Introduction & Epidemiology
Calcaneal fractures represent a significant and challenging subset of lower extremity trauma. As the most frequently fractured tarsal bone, they account for approximately 60% of all tarsal injuries and 2% of all fractures in the adult skeleton. These fractures typically result from high-energy axial loading mechanisms, such as falls from height or motor vehicle accidents, leading to substantial disruption of the intricate hindfoot architecture. The demographic most commonly affected comprises young to middle-aged males.
The calcaneus plays a pivotal role in hindfoot biomechanics, serving as the primary heel strike absorber, a lever arm for the triceps surae, and the foundation for the subtalar joint. Displacement or comminution of the calcaneus, particularly intra-articular involvement of the posterior facet, can lead to chronic pain, stiffness, deformity, and significant functional impairment if not anatomically reduced and stably fixed. The resultant loss of Böhler's angle, widening of the calcaneal body, and impaction of the subtalar joint directly compromise the load-bearing and shock-absorbing capabilities of the hindfoot.
The lateral approach to the calcaneus, specifically the extensile lateral approach (ELA), has long been a cornerstone for surgical management of displaced intra-articular calcaneal fractures. This approach provides unparalleled visualization of the posterior facet, the lateral calcaneal wall, and allows for direct reduction of the displaced fragments and stable internal fixation. While alternative approaches, such as sinus tarsi or percutaneous techniques, have gained traction for specific fracture patterns, the ELA remains the gold standard for complex, displaced intra-articular fractures where anatomical restoration of the subtalar joint and overall calcaneal morphology is paramount. This guide aims to provide a comprehensive review of the indications, surgical technique, and management considerations for mastering the lateral approach to the calcaneus.
Surgical Anatomy & Biomechanics
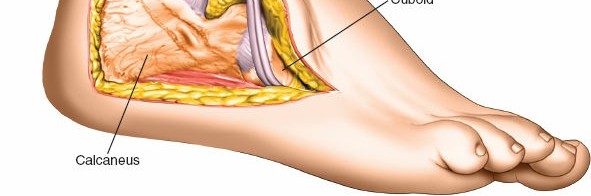
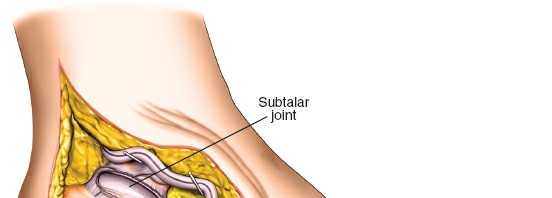
A thorough understanding of calcaneal anatomy and its biomechanical function is critical for successful surgical intervention. The calcaneus is an irregularly shaped bone forming the posterior aspect of the foot, articulating with the talus superiorly (subtalar joint) and the cuboid anteriorly (calcaneocuboid joint).
Anatomical Landmarks and Surfaces
- Body: The main bulk of the calcaneus.
- Tuberosity: The most posterior part, serving as the insertion for the Achilles tendon.
- Sustentaculum Tali: A medial shelf-like projection supporting the talar head and carrying the grooves for the flexor hallucis longus (FHL) tendon. This structure is crucial for medial column stability and is often a key fragment in comminuted fractures.
- Peroneal Trochlea (Peroneal Tubercle): A variable bony prominence on the lateral aspect, separating the tendons of peroneus longus and brevis.
-
Articular Facets:
The superior surface of the calcaneus features three articular facets for articulation with the talus:
- Posterior Facet: The largest and most crucial for subtalar joint function, typically concave and ovoid. Its integrity dictates the prognosis for post-traumatic arthritis.
- Middle Facet: Smaller, located anteromedial to the posterior facet, separated by the sinus tarsi.
- Anterior Facet: The smallest, anterior to the middle facet.
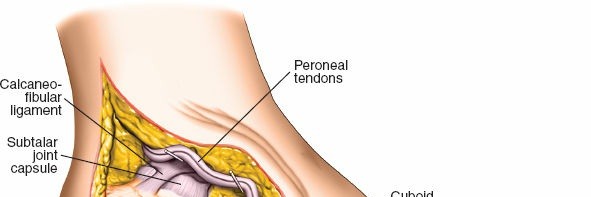
- Sinus Tarsi: A tunnel formed by the sulcus calcanei and sulcus tali, containing fat, neurovascular structures, and ligaments (cervical and interosseous talocalcaneal ligaments).
- Lateral Wall: The lateral aspect of the calcaneus, often extruded or comminuted in high-energy fractures, potentially impinging on the peroneal tendons.
