Mastering Distal Femur for Anterior ACL: Lateral Approach
Introduction & Epidemiology
The anterior cruciate ligament (ACL) is a critical stabilizer of the knee, with its rupture being a common and debilitating injury, particularly in athletic populations. The epidemiology of ACL tears demonstrates a higher incidence in younger, active individuals, with significant associated societal and healthcare burdens. Surgical reconstruction remains the gold standard for restoring knee stability and facilitating a return to high-level activity in symptomatic patients.
Historically, various techniques have evolved for femoral tunnel creation in ACL reconstruction. The lateral approach to the distal femur, often referred to as the "over-the-top" (OTT) approach, represents a historically significant and, in specific circumstances, still relevant method for managing the femoral attachment of the ACL graft. This approach, by passing the graft over the top of the posterior aspect of the lateral femoral condyle, was initially conceived to address challenges related to tunnel placement, particularly in the era prior to widespread adoption of anatomically precise arthroscopic drilling techniques. While contemporary ACL reconstruction predominantly favors anatomic femoral tunnel placement via anteromedial portal or transtibial techniques, the lateral approach retains a niche in revision surgery, pediatric cases requiring physeal sparing, or situations where standard tunnel placement is complicated by pre-existing hardware or compromised bone stock. It is typically employed in conjunction with a medial parapatellar or arthroscopic approach to the joint for graft passage and tibial tunnel creation, rarely as an isolated incision. This technique exposes the posterior aspect of the intercondylar notch and the lateral aspect of the lateral femoral condyle, providing direct visualization and access for graft fixation. Understanding this approach provides a comprehensive perspective on the evolution and current versatility of ACL reconstructive strategies.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy of the lateral distal femur and its surrounding structures is paramount for the safe and effective execution of the lateral approach.
Bony Anatomy
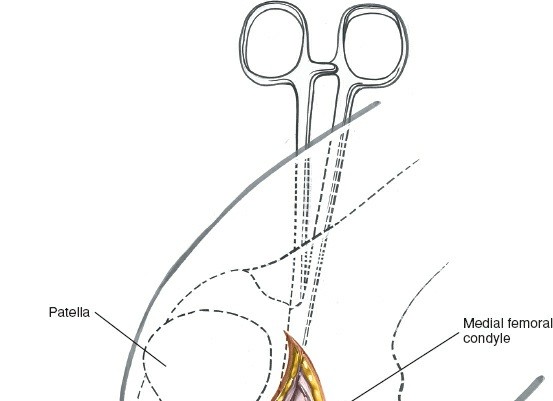
The lateral femoral condyle forms the lateral wall of the intercondylar notch. Its posterior aspect is crucial to the "over-the-top" technique. The posterior lateral margin of the lateral femoral condyle serves as a key palpable landmark, flaring out from the femoral shaft. Proximally, the condyle transitions into the supracondylar region of the femur. The precise location of the graft fixation on this posterior aspect significantly influences graft isometry and subsequent knee kinematics.
Ligamentous Structures
The anterior cruciate ligament (ACL) originates from the posterior medial aspect of the lateral femoral condyle. Its femoral attachment is broad and fan-shaped, consisting of two main bundles: the anteromedial (AM) and posterolateral (PL) bundles. The "over-the-top" position for graft placement, typically more posterior and superior on the condyle, historically aimed to mimic the isometric properties of the native ACL, though modern anatomical techniques strive for a more precise intra-articular origin.
Musculature & Fascia
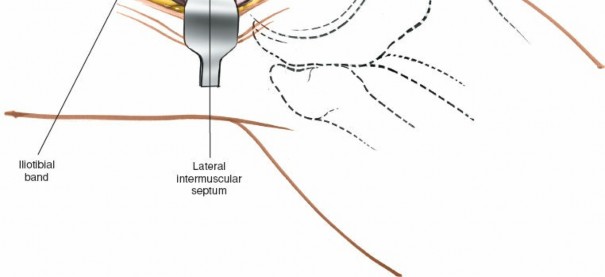
- Iliotibial Band (ITB): A thick band of fascia lata located laterally, extending from the iliac crest to Gerdy's tubercle on the tibia. It provides significant lateral stability to the knee. Its intersection with the biceps femoris muscle is a critical superficial landmark. The ITB must be incised or split longitudinally to access deeper structures.
- Biceps Femoris Muscle: The most lateral hamstring muscle, originating from the ischial tuberosity and inserting primarily into the fibular head. It lies posterior to the ITB and contributes to knee flexion and external rotation. It is retracted posteriorly during the approach.
