PEDIATRIC KNEE FRACTURES: AN ACADEMIC OVERVIEW
Fractures about the knee in the skeletally immature patient represent a complex intersection of pediatric traumatology and sports medicine. Unlike adult fractures, which typically involve catastrophic failure of cortical bone, pediatric knee injuries frequently involve the chondro-osseous junction, physes, and apophyses. The two most clinically significant entities in this domain are patellar fractures—specifically the deceptive "sleeve" fracture—and fractures of the tibial intercondylar eminence.
Mismanagement of these injuries can lead to profound long-term morbidity, including extensor mechanism incompetence, chronic patellofemoral instability, and persistent anterior cruciate ligament (ACL) laxity. This masterclass provides an exhaustive, evidence-based framework for the diagnosis, biomechanical evaluation, and surgical management of these challenging fractures.
PATELLAR FRACTURES IN THE IMMATURE SKELETON
Epidemiology and Pathomechanics
Patellar fractures are exceedingly rare in the pediatric population. Epidemiological data estimates that only 1% of all skeletal fractures occur in the patella, and a mere 1% of these occur in the immature skeleton. Consequently, pediatric patellar fractures are primarily observed in older children and adolescents nearing skeletal maturity.
The pathomechanics of these injuries differ significantly from those in adults. While direct trauma can cause comminuted or stellate fractures, the majority of pediatric patellar fractures are avulsion injuries mediated by eccentric contraction of the quadriceps mechanism against a flexed knee.
Clinical Pearl: Acute lateral dislocation of the patella is a frequent etiology for osteochondral shear fractures, small peripheral avulsions, and sleeve-type fractures in children. Always evaluate for patellofemoral instability when presenting with an acute hemarthrosis and a seemingly isolated patellar fragment.
In the adolescent athlete, chronic repetitive microtrauma to the ligamentous insertions leads to traction apophysitis. Conditions such as "jumper’s knee" and Sinding-Larsen-Johansson syndrome represent chronic avulsion injuries of the proximal and distal poles of the patella, respectively.
Furthermore, systemic and neuromuscular conditions alter the epidemiological profile. Children with cerebral palsy and spasticity of the quadriceps muscle frequently sustain fractures of the distal pole or transverse fractures due to chronic, unyielding tensile forces. Congenital anomalies, such as patellar hypoplasia or absence seen in nail-patella syndrome (onychoosteodysplasia), must also be considered in the differential diagnosis of the dysplastic knee.
The Bipartite Patella: A Diagnostic Pitfall
A critical differential diagnosis in pediatric patellar trauma is the bipartite patella. Often discovered incidentally, it can become symptomatic in adolescent athletes, mimicking an acute fracture.
- Location: Almost exclusively found in the superolateral quadrant.
- Morphology: The edges of the synchondrosis are smooth and rounded, unlike the sharp, jagged radiolucent lines of an acute fracture.
- Incidence: Bilateral in approximately 50% of cases.