Neurovascular Structures of Clinical Relevance to the Lateral Approach
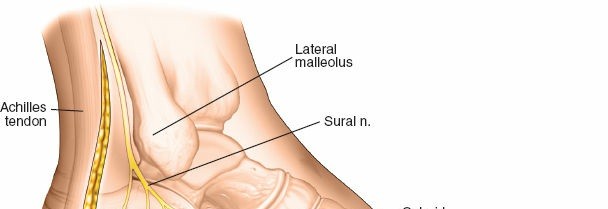
- Sural Nerve: Arises from the tibial and common peroneal nerves, typically courses along the lateral aspect of the Achilles tendon, then anteriorly near the inferior border of the fibula, providing sensation to the lateral ankle and foot. It is highly susceptible to injury during the extensile lateral approach.
- Peroneal Tendons (Longus and Brevis): Course posterior to the lateral malleolus within their fibrous sheath, passing superior to the peroneal trochlea. The peroneus brevis inserts onto the base of the fifth metatarsal, while the longus continues plantarward to insert on the medial cuneiform and first metatarsal. They lie directly beneath the incision for the lateral approach and must be carefully protected.
- Lesser Saphenous Vein: Often accompanies the sural nerve.
- Calcaneal Branches of the Posterior Tibial Artery: These provide critical blood supply to the skin and soft tissues around the heel and are vulnerable during flap elevation.
Biomechanics and Fracture Patterns
The calcaneus functions as a shock absorber, transmitting axial loads from the tibia to the ground. In high-energy injuries, the talus acts as a wedge, impacting into the calcaneal body. This typically results in characteristic fracture patterns:
- Böhler's Angle: Formed by the intersection of a line from the anterior process to the apex of the posterior facet and a line from the apex of the posterior facet to the superior aspect of the tuberosity. Normal values range from 20-40 degrees. A decrease indicates collapse of the posterior facet and calcaneal body.
- Gissane's Angle (Crucial Angle of Gissane): Formed by the intersection of the lateral process of the talus, the posterior facet, and the anterior process. Normal values are 100-130 degrees. Its disruption indicates subtalar joint involvement.
Calcaneal fractures are broadly classified into extra-articular and intra-articular types. The Sanders classification, based on CT imaging of the posterior facet, is widely used for intra-articular fractures:
*
Type I:
Non-displaced intra-articular fracture.
*
Type II:
Two-part fracture of the posterior facet.
*
Type III:
Three-part fracture of the posterior facet.
*
Type IV:
Four-part or severely comminuted fracture of the posterior facet.
The mechanism of injury often determines the fracture pattern:
*
Tongue-Type:
A fracture line extends posteriorly, separating a "tongue" fragment including the posterior facet and calcaneal tuberosity.
*
Joint Depression Type:
The posterior facet is depressed into the calcaneal body, often with significant comminution of the calcaneal body and lateral wall extrusion.
Understanding these anatomical relationships and biomechanical principles is paramount for achieving accurate reduction and stable fixation, ultimately influencing long-term functional outcomes.
Indications & Contraindications
The decision to proceed with surgical intervention for calcaneal fractures, particularly via the extensile lateral approach, requires careful consideration of fracture characteristics, patient comorbidities, and surgeon expertise.
Indications for the Lateral Approach
-
Displaced Intra-Articular Calcaneal Fractures:
- Sanders Type II, III, and IV fractures: Especially those with significant displacement (>2mm) of the posterior facet, articular step-off, or incongruity of the subtalar joint.
- Loss of Böhler's Angle: Significant reduction (<15-20 degrees) indicating collapse of the calcaneal body and posterior facet depression.
- Calcaneal Widening and Shortening: Disrupting normal hindfoot alignment and potentially impinging on the fibula or soft tissues.
- Lateral Wall Blowout/Extrusion: Impinging on the peroneal tendons or causing significant soft tissue irritation.
- Tongue-type fractures: With significant posterior displacement of the tongue fragment.
- Joint Depression type fractures: Where direct visualization and reduction of the depressed posterior facet are necessary.
-
Displaced Extra-Articular Fractures:
- While less common, some displaced extra-articular fractures (e.g., severe displacement of the calcaneal tuberosity, anterior process fractures with significant subtalar involvement) may benefit from an open approach for anatomical reduction and fixation, particularly if associated with subtalar joint involvement.
-
Treatment of Other Lesions:
- Fractures or other pathologies involving the posterior facet of the subtalar joint or lateral wall of the os calcis requiring direct access for reconstruction or excision.
- Persistent peroneal tendon subluxation or impingement secondary to fracture deformity.
Contraindications for the Lateral Approach
The lateral approach, particularly the extensile variant, is associated with a high risk of soft tissue complications, making meticulous patient selection and timing crucial.
-
Severe Soft Tissue Compromise:
- Presence of significant soft tissue swelling, tension blisters (especially hemorrhagic), impending skin necrosis, or open wounds. It is critical to allow this soft tissue swelling to subside before surgery is carried out to reduce the risk of skin necrosis. The "wrinkle sign" is a reliable indicator of adequate soft tissue resolution.
- Active cellulitis or deep infection of the surgical site.
-
Patient-Related Factors:
- Diabetes mellitus, especially with associated neuropathy and/or microvascular disease: Significantly increases the risk of wound complications, infection, and poor healing.