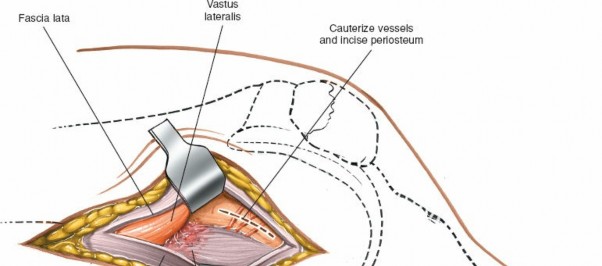
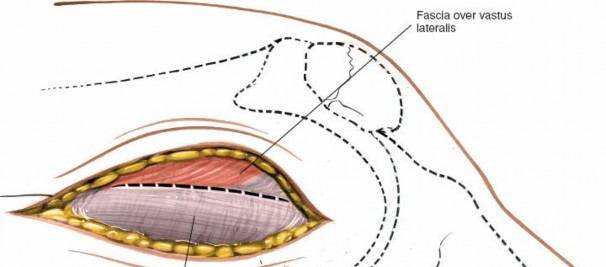
- Vastus Lateralis Muscle: The largest head of the quadriceps femoris, originating from the greater trochanter and linea aspera, inserting into the patella via the quadriceps tendon. It lies anterior to the ITB and lateral intermuscular septum and is retracted anteriorly.
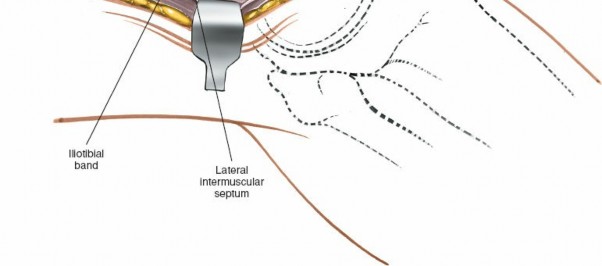
- Lateral Intermuscular Septum: A strong fascial band extending from the linea aspera to the lateral epicondyle, separating the vastus lateralis from the posterior compartment muscles. This septum must be incised to gain access to the posterior aspect of the condyle.
- Gastrocnemius Muscle (Lateral Head): Originates from the posterior aspect of the lateral femoral condyle, deep and distal to the area of the over-the-top placement. It needs careful retraction or protection if dissection extends deeply posterior.
Neurovascular Structures
- Common Peroneal Nerve: The most critical nerve at risk. It branches from the sciatic nerve in the popliteal fossa, courses laterally around the head of the fibula. Proximally, it lies posterior to the biceps femoris. During the lateral approach, it is vulnerable as the biceps femoris is retracted posteriorly, and careful protection is essential, especially when dissecting towards the fibular head or performing any posterior capsular work.
- Superior Lateral Genicular Artery and Nerve: These small vessels and nerves course around the lateral aspect of the distal femur, potentially crossing the surgical field.
- Popliteal Artery and Vein: These major vessels lie deep in the popliteal fossa, posterior to the knee joint capsule. While generally protected by the posterior capsule and gastrocnemius, aggressive posterior dissection or eccentric drill bit excursions can put them at risk.
Biomechanics
The biomechanical rationale for the "over-the-top" technique historically centered on achieving an isometric or near-isometric graft placement. By placing the graft attachment posteriorly on the lateral femoral condyle, it was believed to maintain relatively constant tension throughout the range of motion. However, modern understanding emphasizes anatomical ACL reconstruction, aiming to replicate the native footprint with its distinct AM and PL bundles. While the OTT position offers a robust cortical fixation site, it can result in a more vertical graft orientation, potentially leading to rotational instability or roof impingement if not carefully executed. In revision settings or specific anatomical challenges, the ability to utilize virgin bone posteriorly can be advantageous, offering a predictable starting point for a graft when traditional tunnel locations are compromised.
Indications & Contraindications
The lateral "over-the-top" approach for femoral fixation in ACL reconstruction, while less common for primary, anatomic reconstructions today, remains a valuable technique in specific scenarios.
Indications (Operative)
-
Revision ACL Reconstruction:
- Compromised Anatomic Femoral Tunnel: When a previously created femoral tunnel is malpositioned, excessively wide, or located such that a new anatomical tunnel cannot be safely drilled without compromising the integrity of the existing tunnel or the bone bridge.
- Failed Anatomic Reconstruction: In cases where a non-anatomic or unstable reconstruction has failed, the OTT approach provides an alternative femoral fixation point utilizing virgin bone.
