Introduction & Epidemiology
The lateral approach to the knee is a fundamental exposure in orthopedic surgery, providing comprehensive access to the intricate supporting structures of the lateral compartment. While medial knee pathologies, particularly valgus-induced ligamentous injuries, are statistically more prevalent, the lateral approach is indispensable for addressing a spectrum of acute and chronic conditions affecting the lateral collateral ligament (LCL), posterolateral corner (PLC), iliotibial band (ITB), biceps femoris, and lateral meniscus. Furthermore, this approach can be judiciously extended for broader intra-articular visualization of anterior and posterior structures, making it versatile for complex multi-ligamentous knee injuries and certain fracture patterns of the lateral tibial plateau or fibular head.
Understanding the epidemiology of lateral knee injuries underscores the importance of a meticulous lateral approach. Isolated LCL injuries are less common than medial collateral ligament (MCL) injuries, often occurring in varus stress traumas, contact sports, or falls. However, the PLC, a complex confluence of static and dynamic stabilizers, is frequently injured in conjunction with cruciate ligaments, particularly the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL). Combined ACL-PLC injuries represent a significant challenge, often resulting from hyperextension, varus stress, or external rotation mechanisms. Chronic instability stemming from inadequately treated lateral-sided injuries can lead to progressive articular degeneration and functional impairment. The lateral approach is thus critical for accurate diagnosis, anatomical repair, and robust reconstruction, aiming to restore knee stability and kinematics.
Surgical Anatomy & Biomechanics
A thorough understanding of the layered surgical anatomy and the intricate biomechanics of the lateral knee is paramount for safe and effective surgical intervention. The lateral compartment is defined by a complex interplay of passive stabilizers (ligaments, capsule) and dynamic stabilizers (muscles, tendons) working in concert to resist varus stress and posterolateral tibial rotation.
Superficial Layer:
*
Skin and Subcutaneous Tissue:
The initial dissection exposes the superficial fascia and subcutaneous fat. Neurovascular structures in this plane are typically minor, but care must be taken to minimize dissection of cutaneous nerves to reduce post-operative dysesthesia.
*
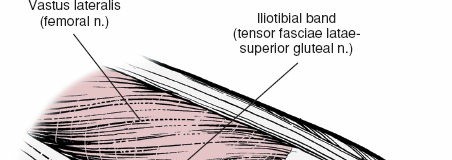
Iliotibial Band (ITB):
This fibrous aponeurosis, originating from the tensor fascia lata and gluteus maximus, courses distally to insert primarily on Gerdy's tubercle (the lateral tubercle of the tibia) and also sends fibers to the lateral patellar retinaculum and lateral femoral epicondyle. It acts as an important stabilizer against varus stress and internal tibial rotation, particularly in extension.
* The ITB can be incised longitudinally, elevated anteriorly or posteriorly, or approached through a posterior split to access deeper structures.
Middle Layer:
*
Lateral Collateral Ligament (LCL):
The primary static restraint to varus stress. It originates from the lateral femoral epicondyle, distal and posterior to the popliteus tendon origin, and inserts into the fibular head, anterior to the biceps femoris insertion. It is extra-articular and distinct from the capsule.
*
Popliteus Tendon:
Originating from the lateral femoral epicondyle, deep to the LCL, it courses inferomedially across the posterior aspect of the lateral tibial plateau, inserting onto the posterior tibia. Its musculotendinous unit actively assists in internal tibial rotation (unlocking the knee) and resists external rotation and posterior translation of the tibia.
*
Popliteofibular Ligament:
A key component of the PLC, this ligament runs from the popliteus musculotendinous junction to the fibular head, reinforcing the PLC and resisting posterolateral tibial rotation.
*
Lateral Capsule:
The fibrous capsule, though less robust than medially, contributes to joint stability.