- Smoking: A potent vasoconstrictor and inhibitor of wound healing, markedly increasing complication rates.
- Peripheral Vascular Disease (PVD): Compromised vascular status further elevates the risk of wound breakdown. An accurate assessment of the vascular status of the patient is critical before undertaking surgery.
- Severe Medical Comorbidities: Patients unfit for prolonged anesthesia or significant blood loss.
- Advanced Age: While not an absolute contraindication, older patients may have compromised skin quality and healing capacity.
- Poor Patient Compliance: Unwillingness or inability to adhere to post-operative non-weight-bearing protocols.
-
Fracture Characteristics:
- Non-displaced or Minimally Displaced Fractures: (e.g., Sanders Type I fractures or extra-articular fractures without significant displacement). These are typically managed non-operatively.
- Severely Comminuted Fractures (Sanders Type IV): Especially in the presence of severe osteoporosis, where anatomical reduction and stable fixation may be unachievable or result in hardware prominence, leading to consideration of primary subtalar arthrodesis or non-operative management.
- "Salvageable" vs. "Non-Salvageable" Foot: In cases of devastating injury where the functional outcome is predicted to be extremely poor despite aggressive reconstruction, non-operative management or primary arthrodesis may be considered.
- Lack of Surgical Expertise: The extensile lateral approach is technically demanding and should only be performed by surgeons experienced in foot and ankle trauma.
Operative vs. Non-Operative Indications
The decision-making process for calcaneal fractures is complex and hinges on a nuanced understanding of these indications and contraindications.
| Indication Type | Operative Management (Lateral Approach) | Non-Operative Management |
|---|---|---|
| Fracture Pattern | Displaced intra-articular (Sanders Type II, III, IV) | Non-displaced intra-articular (Sanders Type I) |
| Significant articular step-off (>2mm) of posterior facet | Non-displaced extra-articular fractures | |
| Significant Böhler's angle depression (<15-20 degrees) | Minimally displaced extra-articular fractures | |
| Severe calcaneal widening/shortening | Severely comminuted fractures with poor bone quality (relative) | |
| Lateral wall extrusion/impingement | ||
| Patient Factors | Medically fit, good soft tissue envelope (wrinkle sign present) | Severe comorbidities (PVD, uncontrolled DM, neuropathy) |
| Non-smoker or committed to smoking cessation | Active smoker, unwilling to quit | |
| Absence of severe peripheral neuropathy | Severe soft tissue compromise (blisters, open wounds, infection) | |
| High functional demand, desire for anatomical restoration | Low functional demand, sedentary lifestyle, elderly (relative) | |
| Timing | Delayed surgery after resolution of soft tissue swelling (7-14 days) | Immediate management for non-operative cases, ongoing monitoring |
| Outcome Goal | Anatomical reduction, restoration of subtalar congruity | Symptomatic relief, functional adaptation |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and precise patient positioning are fundamental to optimizing outcomes and minimizing complications in calcaneal fracture repair via the lateral approach.
Pre-Operative Planning
-
Clinical Assessment:
- Thorough history and physical examination, including assessment of the entire limb for associated injuries (e.g., spine, contralateral lower extremity, pelvis).
- Detailed neurovascular assessment of the foot.
- Careful evaluation of the soft tissue envelope: inspect for open wounds, abrasions, lacerations, or blisters. The presence of tension blisters, especially hemorrhagic, mandates delaying surgery. The "wrinkle sign" (restoration of skin creases on the lateral heel) is a critical indicator of subsiding edema and readiness for surgery, typically appearing 7-14 days post-injury.
- Identify and document any pre-existing comorbidities such as diabetes, peripheral vascular disease, or smoking status, as these significantly influence surgical timing and risk.
-
Imaging Review:
- Standard Radiographs: Lateral, axial (Harris), and Broden's views are essential for initial assessment. Böhler's and Gissane's angles should be measured.
-
Computed Tomography (CT) Scan:
Mandatory for all suspected intra-articular calcaneal fractures. Fine-cut (1-2mm) axial, sagittal, and coronal reconstructions are critical for:
- Detailed fracture characterization (Sanders classification).
- Assessment of posterior facet involvement, displacement, and comminution.
- Evaluation of sustentaculum tali, calcaneocuboid joint, and anterior process.
- Identification of impacted bone fragments and lateral wall extrusion.
- 3D reconstructions can aid in visualizing the overall deformity and planning reduction maneuvers.
-
Surgical Strategy Development:
-
Based on CT imaging, formulate a clear surgical plan:
- Determine the primary fracture fragments requiring reduction.
- Anticipate specific reduction maneuvers (e.g., disimpaction, joystick placement, lamina spreader use).
- Consider the sequence of reduction (often starting with the posterior facet, using the talus as a template).
- Plan the optimal placement of hardware (e.g., pre-contoured calcaneal plate, lag screws).
- Anticipate potential challenges and alternative strategies.