-
Skeletal Immaturity (Physeal-Sparing Techniques):
- In skeletally immature patients with open physes, avoiding transphyseal drilling is crucial to prevent growth disturbances. The OTT technique allows for epiphyseal or metaphyseal femoral fixation, bypassing the physis.
-
Specific Anatomical Variations:
- Severe posterior condylar erosion or bony defects that preclude standard tunnel drilling.
- Certain congenital deformities or post-traumatic changes that alter the normal femoral anatomy.
- Combined Ligamentous Injuries with Lateral Sided Reconstruction: While primarily for ACL, the lateral approach can be extended or modified to address concomitant posterolateral corner injuries, providing direct visualization for specific repair or reconstruction procedures involving the lateral epicondyle or popliteus tendon.
-
Historically, Primary ACL Reconstruction:
- Prior to the widespread adoption of transtibial or anteromedial portal techniques, the OTT approach was a common method for femoral graft fixation, particularly with specific graft types like vastus lateralis or ITB autografts. Its utility in primary cases is now limited to very specific indications where conventional methods are not feasible.
Contraindications
- Active Infection: Any active infection in or around the knee joint is an absolute contraindication to elective ACL reconstruction due to the high risk of septic arthritis and graft infection.
- Severe Degenerative Arthritis: While not an absolute contraindication, severe osteoarthritis (grade III or IV chondrosis) may limit the expected functional outcome of ACL reconstruction, and other joint salvage or replacement strategies may be more appropriate.
- Significant Soft Tissue Compromise: Extensive scarring, poor skin quality, or compromised vascularity in the lateral distal thigh region may preclude safe incision and dissection, increasing the risk of wound complications.
- Non-Cooperative Patient: Patients unable or unwilling to comply with the rigorous post-operative rehabilitation protocol are at high risk for poor outcomes, including graft failure and arthrofibrosis.
- Extensive Prior Surgery or Hardware: Pre-existing hardware or significant scarring from multiple prior lateral knee surgeries may make dissection difficult and increase the risk of neurovascular injury.
Operative vs. Non-Operative Indications for ACL Injury
| Indication Type | Description
The Lateral approach, also known as the "over-the-top" approach, is used in conjunction with a medial parapatellar approach for repair or reconstruction of the anterior cruciate ligament. Therefore, it is not used as an isolated incision. This approach exposes the posterior aspect of the intercondylar notch by passing over the top of the posterior aspect of the lateral femoral condyle. The lateral approach to the distal femur also provides access to the lateral aspect of the lateral femoral condyle so that drill holes can be made in the condyle (if they are needed) for reattachment of the femoral end of the anterior cruciate ligament or attachment of the femoral end of an anterior cruciate substitute.
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and precise patient positioning are crucial for successful outcomes and to minimize complications.
Pre-operative Planning
- Clinical Assessment: A comprehensive history and physical examination are essential to assess knee stability, range of motion, and identify any concomitant ligamentous or meniscal pathology. Specific attention should be paid to the integrity of the posterolateral corner if the lateral approach is being considered for broader exposure.
-
Imaging Review:
- Plain Radiographs: Anteroposterior (AP), lateral, and Merchant views are obtained to assess for any pre-existing arthritic changes, alignment abnormalities, or bony defects. In revision cases, tunnel widening or hardware from previous surgeries must be evaluated.
- Magnetic Resonance Imaging (MRI): MRI is critical for confirming the ACL rupture, assessing meniscal and chondral injuries, and identifying bone bruises. In revision settings, MRI helps delineate the exact location and size of previous tunnels, vital for planning new tunnel placement to avoid impingement or blow-out.
- Computed Tomography (CT) Scan: May be useful in complex revision cases to precisely map previous tunnel locations, assess bone stock, and plan for potential bone grafting.
- Graft Selection: The choice of graft (autograft: hamstring, patellar tendon, quadriceps tendon; allograft) is determined by patient factors, surgeon preference, and the specific reconstructive goals. The OTT approach is compatible with various graft types.
- Surgical Strategy: The decision to use the lateral approach should be made pre-operatively, particularly in revision cases. The exact femoral fixation point and method (e.g., suture anchors, staples, cortical buttons) should be planned.
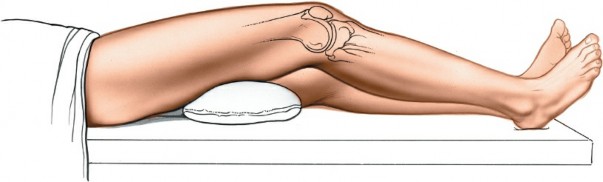
Patient Positioning
The patient is positioned supine on the operating table.
