Introduction to Intramedullary Nail Fixation
Since its popularization in the mid-1950s by Gerhard Küntscher, intramedullary nail fixation has revolutionized the management of long bone fractures, gaining universal acceptance as the gold standard of care. Today, closed interlocking intramedullary nail fixation is the definitive procedure of choice for femoral and tibial shaft fractures. This is particularly true in polytrauma patients managed in Level I trauma centers, where rapid stabilization is critical for systemic resuscitation.
Historically, the method was the subject of intense controversy. Early critics raised valid concerns regarding the destruction of the endosteal medullary circulation, the potentially fatal risk of marrow fat embolism, and catastrophic hardware failures stemming from a poor understanding of the implant's biomechanical limits. However, rigorous scientific investigation and decades of clinical refinement have systematically addressed these concerns. Modern intramedullary nailing—characterized by advanced titanium and stainless steel alloys, anatomically contoured designs, and sophisticated interlocking mechanisms—now provides unparalleled biomechanical stability while respecting the biological envelope of the fracture.
Clinical Pearl: The primary biological advantage of closed intramedullary nailing is the preservation of the fracture hematoma and the periosteal blood supply. By avoiding wide surgical exposures, the surgeon minimizes soft tissue stripping, thereby optimizing the physiological environment for secondary bone healing via callus formation.
Biomechanics of Intramedullary Nailing
To master intramedullary nail fixation, the orthopedic surgeon must possess a profound understanding of its underlying biomechanical principles. Unlike plates, which act as load-bearing devices placed eccentrically on the tension band surface of the bone, intramedullary nails are centrally located load-sharing devices. Their position within the neutral axis of the bone minimizes the bending moments subjected to the implant, significantly reducing the risk of fatigue failure.
Load Sharing vs. Load Bearing
Satisfactory stabilization depends heavily on the fracture pattern and the degree of cortical contact.
In fractures with transverse or short oblique patterns where cortical contact is restored, the rod and the bone share the axial and bending loads (load sharing). This physiological stress transfer stimulates osteoblastic activity and promotes robust union.
Conversely, in cases of severe comminution or segmental bone loss, the intramedullary rod alone must support the entirety of the bending and axial loads. In these scenarios, the implant acts temporarily as a load-bearing device, increasing the risk of hardware failure if union is delayed.
Curvature Mismatch and Interference Fit
The anatomical curvature of the bone must be meticulously considered when selecting the nail type and determining the necessary degree of medullary reaming. Biomechanically, unlocked nails attain stability through a "curvature mismatch" between the rigid nail and the natural bow of the bone (e.g., the anterior bow of the femur). This mismatch induces a longitudinal interference fit, providing three-point fixation.
If the curvature mismatch is substantial, aggressive reaming is required to accommodate the nail without causing an iatrogenic fracture. However, excessive reaming must be avoided, as it significantly weakens the diaphyseal cortex and increases the risk of thermal necrosis to the bone.
Rotational and Axial Control
Unlocked nails can only be considered when a noncomminuted fracture occurs precisely through the narrowest part of the medullary canal (the isthmus). In this highly specific scenario, the tight interference fit eliminates side-to-side shearing forces and adequately controls rotational forces.
However, if the medullary canal is significantly larger in one fragment than the other—such as in metaphyseal fractures—poor control of rotational forces is inevitable. In these situations, interlocking techniques are an absolute requirement. Axially unstable fractures (spiral, comminuted, or segmental) must be treated with static or double-locked nails to prevent shortening and malrotation.
Types of Intramedullary Nails
Intramedullary nails are categorized by their anatomical entry points and functional designs. Selecting the appropriate nail is the first critical step in preoperative planning.
Centromedullary Nails
Centromedullary nails enter the bone in direct line with the medullary canal. They obtain contact with the bone through multiple points of longitudinal interference and depend heavily on the restoration of bony contact to avoid axial and rotational deformation.
* Examples: The classic Küntscher cloverleaf nail and the Sampson nail. While historically significant, pure centromedullary unlocked nails are rarely used today due to the superiority of interlocking designs.
Condylocephalic Nails
These nails enter the bone in the condyles of the metaphysis and are driven proximally into the opposite metaphyseal-epiphyseal area. They are frequently inserted in clusters to provide added rotational stability through a divergent spread.
* Examples: Ender pins and Hackenthall pins. These are largely historical but may occasionally be used in pediatric orthopedics (elastic stable intramedullary nailing - ESIN).