*
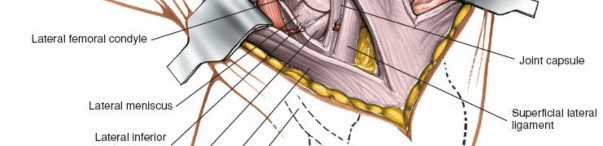
Lateral Meniscus:
The crescent-shaped fibrocartilaginous structure between the femoral condyle and tibial plateau. Its peripheral attachments are crucial, and root tears or ramp lesions can significantly compromise knee stability.
Deep Layer (Posterolateral Corner - PLC):
The PLC is not a single structure but a complex functional unit comprising the LCL, popliteus musculotendinous unit, popliteofibular ligament, lateral gastrocnemius tendon, fabellofibular ligament (when present), and posterolateral capsule. These structures synergistically resist external tibial rotation and varus angulation, particularly at higher flexion angles.
Neurovascular Structures:
*
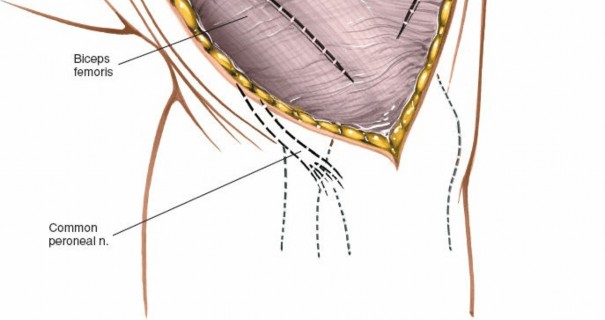
Common Peroneal Nerve (CPN):
This is the most critical neurovascular structure at risk during lateral knee surgery. It courses from the popliteal fossa, deep to the biceps femoris muscle, around the fibular neck, where it divides into its superficial and deep branches. It lies immediately posterior to the biceps femoris tendon insertion on the fibular head. Meticulous identification and protection are paramount.
* The superficial peroneal nerve provides sensation to the dorsum of the foot, while the deep peroneal nerve innervates the anterior compartment muscles of the leg (dorsiflexion) and provides sensation to the first web space. Injury can result in foot drop and sensory deficits.
Biomechanics:
*
Varus Stability:
Primarily conferred by the LCL, ITB, and lateral capsule.
*
Posterolateral Rotatory Stability (PLRI):
A complex interaction, primarily resisted by the popliteus tendon, popliteofibular ligament, LCL, and posterior-lateral capsule. Loss of PLRI results in increased external tibial rotation, especially at 30 degrees of knee flexion, and can lead to pivot-shift phenomenon in ACL-deficient knees.
Indications & Contraindications
The lateral approach to the knee is indicated for a range of pathologies, primarily involving the lateral ligamentous complex and its associated structures.
Indications
- Acute Lateral Collateral Ligament (LCL) Rupture: Especially grade III tears (complete rupture) or avulsion fractures.
- Chronic LCL Insufficiency: Leading to symptomatic varus instability.
- Acute Posterolateral Corner (PLC) Injury: Isolated or, more commonly, combined with cruciate ligament (ACL/PCL) ruptures. Often requires anatomical repair or reconstruction.
- Chronic PLC Instability: Symptomatic posterolateral rotatory instability.
- Avulsion Fractures: Of the fibular head (e.g., biceps femoris or LCL avulsions), lateral femoral epicondyle, or Gerdy's tubercle.
- Complex Lateral Tibial Plateau Fractures: Providing direct visualization and access for reduction and internal fixation.
- Iliotibial Band (ITB) Procedures: Such as ITB friction syndrome release (though often amenable to smaller approaches), ITB tenodesis for patellar instability (e.g., lateral retinacular lengthening), or reconstruction for chronic lateral instability.
- Lateral Meniscus Repair: When combined with lateral ligamentous reconstruction, or for complex peripheral tears.
- Tumors or Biopsies: Of lateral knee soft tissues or bone.
- Excision of Osteophytes: In lateral compartment osteoarthritis.
- Revision Surgery: For failed previous lateral knee procedures.
Contraindications
Absolute Contraindications:
* Active local or systemic infection.
* Severe vascular compromise of the limb.