-
Based on CT imaging, formulate a clear surgical plan:
-
Hardware Selection:
- Pre-contoured calcaneal plates (locking and non-locking options) are commonly used.
- Various screw types (e.g., cortical, cancellous, locking) and lengths should be available.
- K-wires for provisional fixation.
- Specialized instruments such as lamina spreaders, Hohmann retractors, distraction frames, and pointed reduction clamps.
-
Patient Optimization:
- Address any modifiable risk factors: smoking cessation, glucose control in diabetics.
- Pre-operative antibiotics administered within 60 minutes of incision.
- DVT prophylaxis plan.
Patient Positioning
Place the patient in the lateral position on the operating table.
- Lateral Decubitus: Position the patient in a true lateral decubitus position with the affected limb superior. This allows gravity to assist with retraction and provides excellent access to the lateral aspect of the hindfoot.
- Limb Positioning: The leg that is to be operated on posteriorly with the under leg anterior. This arrangement helps prevent impingement and allows for full range of motion of the operative limb.
- Padding: Ensure that the bony prominences (e.g., contralateral knee, greater trochanter, dependent malleolus, and elbow) are well padded to prevent pressure sores or nerve palsies. A beanbag can be used to stabilize the patient.
- Tourniquet Application: A pneumatic tourniquet is applied high on the ipsilateral thigh.
- Exsanguination: Exsanguinate the limb either by elevating it for 3 to 5 minutes or by applying a soft rubber bandage (e.g., Esmarch bandage). Inflate a tourniquet to 250-300 mmHg (or 100 mmHg above systolic blood pressure) to create a bloodless field, which is crucial for identifying anatomical structures and fracture fragments.
- Sterile Preparation and Draping: Prepare the limb from the mid-thigh to the toes, circumferentially. Drape the limb to allow complete access to the lateral aspect of the ankle and hindfoot, and potentially the plantar aspect if needed for reduction maneuvers or K-wire insertion. Ensure visualization of the lateral malleolus, Achilles tendon, and base of the fifth metatarsal.
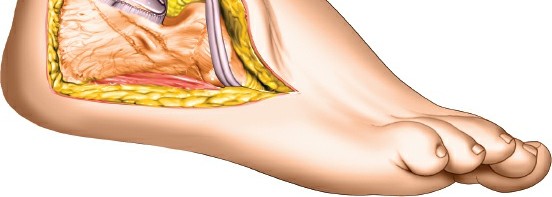
Detailed Surgical Approach / Technique
The extensile lateral approach to the calcaneus is a technically demanding procedure that requires meticulous dissection, precise reduction, and stable fixation. The goal is to restore the normal anatomy of the calcaneus, particularly the posterior facet of the subtalar joint, Böhler's angle, Gissane's angle, and calcaneal width and height.
Incision and Soft Tissue Dissection
The most common incision is the extensile "L-shaped" lateral approach, also known as the Cincinnati approach or modified Ollier approach.
-
Landmarks:
- Palpate the posterior border of the distal fibula.
- Palpate the lateral border of the Achilles tendon.
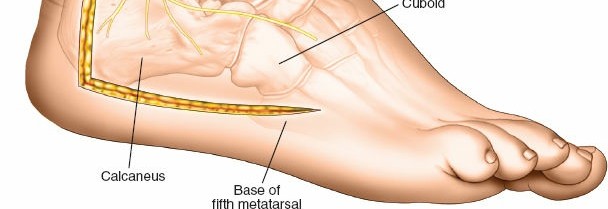
- Next, identify the styloid process at the base of the fifth metatarsal bone.
- The incision is planned to avoid crossing the calcaneal tuberosity or the sural nerve distribution directly.
-
Incision:
- The vertical limb of the L-shaped incision starts superiorly, approximately 1-2 cm posterior to the tip of the lateral malleolus. It extends inferiorly, curving anteriorly just above the insertion of the Achilles tendon, then proceeds distally along the lateral border of the Achilles tendon toward the lateral calcaneal tuberosity.
- The horizontal limb extends anteriorly from the inferior aspect of the vertical limb, parallel to the plantar aspect of the foot, toward the sinus tarsi and the base of the fifth metatarsal. The anterior extent of the incision should not cross the peroneal tendons or the sural nerve unnecessarily.
-
 - This full-thickness flap typically includes the skin, subcutaneous tissue, and the peroneal retinaculum, ensuring adequate vascularity.
-
Flap Elevation:
- The skin incision is carried down to the lateral wall of the calcaneus in a single full-thickness flap.
- Carefully identify and protect the sural nerve, which is typically located in the subcutaneous fat superior and anterior to the incision. It should be meticulously dissected and retracted with a vessel loop.
- Identify the peroneal tendons (peroneus longus and brevis) and their sheath, which lie deep to the sural nerve and superficial to the calcaneus. These tendons are retracted superiorly. The peroneal retinaculum is incised to allow full exposure and protection.