The Patellar Sleeve Fracture: A Deceptive Entity
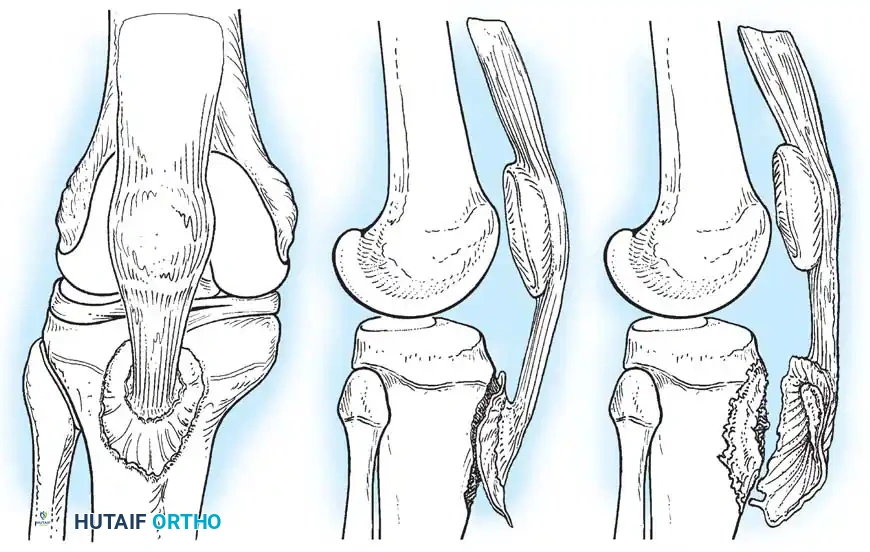
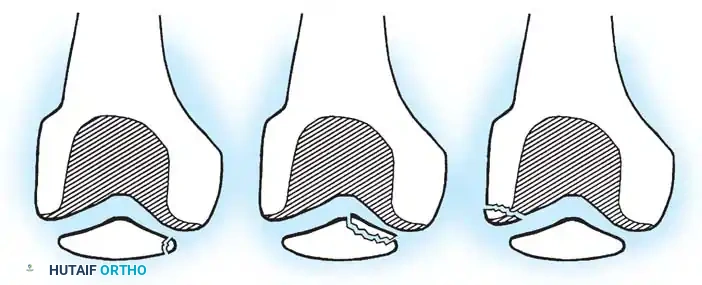
The "sleeve" fracture is a pathognomonic pediatric injury that demands high clinical vigilance. It involves the avulsion of a large cartilaginous envelope (the "sleeve") from the main body of the patella, typically at the distal pole, carrying with it the patellar tendon insertion.
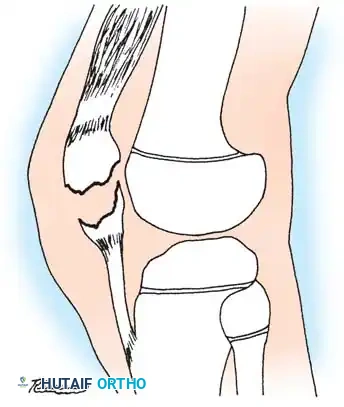
Radiographically, this injury is notoriously deceptive. Because the avulsed fragment is predominantly unossified cartilage, the standard lateral radiograph may only reveal a minute "fleck" of bone. This falsely benign appearance frequently leads to missed diagnoses.

If left untreated, the cartilaginous sleeve continues to generate bone, healing in a malaligned and elongated position. This results in severe patella alta, extensor lag, and an abnormally elongated patellar mechanism. If the initial injury occurred in conjunction with a patellar dislocation, this resultant elongation exacerbates patellofemoral instability, leading to chronic, recurrent dislocations.

Surgical Warning: When a pediatric patient presents with an inability to perform a straight leg raise, a palpable infrapatellar defect, and a high-riding patella, a sleeve fracture must be assumed regardless of how benign the radiograph appears. Magnetic Resonance Imaging (MRI) is the gold standard for delineating the true extent of the cartilaginous avulsion.
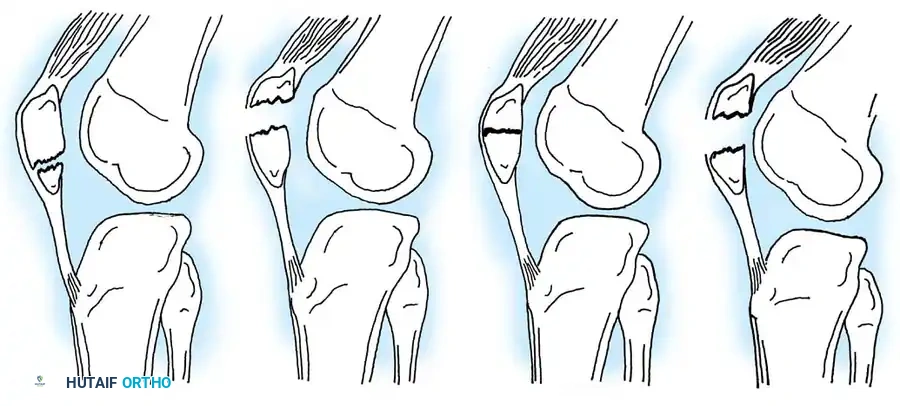
Classification of Patellar Fractures
Patellar fractures in children are classified based on anatomical location, fracture pattern, and the degree of displacement.