* Compromised skin integrity (e.g., burns, severe cellulitis) in the surgical field.
Relative Contraindications:
* Significant medical comorbidities precluding safe anesthesia and surgery.
* Extensive scarring from previous surgeries that may compromise skin viability or obscure critical anatomical planes.
* Extremely limited surgical exposure required for specific procedures, where a smaller, more targeted approach might be less morbid.
* Uncontrolled coagulopathy.
Operative vs. Non-Operative Indications
The decision between operative and non-operative management for lateral knee injuries is complex and depends on the severity of the injury, associated pathologies, patient activity level, and functional demands.
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| LCL Injury |
*
Grade III Tears:
Complete tears, especially mid-substance or avulsions.
Combined LCL-Cruciate/PLC Injuries: Necessitates surgical stabilization of all involved structures. Chronic Symptomatic Varus Instability: Persistent functional instability despite conservative measures. |
*
Grade I & II Sprains:
Mild to moderate partial tears with minimal laxity.
Asymptomatic or Mildly Symptomatic Grade III Tears: In low-demand patients or those unwilling/unfit for surgery, with bracing and physical therapy. Isolated LCL Injuries: Often treated with immobilization and progressive rehabilitation. |
| PLC Injury |
*
Acute Grade III Tears:
Particularly in conjunction with ACL/PCL tears.
Fibular Head Avulsion Fractures: Requiring fixation. Chronic Symptomatic Posterolateral Rotatory Instability: Despite extensive physical therapy. Multi-ligamentous Knee Injuries: * Where PLC disruption contributes significantly to instability. |
*
Grade I & II Sprains:
Mild to moderate injury without significant instability.
Asymptomatic Grade III Tears: In select low-demand individuals, though this is less common given the functional impact. Elderly or Medically Unfit Patients: With functional bracing and activity modification. |
| Tibial Plateau Fracture |
*
Displaced Lateral Plateau Fractures:
Requiring open reduction and internal fixation (ORIF) to restore joint congruity and stability.
Depressed Articular Fragments: Requiring elevation and bone grafting. Fractures with Ligamentous Instability: When associated with significant LCL/PLC tears. |
*
Nondisplaced or Minimally Displaced Fractures:
Managed with cast immobilization, bracing, and non-weight-bearing.
Stable Fractures: * With minimal articular step-off or gap. |
| ITB Pathology |
*
Recalcitrant ITB Friction Syndrome:
After failed extensive non-operative management.
ITB Tenodesis: * For patellar instability or as part of complex knee reconstruction. |
* ITB Friction Syndrome: Initial management typically involves rest, activity modification, stretching, physical therapy, NSAIDs, and corticosteroid injections. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and optimal patient positioning are critical for successful outcomes and minimizing complications with the lateral approach to the knee.
Pre-Operative Planning
- Clinical Assessment: A thorough history and physical examination are paramount, focusing on the mechanism of injury, associated symptoms, and evaluation of all knee ligamentous structures (varus/valgus stress testing at 0 and 30 degrees, Lachman, posterior drawer, dial test for PLRI). Pre-existing neurological deficits, particularly involving the common peroneal nerve, must be documented.
-
Imaging:
- Plain Radiographs: AP, lateral, and oblique views to assess for fractures (e.g., fibular head avulsion, Segond fracture, tibial plateau fractures), osteophytes, or degenerative changes. Stress radiographs (varus stress at 0 and 30 degrees) can objectively quantify LCL and PLC laxity.
- Magnetic Resonance Imaging (MRI): The gold standard for soft tissue evaluation, delineating ligamentous ruptures (LCL, PLC, cruciate ligaments), meniscal pathology, and chondral lesions. It provides crucial information on the extent and location of injuries.
- Computed Tomography (CT) Scan: Indicated for complex tibial plateau fractures to assess fracture morphology, articular depression, and comminution, aiding in surgical templating.
- Surgical Templating: For reconstructions, consider graft choice (autograft: hamstring, quadriceps, achilles; allograft: tibialis anterior, achilles), tunnel placement, and fixation methods. For fractures, template plate and screw sizes and locations.