- The subperiosteal elevation of the lateral flap then proceeds, carefully dissecting from posterior to anterior, exposing the lateral wall of the calcaneus, the calcaneofibular ligament, and the sinus tarsi. This exposes the fracture fragments of the lateral wall, the posterior facet, and the calcaneocuboid joint.
-
Fracture Exposure and Debridement
-
Lateral Wall Osteotomy/Dissection:
- Often, the lateral wall of the calcaneus is extruded, comminuted, or impacted. The goal is to gain access to the underlying subtalar joint and calcaneal body.
- If the lateral wall is significantly comminuted and non-reconstructible, these fragments may be removed to facilitate visualization. If reconstructible, they are carefully preserved.
- A lateral wall osteotomy, often creating a hinged flap, may be performed to expose the depressed posterior facet. This involves making an osteotomy line along the plantar aspect of the calcaneus and hinging the lateral wall superiorly.
-
Debridement:
- Evacuate hematoma and debride small, non-articular, severely comminuted cancellous bone fragments that obscure visualization or impede reduction.
- Preserve all viable bone fragments, especially those contributing to the articular surface.
-
Reduction Techniques
The reduction sequence typically prioritizes the restoration of the posterior facet articular surface, followed by correction of calcaneal height, length, and width.
-
Disimpaction and Provisional Fixation:
- The lateral aspect of the calcaneal body is often impacted medially. A lamina spreader or dedicated calcaneal distractor may be applied between the talus and calcaneus in the sinus tarsi to indirectly distract the subtalar joint and disimpact the fracture fragments.
- Alternatively, a large Hohmann retractor or osteotome can be used as a lever to disimpact the lateral wall and de-rotate the tuberosity.
- Restore Böhler's angle using provisional K-wires from the posterior tuberosity.
- Restore Gissane's angle.
-
Posterior Facet Reduction:
- This is the most critical step. Using small osteotomes, elevators, or joy-sticks, carefully elevate the depressed posterior facet fragments.
- The talus acts as an anatomical template for reduction. The goal is to achieve an anatomical, congruent articular surface.
- Once the posterior facet is reduced, provisional K-wires are inserted from the lateral aspect into the talus to hold the reduction. These pins must be placed carefully to avoid impinging on the articular surface.
-
-
Restoration of Calcaneal Body Morphology:
- Height: Once the posterior facet is reduced, the calcaneal height is restored by packing the underlying cancellous void with cancellous bone graft (autograft from the iliac crest or allograft) to support the reduced articular surface. This also helps elevate Böhler's angle.
- Width: The lateral wall, if present and reconstructible, is reduced to correct the calcaneal width. This often involves reducing the lateral wall against the reconstituted sustentaculum and body. If the lateral wall is severely comminuted and cannot be reconstructed, the goal is to ensure the peroneal tendons are not impinged.
- Length and Rotation: Ensure the tuberosity fragment is aligned to restore overall calcaneal length and rotational alignment. This may require further joystick manipulation and K-wire fixation.
Internal Fixation
Once anatomical reduction is achieved, stable internal fixation is performed.
-
Plate Application:
- A pre-contoured calcaneal plate is typically used. This plate is designed to span the fracture lines and provide buttress support to the lateral wall and subtalar joint.
- The plate is applied to the lateral aspect of the calcaneus, ensuring it fits snugly without compressing the peroneal tendons.
- Provisional K-wires can be used to hold the plate in position while screws are inserted.
-

-
Screw Insertion:
- Insert screws through the plate, ensuring bicortical purchase where appropriate for stability.
- Locking screws are often preferred in osteoporotic bone or for greater construct stability.
- Lag screws can be used independent of the plate or through plate holes to compress specific fracture fragments (e.g., posterior facet, sustentaculum tali).
- The posterior facet screws should be inserted perpendicular to the articular surface to maximize compression.
- Check intra-operative fluoroscopy (Broden's view, axial view, lateral view) to confirm screw positions, articular congruity, and overall calcaneal alignment.
-
-
Final Assessment:
- After fixation, re-evaluate the subtalar joint for congruity and stability.
- Check for hardware prominence, particularly under the peroneal tendons or in the sinus tarsi.
- Confirm restoration of Böhler's and Gissane's angles.
- Assess ankle and subtalar range of motion to ensure no impingement.
Wound Closure
- Irrigation: Thoroughly irrigate the wound with saline.
- Drain Placement: A closed suction drain is frequently placed deep to the flap, particularly in cases with significant dead space or anticipated hematoma, to reduce the risk of wound hematoma and infection. The drain is usually brought out through a separate stab incision distal to the main incision.
- Flap Readaptation: Carefully re-drape the full-thickness lateral flap, ensuring no tension on the incision line.
-
Layered Closure:
Close the wound in layers:
- Deep fascia (peroneal retinaculum) if disrupted.
- Subcutaneous tissue to reduce dead space.
