Intramedullary Fixation of Forearm Shaft Fractures
DEFINITION
Forearm shaft fractures represent the third most common fracture encountered in the pediatric population. 5Closed fracture care is successful in the large majority of children who sustain forearm shaft fractures (especially the common greenstick fracture pattern). 4For children who are 8 to 10 years of age and older with complete fracture patterns, the limits of acceptable displacement (angulation, rotation, and translation) become more strict and the likelihood of surgical intervention increases. 1,13
ANATOMY
The forearm represents a largely nonsynovial, two bone joint with a high-amplitude range of motion (roughly 180 degrees). In the fully supinated anteroposterior (AP) plane, the radius bows naturally out and away from the relatively straight ulna, whereas both bones are predominantly straight in the lateral plane.Anatomically, the shaft of the radius extends from the most proximal aspect of the tubercle of Lister (which approximates the distal metaphyseal-diaphyseal junction) to the proximal base of the bicipital tuberosity. The shaft of the ulna corresponds to these same points on the radius ( FIG 1).11,13In unfractured bones, the normal orientation of the radial styloid and bicipital tuberosity is slightly less than 180 degrees from one another, whereas the ulnar styloid and coronoid process come closer to a true 180-degree relationship.Classically, forearm shaft fractures are divided into distal third (pronator quadratus region), central third (pronator teres region), and proximal third (biceps and supinator region). These anatomic relationships offer insight into the deforming forces acting on the fractured forearm ( FIG 2).
PATHOGENESIS
Forearm shaft fractures most commonly occur secondary to a fall on an outstretched arm and usually involve both bones. Forward falls tend to involve a pronated forearm, and backward falls involve a supinated forearm.Single-bone forearm shaft fractures should raise significant suspicion regarding the presence of a Galeazzi or Monteggia-type injury (see Chap. 11).Mechanisms of injury that involve little rotational force result in forearm fractures at nearly the same levels, whereas greater rotational force results in fractures at rather different levels.
NATURAL HISTORY
The remodeling potential of the pediatric forearm shaft has been well documented and is considered to be most predictable in children younger than about 8 to 10 years of age.Spontaneous correction and improvement of malaligned shaft fractures are considered to occur in young children via three mechanisms:Adjacent physes produce “straight bone” via normal growth.Physeal orientation tends to “right its horizon” via the Hueter-Volkmann law. 12 True shaft remodeling occurs via Wolff law.15
PATIENT HISTORY AND PHYSICAL FINDINGS
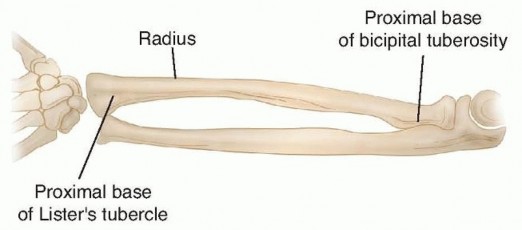
FIG 1 • The radial diaphysis extends from the most proximal aspect of the tubercle of Lister to the proximal base of the bicipital tuberosity. The ulnar diaphysis corresponds to these same points on the radius.
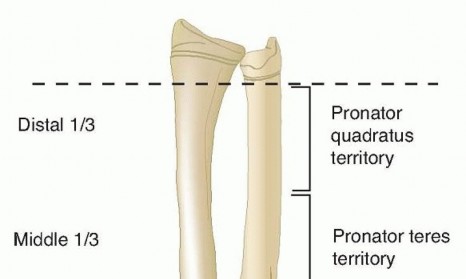
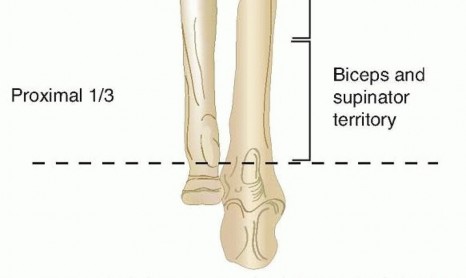
FIG 2 • Forearm shaft fractures are divided into distal third (pronator quadratus region), central third (pronator teres region), and proximal third (biceps and supinator region). It has been said that you need only a thumb to test the motor function of all three major nerves: radial nerve = extensor pollicis longus, ulnar nerve = adductor pollicis, median nerve = opponens pollicis.Peripheral nerves in the fractured extremity are assessed with the “rock-paper-scissors” method.The radial nerve (really the posterior interosseous nerve in the forearm) is tested with “paper”—extension of the fingers and wrist well above a zero-degree wrist position. The autonomous zone is the dorsal web space between the thumb and index finger. There is a risk of iatrogenic injury during surgical exposure of the proximal radial shaft.The ulnar nerve is tested with “scissors”—adducted thumb, abducted fingers, and flexor digitorum profundus function to ring and pinky. The autonomous zone is palmar tip pinky finger. This is the most common iatrogenic nerve injury after internal fixation of forearm shaft fractures.The median nerve is tested with “rock.” The autonomous zone is palmar tip index finger. The median is the most commonly injured nerve after closed or open forearm shaft fractures.The anterior interosseous nerve is tested with the “okay” sign. Flexion of the distal interphalangeal of the index finger and the interphalangeal of the thumb herald flexor digitorum profundus and flexor pollicis longus function of these digits. This is a motor branch only (it has no cutaneous innervation, only articular). Isolated palsy has been reported secondary to constrictive dressings and after proximal ulnar fracture.