- Equipment and Instrumentation: Ensure availability of appropriate retractors (Hohmann, army-navy), dissecting instruments, arthroscopy equipment (if combined procedure), drills, guidewires, screw sets, suture anchors, and reconstruction kits.
- Tourniquet: A pneumatic tourniquet should be readily available and tested.
- Consent: Comprehensive discussion with the patient regarding the procedure, potential benefits, risks (especially common peroneal nerve injury, infection, stiffness, re-rupture), and expected post-operative course.
Patient Positioning
The patient is typically placed supine on the operating table.
- Limb Preparation: The entire limb, from the iliac crest to the toes, is prepped and draped in a sterile fashion.
-
Sandbag Placement:
A sandbag or bolster is placed under the ipsilateral buttock. This maneuver internally rotates the entire leg, effectively exposing the lateral aspect of the knee and making the fibular head and common peroneal nerve more accessible and identifiable.

- Knee Flexion: The knee is often flexed to approximately 90 degrees, either supported by a specialized leg holder or allowing the foot to rest on the table or a footrest. This position allows for optimal visualization and manipulation of the lateral structures.
- Exsanguination and Tourniquet Inflation: The limb is exsanguinated by elevating it for 3-5 minutes, or by applying a soft rubber bandage (Esmarch). A pneumatic tourniquet is then inflated to a supra-systolic pressure (typically 250-300 mmHg, adjusted for patient's blood pressure) to create a bloodless field, which is crucial for identifying delicate structures like the common peroneal nerve. The tourniquet time should be carefully monitored.
Detailed Surgical Approach / Technique
The lateral approach requires a systematic, layered dissection to safely identify and address the supporting structures. The specific incision and depth of dissection will vary based on the pathology and planned procedure, but adherence to anatomical landmarks and awareness of critical neurovascular structures are constant.
Landmarks and Incision
Key anatomical landmarks are meticulously palpated and marked pre-operatively:
*
Lateral Border of the Patella:
Defines the anterior extent of the approach.
*
Lateral Joint Line:
Helps localize the menisci and femoral epicondyle.
*
Fibular Head:
A prominent bony landmark, crucial for identifying the common peroneal nerve (CPN) and LCL/PLC attachments.
*
Lateral Femoral Epicondyle:
Origin of the LCL and popliteus.
*
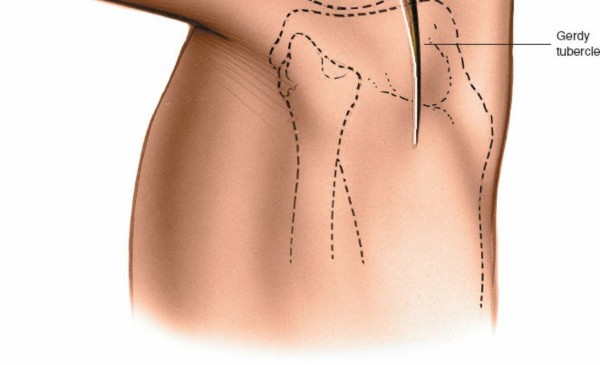
Gerdy's Tubercle:
The lateral tubercle of the tibia, palpable just lateral to the patellar ligament, marks the inferior attachment of the iliotibial band (ITB).
*
Biceps Femoris Tendon:
Courses to insert on the fibular head. The CPN lies deep and posterior to its distal aspect.
Incision:
A variety of incisions can be utilized:
*
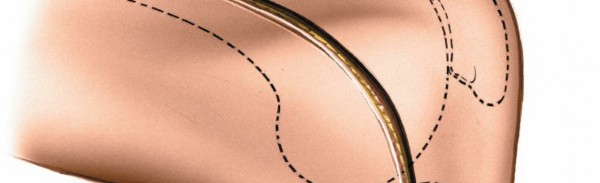
Straight Longitudinal Incision:
Centered over the lateral femoral epicondyle and fibular head. This is a common and versatile incision.