*
Anesthesia:
General or regional anesthesia (spinal/epidural) is typically employed. A femoral nerve block or adductor canal block can be used for post-operative pain management.
*
Tourniquet:
A pneumatic tourniquet is applied high on the thigh to facilitate a bloodless field.
*
Leg Holder/Support:
A lateral post or leg holder is positioned at the proximal thigh, allowing the knee to be flexed to at least 90 degrees, often more, for optimal exposure of the posterior aspect of the lateral femoral condyle. The foot is typically placed in a sterile foot holder, allowing for manipulation of the knee joint.
*
Preparation and Draping:
The entire lower extremity, from the iliac crest to the toes, is prepped and draped in a sterile fashion to allow for full range of motion of the knee and hip during the procedure.
*
* The limb is exsanguinated, and the tourniquet inflated. The operating table may be tilted to improve surgeon ergonomics.
*
* The knee is positioned in 70-90 degrees of flexion, which places the lateral femoral condyle in a more accessible position.
Detailed Surgical Approach / Technique
The lateral approach requires meticulous dissection to expose the posterior aspect of the lateral femoral condyle while protecting vital neurovascular structures.
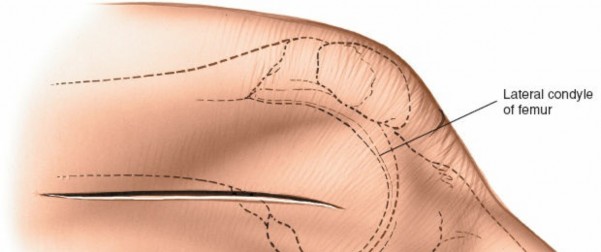
Landmarks and Incision
-
Landmarks:
- Palpate the posterior lateral margin of the lateral femoral condyle as it flares out from the shaft of the femur. This is the anatomical target for the "over-the-top" graft placement.
- Note the intersection between the iliotibial band and the biceps femoris muscle. This intersection serves as a reliable superficial guide for the skin incision.
-
Incision:
- A straight or slightly curvilinear incision, approximately 6-8 cm in length, is made over the lateral aspect of the distal femur. It typically begins slightly anterior and superior to the lateral epicondyle and extends proximally along the posterolateral aspect of the thigh, often centered around the intersection of the ITB and biceps femoris.
-
 - The skin and subcutaneous tissues are incised. Careful hemostasis is maintained.
-
 -
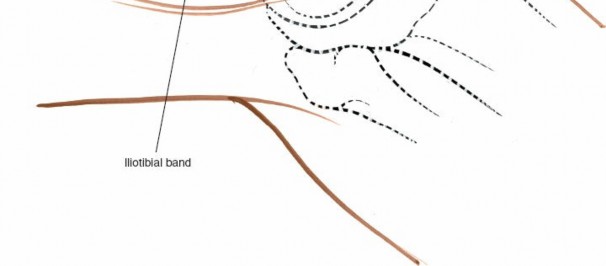
Dissection
- Incision of the Iliotibial Band (ITB): The ITB is identified lying deep to the subcutaneous fat. It is incised longitudinally, typically in line with its fibers, ensuring enough tissue remains for a strong repair at closure. The incision should be generous enough to allow for adequate exposure of the deeper structures.
-
Muscle Retraction:
- The vastus lateralis muscle, lying anterior to the ITB, is retracted anteriorly.
- The biceps femoris muscle, lying posterior to the ITB, is retracted posteriorly.
-

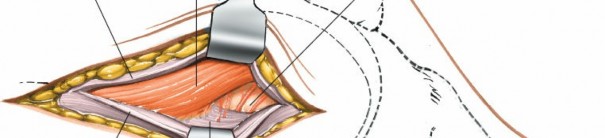
- Internervous Plane: The surgical plane is created between the vastus lateralis (innervated by the femoral nerve) and the biceps femoris (innervated by the sciatic nerve). Deep to the ITB, the lateral intermuscular septum is identified, separating the anterior and posterior compartments of the thigh. This septum is incised or split to allow further posterior retraction of the biceps femoris.