In a landmark review by Maguire and Canale of 67 patellar fractures in 66 children (average age 12.4 years), the distribution was as follows:
* Comminuted: 19 fractures
* Transverse: 18 fractures
* Chip/Osteochondral: 15 fractures
* Vertical: 6 fractures
* Sleeve: 2 fractures
Principles of Management
The overarching goal of treatment is the absolute restoration of the extensor mechanism and the preservation of a congruent patellofemoral articulation.
- Non-Operative Management: Reserved strictly for undisplaced fractures with an intact extensor mechanism (patient can actively extend the knee against gravity). Immobilization in a cylinder cast in extension for 4-6 weeks is appropriate.
- Operative Management: Indicated for displaced fractures (>2-3 mm step-off) or any loss of extensor continuity.
- Hardware Considerations: Unlike adults, pediatric patients are prone to hardware prominence, breakage, and potential growth disturbances. It is a standard recommendation to routinely remove wires, pins, and screws after radiographic union is achieved, preferably before hardware failure occurs.
- Patellectomy: Total patellectomy is rarely indicated but may be considered for severely displaced, highly comminuted fractures without ipsilateral tibial or femoral fractures. However, every effort should be made to preserve the patella to maintain the mechanical advantage of the quadriceps.
Surgical Technique: Open Reduction and Internal Fixation of Sleeve Fractures (Houghton and Ackroyd)
Because the sleeve fracture involves a massive cartilaginous fragment attached to a small osseous fleck, closed reduction is impossible. Open anatomical reduction is mandatory.
1. Positioning and Preparation
* Place the patient supine on a radiolucent operating table.
* Apply a proximal thigh tourniquet.
* Prepare and drape the limb in a standard sterile fashion, allowing for full flexion and extension of the knee.
2. Surgical Approach
* Utilize a 7-cm medial parapatellar incision, focusing on the distal portion to expose the inferior pole of the patella and the patellar tendon.
* Incise the retinaculum longitudinally to expose the fracture hematoma.
3. Debridement and Reduction
* Irrigate the fracture site copiously with sterile saline.
* Use a small curette to meticulously remove organized hematoma, interposed periosteum, and loose cancellous debris.
* Reduce the cartilaginous sleeve fragment to the main body of the patella using a small, pointed bone reduction forceps.
* Crucial Step: Assess the reduction not only on the anterior cortical surface but also on the posterior articular surface. If direct visualization is obscured, insert a gloved finger into the joint to palpate the articular cartilage, ensuring no step-off or angulation exists.

4. Internal Fixation (Tension Band Principle)
* Drive two parallel, longitudinal Steinmann pins (or heavy Kirschner wires) from distal to proximal across the fracture site.
* Leave the pins protruding approximately 0.5 cm (1/4 inch) distally to facilitate future removal.
* Pass a flexible stainless-steel wire (18- or 20-gauge, depending on patient size) transversely through the insertion of the quadriceps tendon at the superior pole.
* Pass the wire distally, crossing it in a figure-of-eight fashion over the anterior surface of the patella.
* Pass the wire deep to the protruding Steinmann pins at the inferior pole.

- Tighten the tension band wire symmetrically. The tension band converts the tensile forces of the quadriceps into compressive forces at the articular surface during knee flexion.
- Pitfall: Do not overtighten the wire, as this can cause anterior gaping and posterior articular angulation of the cartilaginous fragment.

5. Closure and Postoperative Care
* Repair the medial and lateral retinacular tears meticulously with absorbable sutures to restore the secondary restraints of the extensor mechanism.
* Close the subcutaneous tissues and skin.