*
Modified "Lazy S" or Hockey Stick Incision:
Starting proximally along the posterior aspect of the ITB, curving anteriorly over the lateral joint line, and then distally along the fibular head. This can provide broader exposure and improve cosmesis.
*
Posterolateral Incision:
May be preferred for specific PLC reconstructions.
For most lateral approaches targeting supporting structures, a straight or slightly curved longitudinal incision, approximately 10-15 cm in length, is appropriate. It typically begins 3-4 cm proximal to the lateral femoral epicondyle, extends distally over the lateral epicondyle, lateral joint line, and fibular head, ending about 3-4 cm distal to the fibular head.

Superficial Dissection
- Skin and Subcutaneous Tissue: The incision is carried through the skin and subcutaneous fat. Superficial nerves (e.g., lateral sural cutaneous nerve, terminal branches of the common peroneal nerve) should be identified and protected, though some transection of small cutaneous branches is often unavoidable, leading to areas of post-operative numbness.
- Deep Fascia: The deep fascia investing the ITB is identified.
Deep Dissection and Internervous Planes
This stage requires meticulous dissection to identify and protect vital structures, particularly the common peroneal nerve.
-
Iliotibial Band (ITB): The ITB is a robust structure.
-
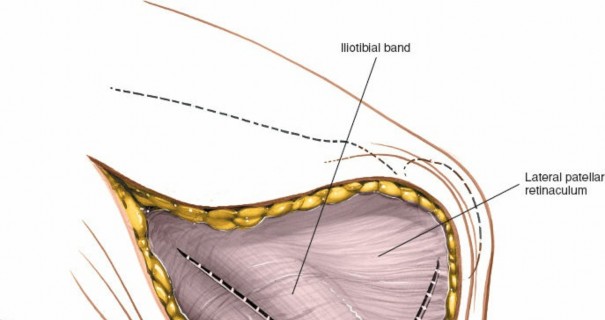
Incision:
A longitudinal incision can be made through the ITB, or it can be elevated and retracted. For a broad exposure, a longitudinal incision starting just distal to the vastus lateralis and extending to Gerdy's tubercle is effective.

- Retraction: The anterior portion of the ITB can be retracted anteriorly, exposing the vastus lateralis and lateral retinaculum. The posterior portion is retracted posteriorly.
- Internervous Plane: The ITB lies superficial to the vastus lateralis muscle (anteriorly) and the biceps femoris muscle (posteriorly).
-
Incision:
A longitudinal incision can be made through the ITB, or it can be elevated and retracted. For a broad exposure, a longitudinal incision starting just distal to the vastus lateralis and extending to Gerdy's tubercle is effective.
-
Common Peroneal Nerve (CPN) Identification and Protection: This is the most critical step.
- Localization: The CPN courses from the popliteal fossa, deep to the biceps femoris muscle, and wraps around the fibular neck, approximately 1-2 cm distal to the fibular head.
- Identification: The nerve is typically identified by dissecting along the posterior border of the biceps femoris tendon as it inserts onto the fibular head. Dissection should proceed cautiously, using blunt dissection and gentle traction. The nerve can often be palpated as a cord-like structure.
-
Protection:
Once identified, the CPN is carefully isolated, encircled with a vessel loop or Penrose drain, and gently retracted posteriorly or inferiorly, away from the operative field. Avoid excessive traction or direct compression.



-
Biceps Femoris Tendon: The conjoined tendon of the biceps femoris inserts primarily onto the fibular head.
- Retraction/Release: The biceps femoris can be retracted posteriorly. In some cases, a partial release of its anterior fibers from the fibular head may be necessary to gain better access to the LCL and PLC, but this should be done cautiously, recognizing its role in lateral stability and its proximity to the CPN.
-
Lateral Collateral Ligament (LCL):
- Identification: Once the ITB is retracted and the CPN protected, the LCL can be identified. It runs from the lateral femoral epicondyle, just distal and posterior to the origin of the popliteus tendon, to the fibular head. It is an extra-articular structure.