-
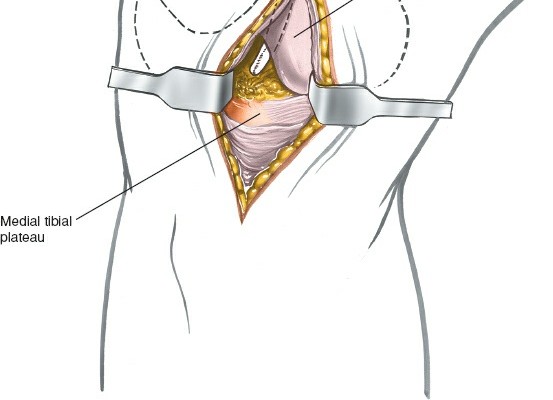
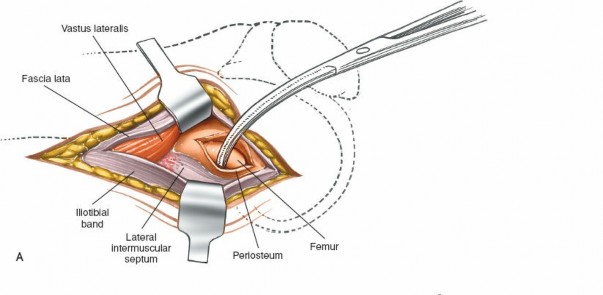
Exposure of the Lateral Femoral Condyle:
- Proceeding deeper, the posterior aspect of the lateral femoral condyle is identified. The knee is typically flexed to approximately 70-90 degrees to bring the posterior aspect of the condyle into the surgical field.
- The posterior capsule of the knee joint and the origin of the lateral head of the gastrocnemius muscle may be encountered. These structures are carefully elevated or retracted to expose the posterior margin of the lateral femoral condyle and the adjacent intercondylar notch.
- Crucial attention must be paid to the common peroneal nerve. It typically lies posterior to the biceps femoris and winds around the fibular neck. All posterior retraction should be cautious, utilizing blunt instruments and palpating for the nerve to avoid injury.
-
 -
Graft Preparation and Femoral Fixation
-
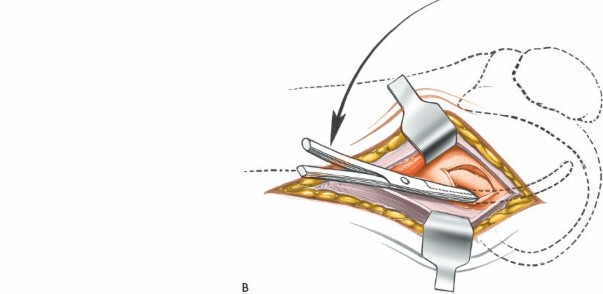
Preparation of the "Over-the-Top" Bed:
Once the posterior aspect of the lateral femoral condyle is adequately exposed, a cortical trough or a starting point for a drill hole is prepared. This typically involves rasping or burring away the cortical bone to create a flat, bleeding bed for graft coaptation. The location is usually just proximal to the origin of the lateral gastrocnemius head and distal to the posterior capsular reflection.
-
 -
 -

-
-
Graft Passage:
- A separate medial parapatellar incision or arthroscopic portals are typically used to address the intra-articular aspect of the reconstruction, including tibial tunnel creation.
- The graft, prepared to the desired length, is typically brought into the joint through a tibial tunnel. Its femoral end is then passed over the prepared "over-the-top" bed.
-
 -
 - For fixation, drill holes can be made in the condyle (if they are needed) for reattachment of the femoral end of the anterior cruciate ligament or attachment of the femoral end of an anterior cruciate substitute. Strong non-absorbable sutures are typically woven through the femoral end of the graft. These sutures are then passed through small drill holes created in the lateral femoral condyle, securing the graft tightly against the bone bed using staples, suture anchors, or a cortical button.
-
Graft Tensioning and Fixation:
With the knee in an appropriate degree of flexion (typically 20-30 degrees) and an anterior drawer force applied to the tibia, the graft is tensioned and secured. The specific angle of knee flexion during tensioning can influence graft isometricity. Final tibial fixation is performed after confirming adequate femoral fixation and graft tension.
-
-
Closure
- Capsular Repair: The posterior capsule, if opened, is meticulously repaired.
- Muscle and Fascial Repair: The lateral intermuscular septum is closed. The vastus lateralis and biceps femoris are allowed to return to their anatomical positions. The incised iliotibial band is then securely repaired with strong absorbable sutures. This repair is critical for restoring lateral stability and preventing muscular herniation.
- Subcutaneous and Skin Closure: Subcutaneous tissues are closed in layers, followed by skin closure with sutures or staples. A sterile dressing is applied.
Complications & Management
Complications following ACL reconstruction, including those specifically associated with the lateral approach, can significantly impact patient outcomes. Vigilance, early recognition, and appropriate management are crucial.