IMAGING AND OTHER DIAGNOSTIC STUDIES

FIG 3 • AP (A) and lateral (B) radiographs of a boy age 9 years and 11 months with a forearm shaft fracture.
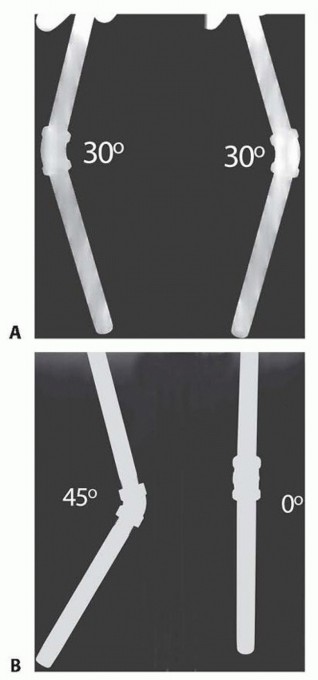
FIG 4 • A. Out-of-plane AP and lateral views of a 45-degree angulated iron pipe. B. True AP and lateral views of the same pipe. Table 1 Practical Classification of Forearm Shaft Fractures Bones: Single-bone fractures occur but both-bone injuries predominate. Radius Ulna Level: Fracture level has bearing on nonoperative versus operative decision making. Distal third Middle third Proximal third Pattern: Fracture pattern has bearing on nonoperative versus operative decision making. Bow (also known asplastic deformation) GreenstickComplete Comminuted
DIFFERENTIAL DIAGNOSIS
Galeazzi injury (concomitant distal radioulnar joint disruption) Monteggia injury (concomitant proximal radioulnar joint disruption)Coexisting distal humeral fracture (eg, supracondylar humeral fracture, also known asfloating elbow) Open fracture (the clinician must be beware of small, innocuous-appearing wounds)Compartment syndrome (more common in setting of floating elbow and extended efforts at indirect reduction of difficult to reduce fractures) 3
NONOPERATIVE MANAGEMENT
Nonoperative (closed) fracture management is used in the vast majority of pediatric forearm shaft fractures. 4Successful nonoperative treatment requires an eclectic mix of anatomic knowledge, skillful application of reduction techniques, appreciation for remodeling potential, and respect for the character of the soft tissue envelope.Greenstick fracture patterns retain a degree of inherent stability; intentional completion of these fractures isnotrecommended. Davis and Green7 reported a 10% loss of reduction rate with greenstick fractures and a 25% rate with complete fractures.Greenstick fracture patterns often involve variable amounts of rotational deformity such that when the forearm is appropriately derotated, reduction of angulation occurs simultaneously.Apex volar greenstick fractures are considered to represent supination injuries that require a relative degree of pronation to effect reduction.Apex dorsal greenstick fractures are considered to be pronation injuries that require supination to aid reduction.Classic finger-trap and traction reduction techniques are probably best reserved for complete both-bone fracture patterns. When dealing with complete both-bone shaft fractures, respect should be paid to the level of the fractures when choosing a relatively neutral, pronated, or supinated forearm position.Price et al 14 has suggested that estimated rotational malalignment should not exceed 45 degrees. The related concepts of maintenance of an appropriate amount of radial bow and interosseous space on the AP radiograph must also not be forgotten, but precise criteria do not exist at this time.Initial above-elbow cast immobilization is the rule for all forearm shaft fractures, as this appropriately controls pronation-supination as well as obeying the orthopaedic maxim of immobilizing the joints above and below the fracture. An extra benefit of above-elbow immobilization relates to the activity limitation it imposes; in some instances, this may increase the chances of maintaining a satisfactory reduction in an otherwise very activecustomer.