Cephalomedullary Nails
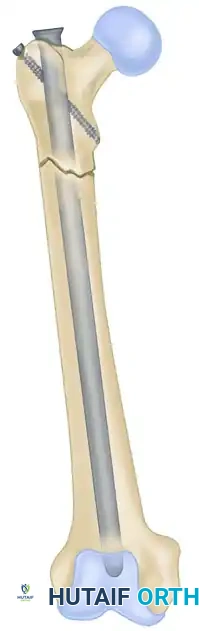
Cephalomedullary nails feature a centromedullary diaphyseal portion but include specialized proximal geometry that permits robust screw fixation up into the femoral head and neck. They are the implant of choice for subtrochanteric fractures and ipsilateral femoral neck/shaft fractures.
* Examples: The Küntscher Y-nail, the Zickel subtrochanteric nail, and modern proximal femoral nails (PFNA, Gamma nails).
Preoperative Planning and Patient Selection
Intramedullary fixation is not a technique to be utilized casually. Complications can be catastrophic if the procedure is misapplied. The following considerations are mandatory:
- Radiographic Templating: Adequate preoperative planning requires orthogonal radiographs of the entire bone, including the joints above and below. The surgeon must ensure the fracture can be adequately stabilized within the "working zone" of the nail. Nails of suitable length and diameter must be identified before the patient enters the operating room.
- Physiological Tolerance: The patient must be hemodynamically stable enough to tolerate a major surgical procedure. In polytrauma patients, the principles of Damage Control Orthopedics (DCO) versus Early Total Care (ETC) must be weighed.
- Pulmonary Status: Special consideration must be given to patients with severe pulmonary injuries (e.g., bilateral pulmonary contusions). The added burden of marrow fat emboli generated during canal reaming and nail insertion may precipitate Adult Respiratory Distress Syndrome (ARDS).
- Operating Room Setup: Suitable instrumentation, a radiolucent fracture table (or flat table for manual traction), highly trained assistants, and high-quality fluoroscopy (C-arm) are absolute prerequisites.
Surgical Warning: A metal nail is not a substitute for biological union. It will inevitably bend or break if subjected to undue strain during convalescence, particularly in the presence of a nonunion or segmental defect.
Surgical Technique: Step-by-Step Principles
1. Positioning and Reduction
Closed nailing techniques should be utilized whenever possible to preserve the fracture hematoma. The patient is typically positioned supine or in the lateral decubitus position on a fracture table. Traction is applied to restore length, while gross rotational and angular alignment is corrected under fluoroscopic guidance.
In simple fracture patterns, closed reduction is often achieved via longitudinal traction. The nail is passed across the fracture site, and proximal locking is performed to secure the implant.
2. The Entry Portal
The entry portal is the most critical step in the procedure. An eccentric starting point will dictate the trajectory of the nail, leading to iatrogenic malalignment or cortical blowout.
* Femur: The traditional entry point is the piriformis fossa, which is perfectly in line with the central axis of the medullary canal. Alternatively, a greater trochanteric entry point can be used with specifically designed trochanteric-entry nails (which feature a proximal lateral bend).
* Tibia: The offset between the entry portal (extra-articular, proximal tibia) and the alignment of the canal introduces strong forces on the posterior cortex. Starting the nail high and at the level of the fibular head, just medial to the lateral tibial spine, minimizes these insertional forces and prevents apex-anterior (procurvatum) deformities.
3. The Reamed vs. Unreamed Controversy
A continuing controversy in the management of long bone fractures, particularly in multiply injured patients, is whether to ream the medullary canal prior to nail insertion.
The Case for Unreamed Nailing:
Proponents of unreamed nailing emphasize the adverse physiological effects of reaming. The reamer acts as a piston, driving intramedullary pressures to extreme levels and forcing bone marrow fat into the venous circulation, leading to pulmonary embolization. Experimental evidence suggests that reaming transiently impairs pulmonary function. However, in modern clinical practice, this adverse effect is rarely clinically significant in isolated fractures. The development of pulmonary complications is more closely related to the initial severity of the chest trauma than to the act of medullary reaming itself.
The Case for Reamed Nailing:
Studies supporting reamed nailing consistently report higher union rates, faster times to union, and lower rates of implant failure. Reaming allows for the insertion of a larger diameter, biomechanically superior nail. Furthermore, the reamings themselves act as an autologous bone graft, depositing osteoprogenitor cells directly at the fracture site.
Infection Rates in Open Fractures:
Historically, reaming in the presence of an open fracture was feared to spread contamination throughout the canal. However, current clinical data demonstrate no statistical difference in infection rates between reamed and unreamed femoral nailing.