Common Complications and Management
| Complication | Incidence (Approximate) | Salvage/Management Strategy ```
Introduction & Epidemiology
The anterior cruciate ligament (ACL) is a paramount stabilizer of the tibiofemoral joint, preventing excessive anterior translation of the tibia relative to the femur and secondary valgus/varus instability, particularly in extended knee positions. Rupture of the ACL is a common and debilitating injury, predominantly affecting young, active individuals involved in pivoting and contact sports. Epidemiological data indicate an annual incidence of ACL ruptures ranging from 30 to 78 per 100,000 person-years in the general population, with higher rates observed in collegiate and professional athletes. Females are reported to have a 2-8 fold higher risk of non-contact ACL injury compared to males, attributed to a complex interplay of anatomical, hormonal, neuromuscular, and biomechanical factors.
Surgical reconstruction remains the standard of care for symptomatic patients seeking to return to high-demand activities, aiming to restore knee stability, prevent secondary meniscal and chondral damage, and mitigate the risk of premature osteoarthritis. The evolution of ACL reconstructive techniques has been marked by a continuous pursuit of anatomical fidelity, graft strength, and durable fixation. Historically, techniques for femoral tunnel placement included transtibial, anteromedial portal, and the lateral "over-the-top" (OTT) approaches.
The lateral "over-the-top" approach, the focus of this discussion, involves passing the graft over the posterior aspect of the lateral femoral condyle for femoral fixation. This technique gained prominence in an era preceding widespread understanding of anatomical tunnel placement and sophisticated arthroscopic drilling. It provided a robust, cortical fixation point, particularly advantageous when managing specific graft types (e.g., iliotibial band, vastus lateralis) or when technical limitations of existing instruments made precise intra-articular tunnel drilling challenging. While contemporary primary ACL reconstruction largely favors anatomical intra-articular femoral tunnel creation via anteromedial portals to mimic the native ACL footprint, the lateral OTT approach retains significant relevance in specific niche indications, such as complex revision ACL surgery where existing tunnels are malpositioned or significantly widened, in skeletally immature patients requiring physeal-sparing reconstruction, or in cases with unusual anatomical constraints. It is almost invariably utilized in conjunction with a medial arthrotomy or arthroscopic approach to the joint to facilitate graft passage and tibial tunnel creation. A thorough understanding of its indications, anatomical considerations, and surgical nuances is essential for any orthopedic surgeon managing complex ACL pathology.
Surgical Anatomy & Biomechanics
A profound comprehension of the regional surgical anatomy and the biomechanical implications of femoral graft placement is critical for the safe and effective application of the lateral approach.
Bony Anatomy
The lateral femoral condyle forms the lateral boundary of the intercondylar notch and articulates with the lateral tibial plateau. Its posterior aspect is central to the "over-the-top" technique. The posterior lateral margin of the lateral femoral condyle is a key palpable landmark, presenting as a distinct flare originating from the posterolateral femoral shaft. The precise location for graft placement on this posterior curve, typically just proximal to the gastrocnemius origin and distal to the posterior capsular reflection, dictates graft isometry. Proximally, the condyle transitions into the supracondylar region, where the linea aspera and attachment points for various muscles are found. The lateral epicondyle, a distinct prominence on the lateral aspect, serves as the origin for the lateral collateral ligament (LCL) and the popliteus tendon.
Ligamentous Structures
The anterior cruciate ligament (ACL) originates from the posterior medial aspect of the lateral femoral condyle, forming a broad, fan-shaped footprint. This footprint comprises two functional bundles: the anteromedial (AM) bundle, taut in flexion, and the posterolateral (PL) bundle, taut in extension. The native femoral attachment site is typically located within the intercondylar notch, positioned obliquely. The historical "over-the-top" placement on the posterior cortex of the lateral condyle, while providing a strong cortical purchase, typically positions the graft more superior and posterior than the anatomical footprint. The lateral collateral ligament (LCL) originates from the lateral epicondyle, running to the fibular head, and must be respected during lateral dissection.
Musculature & Fascia
- Iliotibial Band (ITB): A dense, fibrous aponeurotic structure that constitutes the lateral thickening of the fascia lata. It originates from the iliac crest (tensor fasciae latae and gluteus maximus insertions) and inserts primarily onto Gerdy's tubercle on the anterolateral tibia. It acts as a secondary knee stabilizer. The ITB must be incised longitudinally to access the deeper plane.
- Biceps Femoris Muscle: The most lateral muscle of the hamstring group, comprising a long head (originating from the ischial tuberosity) and a short head (originating from the linea aspera and lateral supracondylar ridge). It inserts primarily onto the fibular head. It lies posterior to the ITB and is retracted posteriorly during the approach.
