KNEE Structured oralexamination question6: Anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) reconstruction
EXAMINER : These images belong to a 26-year-old rugby player. He gives a history of falling awkwardly on to his left knee after a heavy tackle. What can you see? (Figure 3.6.)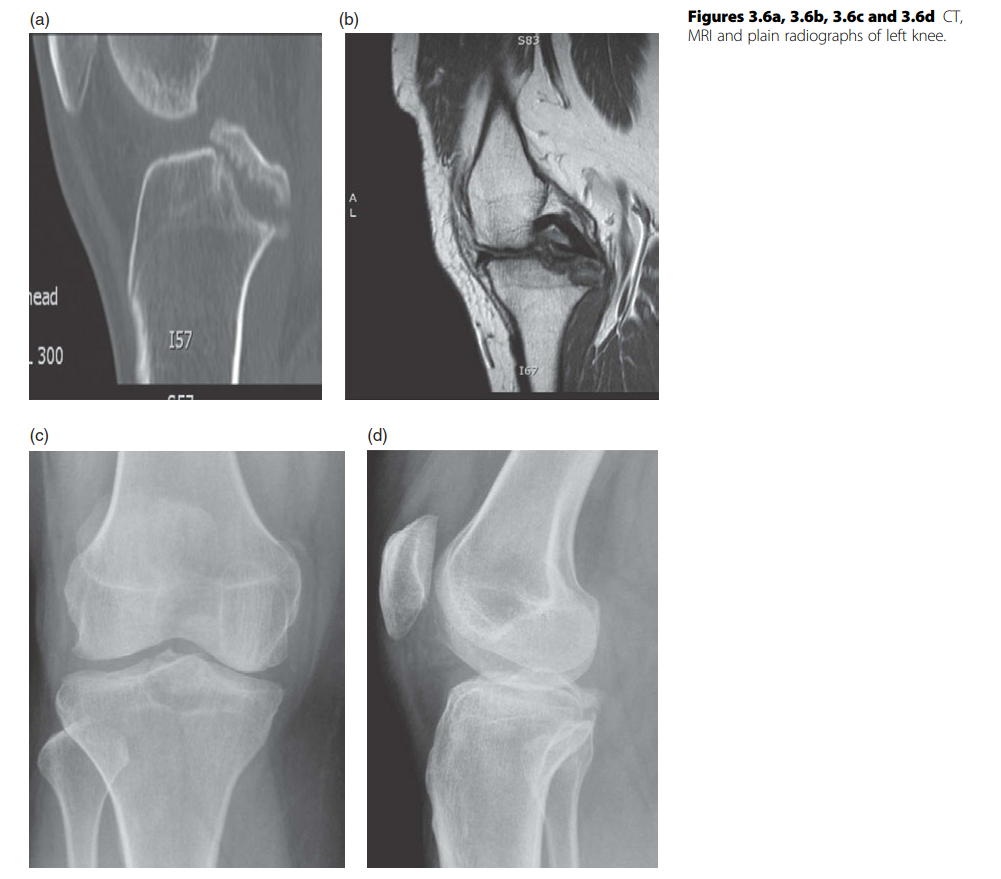
1.30 o’clock ... EXAMINER : Are you sure? (Realizing that the candidate is bluffing.) CANDIDATE : To be honest I have not seen many of these but I will check on it. EXAMINER : Let’s move on. Now tell me about the optimum tunnel placement for single bundle ACL reconstruction. CANDIDATE : The principles of ACL reconstruction are placement of tunnel anatomically and isometrically, using biologically active grafts which are adequately tensioned to allow early rehabilitation. In single-bundle reconstruction, the aim is to place tunnel at the footprint of the posterolateral bundle of ACL. The anteromedial bundle is thought to be the most isometric but most surgeons feel that it’s important to replace the posterolateral bundle. For the femoral tunnel the isometric point lies at about 10 to 10.30 o’clock for right knee and 1.30 to 2 for left knee. The most common mistake is to place femoral tunnel too anterior or ‘resident’s ridge’. This restricts flexion of the knee and may result in elongation of graft. Similarly, too posterior tunnel placement results in excessive tightening of graft when knee is extended. It’s been shown that abnormally narrow intercondylar notch correlates directly with increased incidence of ACL tears. Careful assessment of notch should be done prior to graft insertion using a pin to ensure no impingement on lateral femoral condyle. The presence of impingement with correct placement of tunnels necessitates notchplasty of the anterior portion of lateral femoral condyle. EXAMINER : Which graft would you use and why? CANDIDATE : I would use a hamstring four-strand autograft. The two main biological autografts used in ACL reconstruction are hamstring and bone patella tendon bone (BPTB) graft. The BPTB graft has the advantage of being easy to harvest, rigid fixation and faster integration as it uses bone to bone healing. However, it has donor site morbidity which includes anterior knee pain in 30–50%, patellar tendonitis 3–5%, patellar fracture and patella baja. The hamstring graft on the other hand has less donor site morbidity, can be harvested from a small incision and can be passed relatively easily. However it has slow healing because of tendon to bone incorporation which takes 8 to 12 weeks. It can also result in hamstring weakness and saphenous nerve injury. There are several studies comparing outcome of BPTB versus hamstring graft. Most studies show arthroscopic reconstruction with either graft results in similar functional outcome but increased morbidity in BPTB in form of early OA and increased knee laxity with radiographic femoral tunnel wide in hamstring graft.
Feller JA, Webster KE. A randomized comparison of patellar tendon and hamstring tendon anterior cruciate ligament reconstruction. Am J Sports Med 2003;31:564–573.
Howell SM, Taylor MA. Failure of reconstruction of the anterior cruciate ligament due to impingement by the intercondylar roof. J Bone Joint Surg Am 1993;75-A:1044.
Pinczewski LA, Deehan DJ, Salmon LJ, Russell VJ, Clingeleffer A. A five-year comparison of patellar tendon versus four-strand hamstring tendon autograft for arthroscopic reconstruction of the anterior cruciate ligament. Am J Sports Med 2002;30:523–536.
Debrief: With a thorough understanding of ACL reconstruction, the candidate has recovered from a bad start of this viva. Candidates should be honest and be prepared to say they have not seen some operations.