* Clinical Evidence: In a robust series of 125 open femoral fractures treated with either reamed (95 fractures) or unreamed (30 fractures) nailing, the overall infection rate was 4%. Specifically, infection developed in 3.2% of the reamed group and 6.4% of the unreamed group. Similarly, in 50 open tibial fractures treated with unreamed nailing, the infection rate was 8%, all of which were severe Gustilo-Anderson Type III injuries. Therefore, reaming remains safe and highly effective, even in the majority of open fracture scenarios, provided adequate surgical debridement is performed.
4. Managing Metaphyseal Fractures: Poller Screws
Locked intramedullary nailing techniques have evolved to allow the fixation of fractures within 2 to 4 cm of the articular joint line. However, the wide metaphyseal canal offers no cortical interference fit, leading to a high risk of "bell-clappering" (translation and angular deformity) of the nail within the wide segment.
To counteract this, surgeons utilize blocking screws, commonly known as "Poller" screws. These screws are placed extra-medullarly (outside the nail but inside the bone) in the wide metaphyseal fragment. They artificially narrow the medullary canal, directing the nail into the correct trajectory and providing a rigid fulcrum that prevents angular deformity.
5. Interlocking Configurations: Static vs. Dynamic
Generally, interlocking screws should be positioned at least 2 cm from the fracture line to provide sufficient stability while allowing functional activity postoperatively.

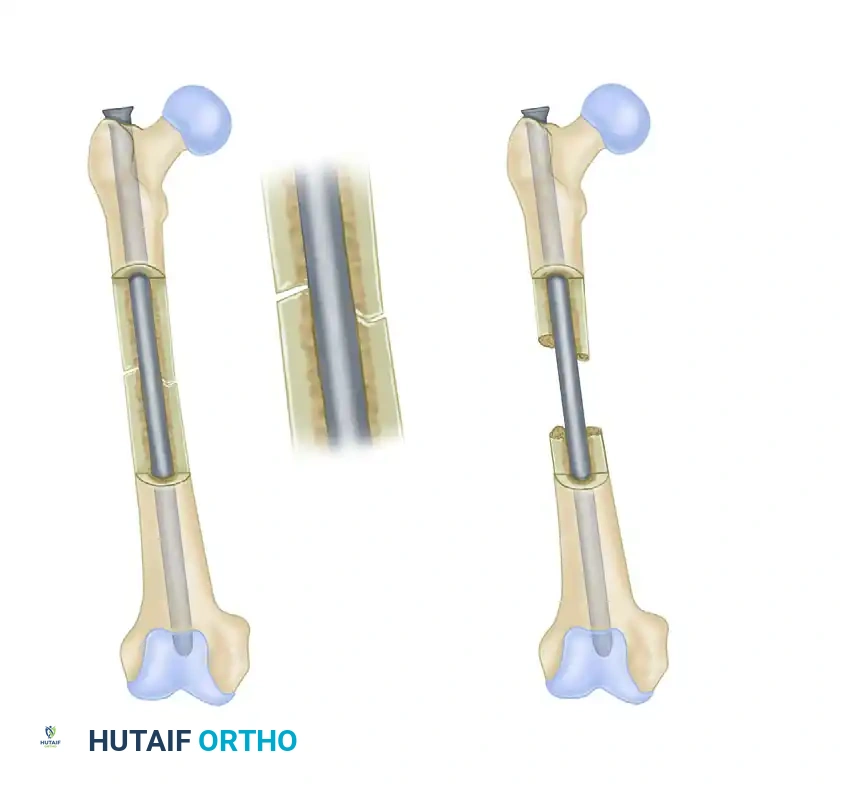
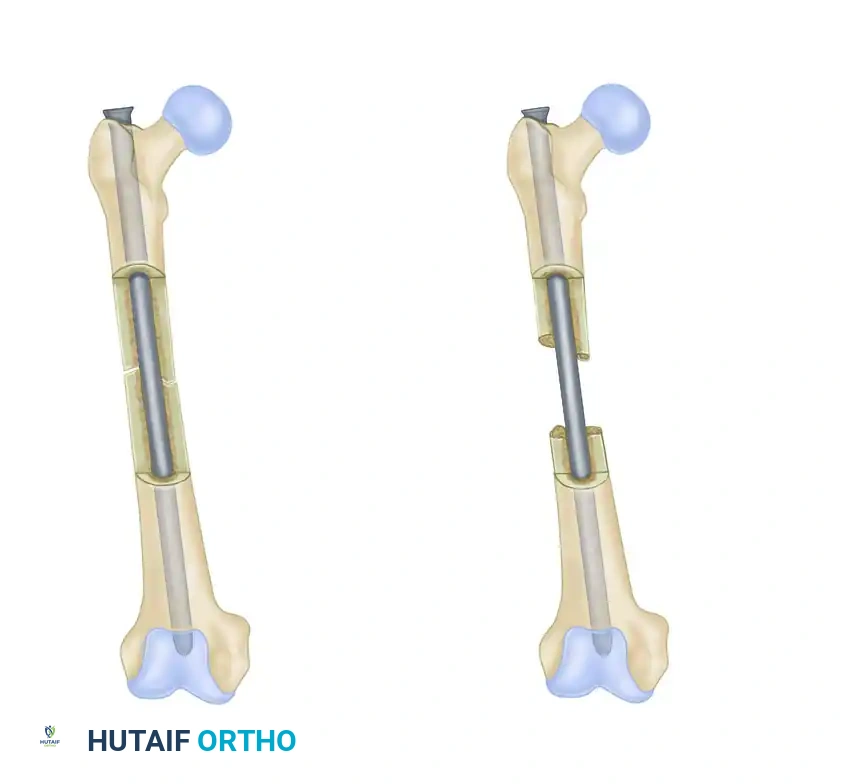
FIGURE 53-36: Dynamic (A) and static (B) locking of an intramedullary nail. Dynamic locking allows for controlled axial compression, whereas static locking rigidly controls both length and rotation.
- Static Locking: Involves placing screws in round holes at both the proximal and distal ends of the nail. This configuration locks the bone to the nail entirely, preventing any axial shortening or rotational movement. It is mandatory for comminuted, spiral, or bone-loss fractures where maintenance of limb length is critical.
- Dynamic Locking: Involves placing a screw through a slotted hole at one end of the nail, allowing the bone fragment to slide axially along the nail while still preventing rotation. This allows contact-compression forces to impact the fracture surfaces during weight-bearing—a highly desirable physiological stimulus for bone union. Dynamization can be performed as a secondary procedure (removing static screws to allow a slotted screw to slide) if delayed union is observed.