- Assessment: The integrity of the LCL is assessed. A torn LCL will show fraying, discontinuity, or avulsion from its femoral or fibular attachments.
-
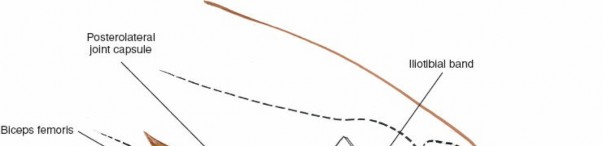
Popliteus Tendon and Posterolateral Corner (PLC):
- Identification: Deep to the LCL, the popliteus tendon can be identified emerging from the lateral femoral condyle, anterior and proximal to the LCL origin. It then courses posteromedially.
-
PLC Structures:
Further dissection posterolaterally will reveal the popliteofibular ligament (a key component of the PLC, running from the popliteus musculotendinous junction to the fibular head), and the posterolateral capsule.




- Internervous Plane: The popliteus tendon lies deep to the LCL and superficial to the lateral femoral condyle and tibia.
-
Lateral Meniscus:
- Visualization: With retraction of the ITB and judicious dissection of the capsule, the peripheral aspects of the lateral meniscus can be visualized. Intra-articular structures are often better assessed arthroscopically, but direct visualization through an open capsular incision can be performed if indicated (e.g., for complex meniscal root repairs or specific meniscectomies).
Specific Procedures
- LCL Repair: For acute avulsions, direct repair with suture anchors or through bone tunnels is preferred. For mid-substance tears, primary repair may be possible.
- LCL Reconstruction: For chronic LCL insufficiency or non-repairable acute tears, various techniques using autograft or allograft are employed (e.g., femoral tunnel, fibular head tunnel).
- PLC Reconstruction: This is more complex, often involving reconstruction of the LCL and popliteofibular ligament. Techniques such as the modified LaPrade reconstruction or anatomical dual-graft reconstructions are commonly used, aiming to restore the femoral and fibular attachments of the LCL and popliteofibular ligament. Tunnel placement must be precise to avoid iatrogenic instability or impingement.
- Fibular Head Avulsion Fixation: Avulsed fragments of the fibular head (often with biceps femoris or LCL attachment) are reduced and fixed with screws or sutures.
- Tibial Plateau Fracture ORIF: The approach provides excellent direct visualization of lateral tibial plateau fractures. Fragments are reduced, and provisional fixation (K-wires) is followed by definitive fixation with plates and screws. Bone grafting (autograft or allograft) may be required for metaphyseal defects or articular depression.
Closure
- Deep Structures: Any capsular or popliteal repairs are completed.
- ITB: The ITB is typically repaired in a tension-free manner, or if a specific release was performed, care is taken with closure based on the intended outcome.
- Subcutaneous Tissue: The subcutaneous layers are closed to obliterate dead space and minimize hematoma formation.
- Skin: The skin is closed with staples or sutures.
- Dressing: A sterile dressing is applied.
Complications & Management
Despite meticulous surgical technique, complications can occur following a lateral knee approach. Pre-operative patient counseling regarding these risks is essential.
| Complication | Incidence (Approx.) | Salvage Strategies / Management The lateral approach provides access to all the supporting structures on the lateral side of the knee. It may be extended for intra-articular exploration of the knee’s anterior and posterior structures as well.
Normally, only part of the exposure is needed for any single surgical procedure. Its major use is in the assessment of ligamentous damage, a type of pathology that is more common on the medial side because valgus stress is more common than varus stress.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following a lateral knee approach, especially for ligamentous reconstruction, is critical for achieving optimal functional outcomes and minimizing complications like stiffness or re-injury. Protocols must be individualized based on the specific structures repaired or reconstructed, the quality of fixation, concomitant injuries, and patient factors. Generally, rehabilitation progresses through phases: Protection, Controlled Motion & Early Strengthening, Intermediate Strengthening & Proprioception, and Return to Activity/Sport.