- Vastus Lateralis Muscle: The largest component of the quadriceps femoris, originating from the greater trochanter and linea aspera, and inserting into the patella via the quadriceps tendon. It lies anterior to the lateral intermuscular septum and is retracted anteriorly.
- Lateral Intermuscular Septum: A strong fibrous septum extending from the linea aspera of the femur to the lateral epicondyle. It separates the vastus lateralis (anterior compartment, femoral nerve innervation) from the biceps femoris (posterior compartment, sciatic nerve innervation). Incision of this septum is essential to access the posterior aspect of the condyle.
- Gastrocnemius Muscle (Lateral Head): Originates from the posterior aspect of the lateral femoral condyle, specifically from a distinct facet on the superior-posterior surface. This origin lies just distal and somewhat anterior to the typical "over-the-top" graft pathway and must be carefully managed to avoid damage.
Neurovascular Structures
- Common Peroneal Nerve: This is the structure most vulnerable to injury during the lateral approach. It branches from the sciatic nerve in the popliteal fossa, courses inferolaterally, running superficial to the popliteus muscle and deep to the biceps femoris tendon, before winding around the fibular neck. All posterior retraction, particularly of the biceps femoris, must be performed with extreme caution, utilizing blunt instruments and identifying the nerve through palpation or direct visualization if necessary.
- Popliteal Artery and Vein: These major neurovascular structures lie deep within the popliteal fossa, posterior to the knee joint capsule. While typically protected by the posterior capsule, vigorous posterior dissection or eccentric drill bit excursion during tunnel creation can pose a risk.
- Superior Lateral Genicular Artery and Nerve: These smaller neurovascular structures course around the lateral aspect of the distal femur and can be encountered during the dissection. They should be cauterized or ligated if necessary.
Biomechanics
The biomechanical rationale for the "over-the-top" technique, particularly in its original conception, centered on achieving a relatively isometric graft placement—where graft tension remains constant throughout the knee's range of motion. By placing the femoral attachment posteriorly and proximally on the lateral femoral condyle, it was believed to minimize changes in graft length. However, comparative biomechanical studies have shown that the OTT position often results in a more vertical graft orientation within the intercondylar notch compared to anatomically placed tunnels. A more vertical graft may offer excellent anterior-posterior stability but can be less effective in controlling rotational stability (pivot shift phenomenon). Furthermore, the graft can impinge on the intercondylar roof in full extension if not carefully managed. Despite these potential limitations, the OTT provides a strong, reliable cortical fixation point, which is particularly advantageous in revision cases with compromised intra-articular bone stock or for physeal-sparing techniques where metaphyseal fixation is preferred over transphyseal drilling. The ultimate goal remains a stable, functional knee, and the OTT can achieve this in selected patients when applied judiciously.
Indications & Contraindications
The utility of the lateral "over-the-top" approach for femoral graft fixation in ACL reconstruction has evolved considerably. While it is rarely the primary choice for contemporary anatomical reconstructions, it remains an indispensable technique in specific, challenging clinical scenarios.
Indications (Operative)
- Revision ACL Reconstruction with Compromised Femoral Tunnel: This is arguably the most common contemporary indication. When a previous femoral tunnel is malpositioned (e.g., too anterior, too vertical), significantly enlarged, or has compromised bone stock, making a new anatomical intra-articular tunnel technically difficult or risky, the OTT approach provides a virgin cortical bone fixation site on the posterior aspect of the lateral femoral condyle. This avoids tunnel convergence or creation of a stress riser in already weakened bone.
- Skeletal Immaturity (Physeal-Sparing Techniques): In skeletally immature patients with open femoral physes, the goal is to reconstruct the ACL while minimizing the risk of growth disturbance. The OTT technique allows for epiphyseal or metaphyseal femoral fixation without violating the physis, often by securing the graft directly over the posterior condyle with staples or suture anchors, or through an epiphyseal tunnel.
-
Specific Anatomical Challenges:
- Extensive Bony Defects: In cases of severe posterior condylar erosion, avulsion fractures of the femoral ACL attachment site, or other post-traumatic changes that alter normal anatomy, the robust cortical fixation provided by the OTT can be advantageous.
- Congenital Abnormalities: Rare cases with unique femoral morphology where standard intra-artarticular tunnel creation is impractical.
- Concomitant Posterolateral Corner (PLC) Reconstruction: Although the lateral approach itself is for ACL femoral fixation, the incision can be readily extended or modified to facilitate exposure for PLC repair or reconstruction, particularly when addressing avulsion fractures or direct repair of the lateral collateral ligament or popliteus tendon.