In highly comminuted fractures, static locking with multiple distal and proximal screws is essential to maintain length and prevent rotational collapse during the early phases of healing.
Postoperative Protocols and Complications
Rehabilitation
The postoperative protocol is dictated by the fracture pattern and the stability of the fixation. For transverse or short oblique fractures treated with a statically locked, reamed nail, immediate weight-bearing as tolerated is often permissible. The axial load stimulates the piezoelectric effect in bone, accelerating callus formation. In severely comminuted fractures, partial weight-bearing may be instituted until early bridging callus is visible on radiographs (typically 4 to 6 weeks).
Hardware Removal
A perfect intramedullary nail should be constructed so that it is accessible for easy removal once the fracture has consolidated. Modern nails feature proximal internal threads to accommodate extraction devices. Routine removal of intramedullary nails is not recommended unless the patient experiences symptomatic hardware irritation (e.g., prominent proximal locking screws causing iliotibial band friction) or in the setting of deep infection.
Complications
Despite its status as the gold standard, complications can occur:
1. Malunion: Most commonly rotational malalignment or angular deformity in proximal/distal third fractures.
2. Nonunion: Often requires secondary interventions such as dynamization, exchange nailing (removing the nail, reaming the canal larger, and inserting a thicker nail), or bone grafting.
3. Iatrogenic Fracture: Can occur during entry portal creation, aggressive reaming, or forceful nail insertion in a mismatched canal.
4. Infection: Deep medullary infection is a devastating complication requiring hardware removal, aggressive intramedullary reaming/irrigation (Reamer-Irrigator-Aspirator systems), and placement of antibiotic-impregnated cement nails.
Conclusion
Intramedullary nail fixation represents the pinnacle of biomechanical and biological synergy in orthopedic trauma surgery. By respecting the soft tissue envelope, acting as a load-sharing device, and allowing for early mobilization, it provides the optimal environment for fracture healing. Mastery of this technique requires meticulous preoperative planning, a deep understanding of medullary anatomy, and strict adherence to the biomechanical principles of reaming, entry portal selection, and interlocking screw configuration. As implant designs and surgical techniques continue to evolve, the indications for intramedullary nailing will only continue to expand, further minimizing the need for open reduction in complex long bone trauma.