Phase I: Maximum Protection (Weeks 0-6)
Goals:
* Protect repair/reconstruction.
* Control pain and swelling.
* Achieve full passive extension.
* Initiate controlled range of motion (ROM).
* Prevent quadriceps atrophy.
Weight-Bearing:
* Typically non-weight-bearing (NWB) or touch-down weight-bearing (TDWB) with crutches for 4-6 weeks, especially after PLC reconstruction or fibular head repair.
* A hinged knee brace is applied immediately post-operatively, locked in full extension for ambulation.
Range of Motion (ROM):
* Continuous Passive Motion (CPM) machine may be used if tolerated (e.g., 0-30 degrees initially, progressing as tolerated).
* Passive knee extension exercises: heel props, prone hangs.
* Passive knee flexion: gentle gravity-assisted flexion, or manual assistance, typically limited to 0-30 degrees for the first 2 weeks, then progressing to 0-60/90 degrees by week 6, avoiding excessive varus stress or external rotation.
Therapeutic Exercises:
* Quadriceps sets, patellar mobilizations.
* Ankle pumps.
* Straight leg raises (SLRs) in supine (avoiding abduction/adduction against resistance to protect lateral structures).
* Core strengthening.
Phase II: Controlled Motion & Early Strengthening (Weeks 7-12)
Goals:
* Gradual increase in weight-bearing.
* Progressive increase in ROM.
* Improve muscle strength and neuromuscular control.
Weight-Bearing:
* Progress to partial weight-bearing (PWB) with crutches, transitioning to full weight-bearing (FWB) as tolerated, typically by week 8-10, with the brace unlocked for gait.
Range of Motion (ROM):
* Progress flexion to 120-130 degrees by week 12. Full flexion may not be achieved for several months.
Therapeutic Exercises:
* Initiate closed-chain strengthening: mini-squats, leg presses (controlled range), wall slides.
* Open-chain strengthening: gentle knee extension (avoiding terminal extension against resistance), knee flexion.
* Balance and proprioception: single-leg stance, weight shifts.
* Stationary bike (high seat, low resistance).
* Core stability exercises.
Phase III: Intermediate Strengthening & Proprioception (Weeks 13-24)
Goals:
* Achieve full pain-free ROM.
* Normalize gait pattern.
* Maximize lower extremity strength, endurance, and power.
* Enhance proprioception and agility.
Weight-Bearing & Brace:
* Discontinue brace when adequate dynamic stability and strength are demonstrated.
* Progress to full functional activities.
Therapeutic Exercises:
* Advanced closed-chain exercises: lunges, step-ups, single-leg squats.
* Resistive exercises: hamstring curls, leg extensions (progressively increasing resistance).
* Plyometrics (low impact initially): box jumps (bilateral), hopping.
* Agility drills: cone drills, lateral shuffles.
* Sport-specific conditioning (non-contact).
* Continue balance and proprioception exercises.
Phase IV: Return to Activity/Sport (Months 6-9+)
Goals:
* Gradual return to full, unrestricted activity and sport.
* Maintain strength, endurance, and flexibility.
* Prevent re-injury.
Return Criteria:
* Full pain-free ROM.
* Isokinetic strength testing: Quadriceps and hamstring strength symmetrical to contralateral limb (typically >90%).
* Functional hop testing: Single-leg hop, triple hop, crossover hop >90% of contralateral limb.
* No effusion, tenderness, or instability.
* Psychological readiness.
* Sport-specific drills without pain or apprehension.
Key Considerations:
*
Common Peroneal Nerve (CPN) Injury:
If CPN palsy occurred, specific neurological rehabilitation and potential orthotics (e.g., AFO for foot drop) will be integrated.
*
Stiffness:
Early ROM is crucial to prevent arthrofibrosis, a common complication, especially with combined injuries.
*
Varus Overload:
Avoid exercises that induce varus stress until the lateral structures are fully healed and strengthened.
*
Patient Education:
Emphasize adherence to the protocol and the importance of gradual progression to minimize the risk of re-injury.