- Skin closure with sutures or staples, ensuring meticulous skin edge approximation without tension.
- Dressing and Splint: Apply a sterile, non-compressive dressing. A posterior splint, incorporating the ankle in a neutral or slight dorsiflexion position, is applied to protect the repair and minimize swelling.
Complications & Management
Despite meticulous surgical technique, the extensile lateral approach to the calcaneus carries a significant risk of complications, primarily related to the unique vascularity of the lateral heel and the complexity of the fracture. Understanding these risks and having a management plan is crucial.
Common Complications
| Complication | Incidence (%) | Management Strategy |
|---|---|---|
| Wound Complications | ||
| Skin Necrosis / Dehiscence | 10-30% (higher in smokers, diabetics) | Early identification. Non-operative: serial dressing changes, negative pressure wound therapy (NPWT) for localized necrosis. Operative: debridement, secondary closure, rotational/free flap reconstruction for large defects. |
| Superficial Infection | 5-15% | Oral antibiotics, local wound care, incision and drainage (I&D) if abscess. |
| Deep Infection (Osteomyelitis) | 1-5% | Aggressive surgical debridement (I&D), culture-directed intravenous antibiotics. May require hardware removal (after fracture healing), irrigation, and soft tissue coverage. Long-term suppressive antibiotics. |
| Neurological Complications | ||
| Sural Nerve Injury (Neurapraxia) | 5-20% (often transient) | Reassurance, observation. Physical therapy for desensitization. |
| Sural Nerve Injury (Transection) | <1% (rare with careful technique) | Microsurgical repair if diagnosed acutely. Otherwise, neurolysis or neurectomy for persistent painful neuroma. |
| Tendon Complications | ||
| Peroneal Tendonitis / Impingement | 5-10% | Non-operative: rest, NSAIDs, physical therapy, orthotics. Operative: hardware removal if prominent, peroneal tenolysis, calcaneal osteotomy for impingement, or tendon debridement/repair. |
| Hardware Related Complications | ||
| Prominent / Painful Hardware | 10-25% (often due to plate contouring) | Non-operative: padding, shoe modifications. Operative: hardware removal after fracture consolidation (typically 12-18 months post-op). |
| Hardware Breakage | Rare (indicates nonunion/excessive loading) | Re-evaluation of fracture healing. Revision surgery with bone grafting and more robust fixation if nonunion. |
| Fracture Healing Complications | ||
| Nonunion | <1% (rare in calcaneal fractures) | Revision surgery with debridement, bone grafting, and more stable fixation. |
| Malunion | Up to 20-30% (despite ORIF) | Non-operative: orthotics, shoe modifications. Operative: corrective osteotomy (e.g., lateral wall exostectomy, calcaneal body osteotomy) or subtalar arthrodesis for painful, debilitating malunion, often after 1 year. |
| Post-Traumatic Arthritis | 20-50% (most common long-term complication) | Non-operative: NSAIDs, activity modification, steroid injections, orthotics. Operative: Subtalar arthrodesis for painful, symptomatic arthritis refractory to conservative measures. |
| Other | ||
| Complex Regional Pain Syndrome (CRPS) | 5-10% | Multidisciplinary approach: physical therapy, pain management (nerve blocks, medications), psychological support. Early recognition and aggressive therapy are key. |
| Deep Venous Thrombosis (DVT) / Pulmonary Embolism (PE) | <5% (varies with prophylaxis) | Chemical prophylaxis (LMWH, oral anticoagulants), early mobilization, compression stockings. Treatment with therapeutic anticoagulation for confirmed DVT/PE. |
Salvage Strategies for Major Complications
- Severe Wound Breakdown / Infection: For extensive skin necrosis or persistent deep infection, aggressive surgical debridement is required. This may necessitate repeat debridements, application of NPWT, and ultimately, soft tissue coverage using local rotational flaps (e.g., sural artery flap) or free tissue transfer. In cases of chronic osteomyelitis, hardware removal and long-term antibiotic therapy are often necessary. In the worst-case scenario, particularly in high-risk patients, partial calcanectomy or even below-knee amputation may be considered as a last resort.
- Painful Malunion: Surgical correction for a painful malunion typically involves corrective osteotomies (e.g., lateral wall ostectomy for peroneal impingement, calcaneal body osteotomy for varus/valgus deformity or persistent heel widening) or, more commonly, a subtalar arthrodesis. Arthrodesis fuses the subtalar joint, eliminating motion and pain from arthritis but impacting hindfoot mobility.
- Post-Traumatic Subtalar Arthritis: This is the most common long-term complication. If conservative measures fail to alleviate significant pain and functional limitation, subtalar arthrodesis (fusion) is the definitive surgical salvage procedure. This can be performed open or arthroscopically.
