior to the origin of the ECRB.
POSTOPERATIVE CARE



FIG 2 • A. Elbow continuous passive motion device. B. Patient-adjusted static elbow brace. Because the collateral ligaments are not released at surgery, no restrictions are typically placed on therapy.3Static progressive elbow bracing is begun early in the postoperative period. The brace is worn for about 30 minutes, two or three times a day. Flexion and extension are alternated based on the preoperative deficit and the early progress of the elbow (FIG 2B).Commercially available braces should be obtained preoperatively, as trying to secure them postoperatively can delay the onset of their use.A nonsteroidal anti-inflammatory agent (Indocin) is commonly prescribed as a prophylaxis against heterotopic ossification for several weeks postoperatively. This also helps to limit inflammation of the joint and soft tissues during rehabilitation.P.1188Patients are typically discharged home on postoperative day 1. Home therapy is performed daily thereafter, including active and passive exercises, continuous passive motion, weighted stretches, and patient-adjusted bracing.Progress should be closely monitored by a therapist who is familiar with the protocol. The physician must also follow these patients closely.Although the bulk of ultimate elbow motion is gained during the first 6 to 8 weeks, patients can continue to make gains in terminal flexion and extension for several months postoperatively. This is especially true forelbow flexion.Continuous passive motion is typically discontinued at 3 to 4 weeks, but bracing is continued for several months as required. As long as the patient is able to obtain full elbow flexion and extension once per day (eg, in the brace), a favorable prognosis exists with respect to the ultimate outcome if vigilance is maintained.
OUTCOMES
In appropriate patients, release of the contracted elbow can be a reliable and satisfying procedure with predictable results.We reviewed our results for 22 patents treated for posttraumatic elbow stiffness using a soft tissue release of the elbow through a lateral approach. The average length of follow-up was 29 months.2Total elbow motion improved in all subjects. Extension increased from an average of 39 ± 10 degrees preoperatively to 8 ± 6 degrees at follow-up. Elbow flexion increased from 113 ± 18 degrees preoperatively to 137 ± 9 degrees at follow-up. Thus, total ulnohumeral joint motion increased an average of 55 degrees (P< .001).Elbow pain, as determined by visual analog scales, decreased in all patients. Elbow function, as determined by standardized scales, also significantly improved.Radiographic analysis revealed no patients with regrowth of excised osteophytes or loose bodies at follow-up.
COMPLICATIONS
Ulnar nerveThe most common complication after elbow release surgery involves the ulnar nerve. This may be related in part to improved elbow flexion after surgery, as ulnar nerve tension increases with flexion. This may precipitate symptoms in a nerve that is already subclinically compromised.Patients with preoperative signs and symptoms of ulnar nerve irritability should undergo neurolysis and transposition of the ulnar nerve.Although no strict guidelines exist, patients with preoperative flexion less than 100 degrees generally undergo concurrent ulnar nerve release even in the absence of preoperative symptoms.Median nerve and brachial arteryAlthough generally well protected by the brachialis muscle, these structures are at risk with anterior dissection. Their safety is increased if dissection proceeds in the interval between the elbow capsule and the brachialis.In addition, transient median neuritis is known to occur in our practices after release. This is likely due to stretch of the median nerve with extension of the severely contracted elbow.Radial nerve injuryThe posterior interosseous nerve may be encountered, as extracapsular dissection proceeds distal to the radiocapitellar joint.Except in cases of significant anterolateral heterotopic ossification, the radial nerve does not typically require identification.Persistent stiffnessThe importance of prolonged postoperative rehabilitation cannot be stressed enough. A program of active and passive range of motion, weighted elbow stretches with wrist weights, formal therapy, and patient-adjusted elbow bracing is common for 3 to 6 months after surgery. All of our patients meet preoperatively both with the therapists at our home institutions as well as with their local therapists.
REFERENCES
- Cohen MS, Hastings H II. Operative release for elbow contracture: the lateral collateral ligament sparing technique. Orthop Clin North Am 1999;30:133-139.
- Cohen MS, Hastings H II. Post-traumatic contracture of the elbow. Operative release using a lateral collateral sparing approach. J Bone Joint Surg Br 1998;80(5):805-812.
- Cohen MS, Hastings H II. Rotatory instability of the elbow. The anatomy and role of the lateral stabilizers. J Bone Joint Surg Am 1997;79(2):225-233.
- Gates HS III, Sullivan FL, Urbaniak JR. Anterior capsulotomy and continuous passive motion in the treatment post-traumatic flexion contracture of the elbow. J Bone Joint Surg Am 1992;74(8): 1229-1234.
- Green DP, McCoy H. Turnbuckle orthotic correction of elbow flexion contractures after acute injuries. J Bone Joint Surg Am 1979;61(7):1092-1095.
- Jupiter JB, O'Driscoll SW, Cohen MS. The assessment and management of the stiff elbow. Instr Course Lect 2003;52:93-111.
- Kasparyan NG, Hotchkiss RN. Dynamic skeletal fixation in the upper extremity. Hand Clin 1997;13:643-663.
- Mansat P, Morrey BF. The column procedure: a limited lateral approach for extrinsic contracture of the elbow. J Bone Joint Surg Am 1998;80(11):1603-1615.
- Modabber MR, Jupiter JB. Reconstruction for post-traumatic conditions of the elbow joint. J Bone Joint Surg Am 1995;77(9): 1431-1446.
- Morrey BF. Post-traumatic contracture of the elbow. Operative treatment, including distraction arthroplasty. J Bone Joint Surg Am 1990;72(4):601-618.
- Vasen AP, Lacey SH, Keith MW, et al. Functional range of motion of the elbow. J Hand Surg Am 1995;20(2):288-292.