Summary of Key Literature / Guidelines
The management of lateral knee pathologies, particularly posterolateral corner (PLC) injuries, has evolved significantly with a growing body of literature emphasizing the importance of anatomical repair and reconstruction.
-
Anatomical PLC Reconstruction:
The pioneering work by
LaPrade et al.
(2007) revolutionized PLC reconstruction by advocating for anatomical restoration of the LCL and popliteofibular ligament using two separate grafts. Their cadaveric studies and clinical outcomes demonstrated superior biomechanical and clinical results compared to non-anatomical or single-bundle techniques. The modified LaPrade technique has become a widely accepted gold standard, with various technical modifications and graft choices reported.
- Reference: LaPrade RF, Resig S, Wentorf F, et al. The anatomy of the posterolateral corner of the knee: a cadaveric study. Am J Sports Med . 2003;31(4):543-549.
- Reference: LaPrade RF, Wentorf FA, Van Citters GW, et al. Fibular collateral ligament and posterolateral corner reconstruction with a long head of the biceps femoris tendon autograft. Am J Sports Med . 2007;35(4):570-576.
-
Acute vs. Chronic Management:
Current guidelines, largely supported by systematic reviews, suggest that
acute, high-grade (Grade III) LCL and PLC injuries, especially those combined with cruciate ligament injuries, benefit significantly from early surgical intervention (repair or reconstruction) within 2-3 weeks of injury.
This approach has been shown to yield better outcomes in terms of stability restoration and lower rates of revision compared to delayed reconstruction or non-operative management for complete tears.
- Reference: Levy BA, Dajani N, Parker B, et al. Primary repair versus reconstruction of the posterolateral corner of the knee: a systematic review. Clin Orthop Relat Res . 2012;470(6):1710-1718.
- Common Peroneal Nerve (CPN) Management: A critical aspect highlighted across numerous studies is the high incidence of CPN injury associated with high-energy lateral knee trauma and PLC injuries. Guidelines emphasize thorough pre-operative neurological assessment, meticulous surgical dissection for nerve identification and protection, and prompt management of any post-operative deficit. Surgical exploration and neurolysis may be indicated for persistent palsy.
-
Concomitant Ligamentous Injuries:
The literature consistently reinforces that isolated LCL/PLC injuries are rare. Most often, they occur in the context of multi-ligamentous knee injuries (MLKI), particularly combined ACL-PLC or PCL-PLC tears.
Successful management of MLKI necessitates addressing all significant ligamentous disruptions.
Neglecting a PLC injury in an ACL-reconstructed knee, for instance, is a well-documented cause of ACL graft failure and persistent instability.
- Reference: Fanelli GC, Edson CJ. Posterior cruciate ligament injuries in trauma. J Am Acad Orthop Surg . 1998;6(5):291-304.
-
Tibial Plateau Fractures:
For lateral tibial plateau fractures, particularly those involving articular depression or significant displacement, the lateral approach (often combined with an anterolateral submeniscal arthrotomy) is well-established for direct visualization, anatomical reduction, and stable internal fixation. Literature focuses on the importance of restoring articular congruity and mechanical axis to prevent post-traumatic osteoarthritis.
- Reference: Schatzker J, Tile M. The Rationale of Operative Fracture Care . Springer-Verlag; 1987.
- Rehabilitation: Evidence-based rehabilitation protocols, characterized by phased progression, controlled ROM, delayed weight-bearing for PLC reconstructions, and early emphasis on full extension and quadriceps activation, are crucial for successful outcomes. The ultimate goal is to restore strength, proprioception, and functional stability, with a gradual return to sport criteria driven by objective performance metrics.
In summary, the lateral approach to the knee, underpinned by detailed anatomical knowledge and guided by robust clinical and biomechanical evidence, remains a cornerstone for addressing a variety of complex lateral knee pathologies, especially those involving the posterolateral corner. Adherence to established surgical principles and comprehensive post-operative rehabilitation are essential for optimizing patient outcomes.
Clinical & Radiographic Imaging