* Apply a well-padded cylinder cast or long-leg cast with the knee in mild flexion (5-10 degrees) to prevent stiffness in hyperextension.
* Aftertreatment: The cast is removed at 3 to 4 weeks, and progressive range-of-motion exercises are initiated. While the AO foundation advocates for immediate motion following tension band wiring in adults, a brief period of immobilization is preferred in young children to protect the delicate chondral repair.
FRACTURES OF THE TIBIAL INTERCONDYLAR EMINENCE
Biomechanics and Pathoanatomy
Fractures of the tibial intercondylar eminence (tibial spine) are the pediatric equivalent of a mid-substance Anterior Cruciate Ligament (ACL) rupture. Because the pediatric ligaments are biomechanically stronger than the adjacent physeal and chondro-osseous structures, applied tensile forces result in an avulsion of the bony attachment rather than a tear of the ligament itself.
The mechanism of injury typically involves forced hyperextension of the knee, often combined with valgus or varus rotational stress—commonly seen in bicycle accidents or contact sports.
The Controversy of Residual Laxity:
Historically, it was believed that anatomical reduction of the bony fragment resulted in a perfectly stable knee. However, modern literature demonstrates that the ACL undergoes significant plastic deformation (interstitial stretching) prior to the bony avulsion.
* Baxter and Wiley reported that 51% of patients had a positive anterior drawer test at long-term follow-up, alongside a measurable loss of terminal extension (4 to 15 degrees).
* Willis et al. utilized KT-1000 arthrometer testing and found objective evidence of laxity in 74% of patients. Interestingly, only 10% complained of subjective pain, and none reported functional instability.
* Grönkvist et al. suggested that while younger children may compensate for this anterior instability through skeletal growth and neuromuscular adaptation, older adolescents often experience persistent, symptomatic instability requiring rigorous rehabilitation or delayed reconstruction.
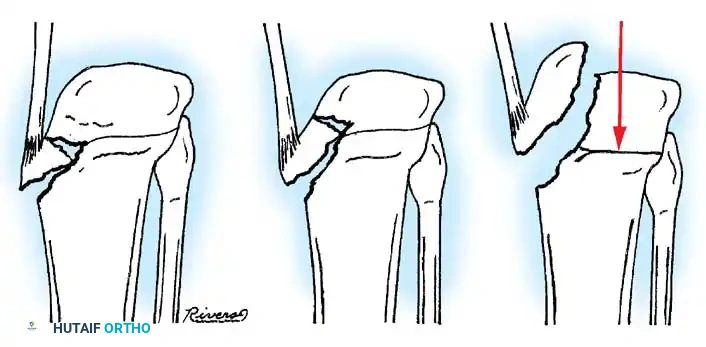
Classification (Meyers and McKeever)
The management of tibial eminence fractures is dictated by the Meyers and McKeever classification system, which assesses the degree of displacement and the presence of a cartilaginous hinge.
- Type I: Non-displaced or minimally displaced fracture. The bony fragment rests in its anatomical bed.
- Type II: The anterior portion of the eminence is elevated and displaced proximally, but an intact cartilaginous hinge remains posteriorly. The fragment resembles a bird's beak.
- Type III: Complete displacement of the fragment with no cortical or cartilaginous continuity. The fragment may be rotated.
- Type IV (Zaricznyj modification): Comminuted fracture of the eminence.
Clinical Evaluation and Blocks to Reduction
Patients present with an acute, tense hemarthrosis, severe pain, and an inability to bear weight. Aspiration of the hemarthrosis (yielding fat globules from the marrow space) provides significant pain relief and allows for a more accurate clinical examination.
Clinical Pearl: The most significant complication of a displaced tibial eminence fracture is not anterior instability, but rather a mechanical block to terminal extension. The displaced fragment impinges against the intercondylar notch of the femur.
Meniscal Entrapment:
A critical factor in the failure of closed reduction is the interposition of soft tissue beneath the avulsed fragment. Kocher et al., in a review of 80 skeletally immature patients, identified entrapment of the anterior horn of the medial meniscus, the intermeniscal ligament, or the anterior horn of the lateral meniscus in:
* 26% of Type II fractures.