Prevention remains the best strategy, emphasizing meticulous pre-operative planning, appropriate timing of surgery, gentle soft tissue handling, precise reduction, and stable fixation.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following open reduction and internal fixation of calcaneal fractures is a critical determinant of long-term functional outcome. Protocols vary slightly based on surgeon preference, fracture severity, stability of fixation, and patient compliance, but generally follow a phased approach. The primary goals are to protect the repair, manage swelling, restore range of motion, regain strength, and achieve full weight-bearing safely.
Phase 1: Immediate Post-Operative (0-6 Weeks)
Goals:
* Protect surgical repair and wound.
* Control pain and swelling.
* Maintain ankle and foot range of motion (non-weight-bearing).
* Prevent complications (e.g., DVT, pressure sores).
Management:
*
Immobilization:
* Posterior splint or bulky dressing with a well-padded compressive dressing for 1-2 weeks.
* Transition to a removable controlled ankle motion (CAM) boot or cast (fiberglass or plaster) for the remainder of this phase.
*
Weight-Bearing:
Strictly
non-weight-bearing (NWB)
on the operative limb, using crutches or a knee scooter.
*
Elevation:
Continuous elevation of the limb above heart level (especially for the first 1-2 weeks) is crucial to minimize edema and promote wound healing.
*
Cryotherapy:
Regular application of ice packs (20 minutes on, 20 minutes off) to reduce swelling and pain.
*
Pain Management:
Opioids, NSAIDs, nerve blocks as needed.
*
Range of Motion (ROM):
* Start early active and passive ROM for the toes and knee of the operative limb.
* Gentle ankle dorsiflexion/plantarflexion within the limits of the splint/boot, avoiding subtalar motion or excessive inversion/eversion to protect the healing fracture. This may begin around 2-3 weeks post-op, depending on fixation stability.
*
Exercises:
* Isometric quadriceps and hamstring exercises.
* Ankle pump exercises (dorsiflexion/plantarflexion) to promote circulation.
*
Wound Care:
Meticulous wound care, drain removal (typically within 24-48 hours if placed), and suture/staple removal at 2-3 weeks.
Phase 2: Early Mobilization and Protected Weight-Bearing (6-12 Weeks)
Goals:
* Gradual restoration of ankle and subtalar joint ROM.
* Initiate protected weight-bearing.
* Begin strengthening exercises.
Management:
*
Weight-Bearing:
* Typically initiated around 6-8 weeks post-operatively, after radiographic evidence of early fracture healing and clinical assessment of stability.
* Progress from NWB to
touch-down weight-bearing (TDWB)
, then to
partial weight-bearing (PWB)
in the CAM boot, gradually increasing weight as tolerated. Use crutches or a walking frame for support.
*
Immobilization:
Continue CAM boot or an ankle brace during ambulation.
*
ROM Exercises:
* Active and passive ankle ROM exercises (dorsiflexion, plantarflexion, inversion, eversion).
* Gentle subtalar ROM exercises are introduced, emphasizing controlled, pain-free movement.
* Manual therapy by a physical therapist to address joint stiffness and soft tissue tightness.
*
Strengthening:
* Isometric exercises for ankle plantarflexors, dorsiflexors, invertors, and evertors.
* Theraband exercises for all ankle movements.
* Start calf raises (seated, then standing, non-weight-bearing initially).
*
Proprioception:
Begin balance exercises on stable surfaces, such as standing on the affected leg with support.
*
Gait Training:
Focus on proper gait mechanics with protected weight-bearing.
Phase 3: Advanced Strengthening and Return to Activity (12+ Weeks)
Goals:
* Achieve full weight-bearing without assistive devices.
* Restore full strength, endurance, and proprioception.
* Return to functional activities, including light work and recreational sports.
Management:
*
Weight-Bearing:
Progress to
full weight-bearing (FWB)
without assistive devices, typically around 12-16 weeks post-op, assuming good radiographic healing and clinical stability.
*
Immobilization:
Discontinue CAM boot, transition to supportive footwear with good arch support and heel cushioning. Custom orthotics may be beneficial.
*
Strengthening:
* Progress to more advanced resistance exercises (e.g., calf raises with added weight, resistance machine exercises).
* Plyometric exercises and agility drills for athletes (late stage, 4-6 months).
* Single-leg balance exercises on unstable surfaces (e.g., wobble board, foam pad).
*
Functional Training:
* Gait training on various terrains.
* Stair climbing, squatting, lunges.
* Sport-specific drills for athletes.
*
Cardiovascular Fitness:
Resume low-impact activities like swimming or cycling.
*
Monitoring:
Continue to monitor for pain, swelling, and residual stiffness. Address any issues promptly.
*
Return to Activity:
Gradual return to work and recreational activities. High-impact sports are typically not recommended until 6-9 months post-op, and sometimes longer, depending on the fracture severity and healing.
Important Considerations:
*
Individualization:
Rehabilitation must be individualized to the patient's specific fracture pattern, bone quality, soft tissue healing, and functional demands.
*
Pain Guidance:
Progression should always be guided by pain. Any increase in pain or swelling warrants a temporary reduction in activity.