- Historical Primary ACL Reconstruction: In the past, especially with certain autograft choices like the iliotibial band or vastus lateralis, and before the advent of precise arthroscopic femoral drilling guides, the OTT technique was a commonly employed method for primary ACL reconstruction. While largely superseded by anatomical techniques for primary cases, understanding its historical context is important.
Contraindications
- Active Septic Arthritis: Any active infection within the knee joint is an absolute contraindication to elective ACL reconstruction due to the high risk of graft infection and irreversible cartilage damage.
- Severe Degenerative Joint Disease: In patients with advanced knee osteoarthritis (Kellgren-Lawrence grade III or IV), the expected functional benefits of ACL reconstruction may be limited, and other treatment strategies (e.g., osteotomy, arthroplasty) may be more appropriate.
- Compromised Soft Tissue Envelope: Significant scarring, poor skin quality, or compromised vascularity in the lateral distal thigh from previous surgeries, trauma, or radiation can increase the risk of wound complications and infection, making the lateral approach less advisable.
- Non-Compliant Patient: Patients unwilling or unable to adhere to the rigorous post-operative rehabilitation protocol are at a high risk of poor outcomes, including graft failure, arthrofibrosis, and persistent instability.
- Extreme Obesity: While not an absolute contraindication, morbid obesity can significantly increase the technical difficulty of the exposure, lengthen surgical time, and elevate the risk of wound complications and nerve injury.
- Prior Lateral Surgical Scars: Extensive scarring from multiple previous lateral knee surgeries may make dissection challenging and increase the risk of iatrogenic injury to neurovascular structures.
Operative vs. Non-Operative Indications for ACL Injury
| Indication Type | Patient Profile & Clinical Presentation | Specific Considerations for Lateral Approach (if Operative) | Common Peroneal Nerve Injury | Rare, but can be severe. Up to 10% in some series, mostly neurapraxia. | Immediate cessation of aggravating maneuvers. If confirmed injury, exploration, neurolysis, or repair. Pre-op counseling on foot drop risk. Post-op AFO for gait. Refer to neurology for evaluation and potential neurosurgery. |
|
Operative
| |
|
Non-Operative
| | Description |
|
* |
*Operative Indications:
|
|
Primary ACL Reconstruction
|
Non-Operative:
|
|
Operative:
| High-level athletic demands (e.g., pivot sports). | Revision cases: The lateral approach offers a "clean" path to virgin bone when existing tunnels are compromised, facilitating robust new graft fixation and avoiding prior hardware.
Physeal-sparing cases: Provides the ability to fix the graft directly to the metaphysis/epiphysis, circumventing the growth plate and minimizing risk of iatrogenic physeal arrest. |
|
Revision ACL with Degraded Tunnels:
If existing bone tunnels are severely expanded or non-anatomically placed. |
Skeletal Immature Patients:
When physeal-sparing techniques are mandated to avoid iatrogenic growth arrest. |
|
Non-Operative:
| Sedentary lifestyle, low-demand activities, isolated ACL tear with minimal instability, good quadriceps strength, no concomitant injuries. | N/A (The lateral approach is a surgical technique, not a non-operative treatment determinant.) |
|
Non-Operative:
| Minimal ACL tear or avulsion, low-demand lifestyle, older patients, sedentary profession, good quadriceps strength, no concomitant meniscal or other ligamentous injuries. | N/A (The lateral approach is a surgical technique, not a non-operative treatment determinant.) |
Non-Operative:
|
Non-Operative:
| Observation, physical therapy, bracing for symptomatic instability during activities of daily living. | N/A (The lateral approach is a surgical technique, not a non-operative treatment determinant.) | | |
|
Non-Operative:
| Initial management of pediatric patients with open growth plates (may transition to surgical later). | N/A |
|
Non-Operative:
| Patients with significant comorbidities precluding surgery. | N/A |
Non-Operative:
| Patients who prioritize conservative management, or where surgery poses excessive risk. | N/A |
Non-Operative:
| Patients who are not surgical candidates due to medical comorbidities, or those who choose non-operative management after thorough counseling on risks and benefits. | N/A |
Non-Operative:
| Patients seeking to delay surgery, undergo a trial of conservative treatment. | N/A |
|
Non-Operative:
| Patients with isolated tears of the posterior cruciate ligament (PCL) or medial collateral ligament (MCL) that are healing well. | N/A |
Non-Operative:
| Unwillingness to undergo surgery, or medical contraindications for anesthesia/surgery. | N/A | |
| | |
|
Non-Operative:
| Previous attempts at surgical reconstruction failed due to specific factors (e. | N/A
Clinical & Radiographic Imaging