* 35% of Type III fractures.

Because of this high rate of soft-tissue interposition, forceful attempts to reduce Type III fractures by simply extending the knee are contraindicated, as this can further crush the entrapped meniscus.
Surgical Management: Open and Arthroscopic Techniques
Non-Operative Management (Type I and Reducible Type II):
Aspirate the tense hemarthrosis under sterile conditions. Apply a long-leg cast or cylinder cast with the knee in full extension (or slight hyperextension, if tolerated) to utilize the femoral condyles to compress the fragment into its bed. Immobilize for 4 to 6 weeks.
Operative Management (Irreducible Type II and Type III):
If closed reduction fails to achieve an anatomical reduction (assessed via plain radiographs or MRI), operative intervention is mandatory to remove the entrapped soft tissue and secure the fragment.

Open Reduction and Internal Fixation (Physeal-Sparing Technique)
While arthroscopic techniques are increasingly popular, open reduction remains a highly reliable, time-tested method, particularly in smaller children where arthroscopic instrumentation may be challenging.
- Approach: Utilize a medial parapatellar incision to expose the intercondylar notch, the ACL, and the anterior horns of both menisci.
- Debridement: Inspect the fracture bed. Retract the entrapped anterior horn of the medial meniscus or the transverse intermeniscal ligament using a nerve hook. Clear the fracture crater of hematoma and small osseous debris.
- Reduction: Anatomically reduce the tibial eminence fragment into its crater.
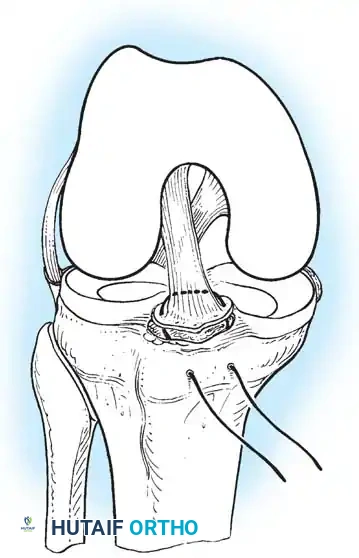
- Fixation: To avoid crossing the proximal tibial physis with rigid hardware (which could cause growth arrest or angular deformity), suture fixation is preferred.
- Pass a heavy, nonabsorbable suture (e.g., #2 FiberWire or Ethibond) through the most distal, robust portion of the ACL substance, just proximal to the bony fragment.
- Using an ACL drill guide, drill two parallel 2.0 mm tunnels from the anteromedial tibial metaphysis, aiming directly into the fracture crater. Crucial: Ensure the drill path remains entirely within the epiphysis if possible, or crosses the physis centrally and vertically to minimize the risk of growth arrest.

* Retrieve the suture limbs through the drill holes.
* Tie the sutures securely over a bony bridge on the anteromedial tibia while holding the knee in 20 degrees of flexion and applying posterior translation to the tibia to tension the ACL.
Arthroscopic-Assisted Reduction
Arthroscopic techniques offer the advantage of minimal morbidity and excellent visualization of the joint space. Fixation can be achieved via:
* Fracture-based methods: Antegrade cannulated screws (only if the fragment is large enough and the patient is nearing skeletal maturity, avoiding the physis).
* Ligament-based methods: Retrograde suture passage using suture passers (e.g., Lasso) through the base of the ACL, shuttled through trans-epiphyseal drill holes, and tied over the anterior tibia.
Postoperative Rehabilitation and Outcomes
Postoperatively, the knee is immobilized in a hinged brace locked in extension for 2 to 4 weeks to protect the repair. Progressive range of motion is then initiated, focusing on achieving full terminal extension. Weight-bearing is restricted for 4 to 6 weeks until radiographic union is evident.
Despite anatomical reduction and rigid fixation, surgeons must counsel parents that objective ACL laxity is a common long-term finding due to the initial plastic deformation