*
Patient Education:
Comprehensive patient education on the expected recovery timeline, potential long-term issues (e.g., post-traumatic arthritis), and the importance of adherence to the protocol is crucial.
*
Potential for Protracted Recovery:
Patients should be counseled that full recovery can take 12-24 months, and some degree of residual stiffness or discomfort is common.
Summary of Key Literature / Guidelines
The surgical management of displaced intra-articular calcaneal fractures, predominantly via the extensile lateral approach, has evolved significantly over the past decades. Key literature and guidelines provide evidence-based recommendations for diagnosis, surgical technique, and post-operative care.
Classification Systems
- Essex-Lopresti (1951): Historically important, describing tongue-type and joint depression-type fractures. This laid the groundwork for understanding the primary displacement patterns.
- Sanders Classification (1993): Based on coronal CT images of the posterior facet, this classification (Types I-IV) is the most widely adopted and guides surgical decision-making. Its prognostic value for surgical outcomes is well-established, with Type II fractures generally having better outcomes than Type III or IV.
- Zwipp Classification (1993): Another comprehensive CT-based system, often used in European literature, providing detailed description of fragments and joint involvement.
Evolution of Surgical Philosophy
Early management often involved non-operative approaches or limited surgical intervention due to high complication rates. However, advancements in surgical technique, internal fixation devices, and a better understanding of fracture biomechanics have shifted the paradigm towards anatomical reduction and stable internal fixation for displaced intra-articular fractures.
- Pioneering work by Benirschke et al. (1993) and Zwipp et al. (1993): Demonstrated improved functional outcomes with anatomical reduction and rigid internal fixation using the extensile lateral approach compared to historical non-operative series. These studies highlighted the importance of restoring articular congruity, calcaneal height, and width.
Timing of Surgery
A consistent theme in the literature emphasizes the critical role of soft tissue status in determining surgical timing.
*
Benirschke et al. (1993):
Advocated for delayed surgery (7-14 days post-injury) to allow for resolution of soft tissue edema, indicated by the "wrinkle sign." Early surgery in the presence of severe swelling is strongly correlated with increased rates of wound complications, including skin necrosis and infection. This principle remains a cornerstone of current practice.
Outcomes and Complications
Despite advancements, calcaneal fractures treated with ORIF still present challenges:
*
Functional Outcomes:
Several studies, including meta-analyses, indicate that ORIF via the ELA generally leads to better functional outcomes (e.g., improved pain scores, functional ankle disability scores, return to work rates) compared to non-operative management for displaced intra-articular fractures, particularly Sanders Type II and selected Type III fractures. However, a significant proportion of patients may still experience residual pain, stiffness, or functional limitations.
*
Post-Traumatic Arthritis:
This remains the most common long-term complication, with rates varying widely (20-50%), often necessitating subtalar arthrodesis. The degree of initial articular comminution and quality of articular reduction are key prognostic factors.
*
Wound Complications:
Rates of wound dehiscence and infection remain a concern, particularly with the ELA, ranging from 10-30%. Risk factors include smoking, diabetes, peripheral vascular disease, and severe soft tissue injury. Careful patient selection and meticulous surgical technique are paramount to mitigate these risks.
Minimally Invasive Approaches vs. Extensile Lateral Approach
Recent literature has explored less invasive alternatives:
*
Sinus Tarsi Approach (STA):
Offers a smaller incision and potentially lower rates of wound complications. It is generally indicated for specific fracture patterns, such as tongue-type fractures, or joint depression fractures with less comminution and good lateral wall integrity (e.g., Sanders Type II with a manageable primary fracture line). The visualization is more limited, making it less suitable for complex, highly comminuted fractures.
*
Percutaneous Fixation:
Utilizes K-wires and cannulated screws. Best suited for non-displaced or minimally displaced fractures, or as an adjunct.
*
Comparative Studies:
A growing body of literature compares the ELA with the STA. While STA may have a lower wound complication rate, some studies suggest ELA may still provide superior anatomical reduction, particularly for complex fractures. The optimal approach depends on the fracture morphology, surgeon expertise, and patient factors. For the majority of displaced intra-articular fractures requiring direct visualization and comprehensive reconstruction, the ELA remains the preferred approach.
Future Directions
Research continues to focus on improving outcomes through:
* Enhanced imaging techniques for better pre-operative planning.
* Development of patient-specific instrumentation and 3D printing for complex reconstructions.
* Improvements in internal fixation devices.
* Better understanding of factors influencing wound healing and infection prevention.
* Refined rehabilitation protocols to optimize functional recovery.
In conclusion, mastering the lateral approach to the calcaneus for fracture repair involves a thorough understanding of calcaneal anatomy and biomechanics, meticulous pre-operative planning, precise surgical execution, and diligent post-operative rehabilitation. While challenges and potential complications exist, a principled approach based on established literature and surgical expertise offers the best chance for optimal patient outcomes.
Clinical & Radiographic Imaging