SURGICAL MANAGEMENT
Flexible intramedullary nail treatment of pediatric forearm shaft fractures focuses predominantly on displaced complete fractures, many of which may have minor comminution (butterfly fragments usually <25% of a shaft diameter).When efforts at closed fracture management do not achieve and maintain fracture reduction within accepted guidelines, surgical treatment is indicated.When complete fractures occur in children younger than about 8 to 10 years of age with angulation of at least 20 degrees in the distal third, 15 degrees in the central third, or 10 degrees in the proximal third, risk-benefitdiscussions are appropriate regarding further efforts at fracture reduction and possible internal fixation. 8,17Lesser measured angulation associated with significant forearm deformity (as defined in a discussion between the orthopaedic surgeon and the parents) may also prompt intervention in selected children.Complete forearm shaft fractures in children older than 8 to 10 years of age should be evaluated very criticallywith the intention to accept no more than 10 degrees of angulation at any level. 8,17 Compromise (loss) of interosseous space should also be considered as well as rotational malalignment (difficult to assess precisely) when debating the merits of continued cast treatment versus flexible intramedullary nail fixation.Single bone fixation of pediatric forearm shaft fractures has been described by some authors but isnotadvocated due to increased risk of redisplacement.6
PREOPERATIVE PLANNING


FIG 5 • My preferred operating room setup, with the injured arm on the radiolucent hand table and the C-arm properly positioned.
POSITIONING
The patient is placed in a supine position on the operating room table with the involved extremity positioned on a sturdy hand table to allow easy, unobstructed radiographic visualization of the entire forearm ( FIG 5).In general, the monitor for the portable fluoroscopy unit should be positioned near the end of the operating table, opposite the imaging unit (C-arm).A nonsterile tourniquet may be applied about the upper arm (near the axilla) before preparation and draping, but it isnotroutinely inflated.The limb is appropriately prepared and draped, with care being taken to ensure that the first layer is a sterile impervious one (eg, blue plastic U-drape). The C-arm is also appropriately protected with a C-arm sterile plastic drape and an additional sterile skirt (usually a sterile paper half-sheet). Without this sterile skirt, certain limb positions and certain surgical maneuvers occur far too close to nonsterile territory.
APPROACH


FIG 6 • Valuable tools for intramedullary nailing of pediatric forearm fractures.
TECHNIQUES
Distal Radial Entry Point (Physeal Sparing)
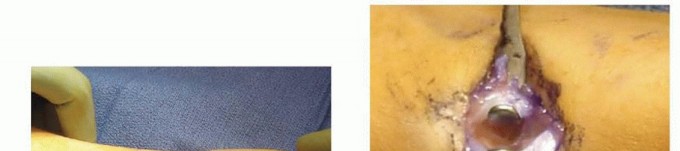
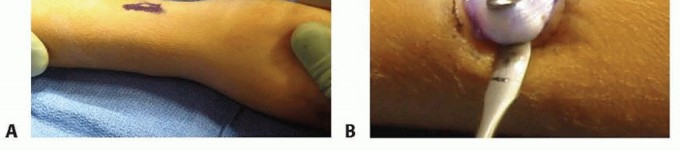
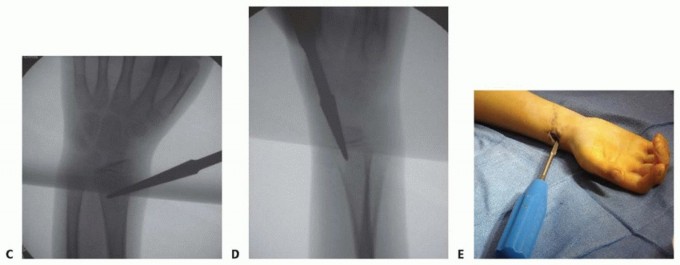
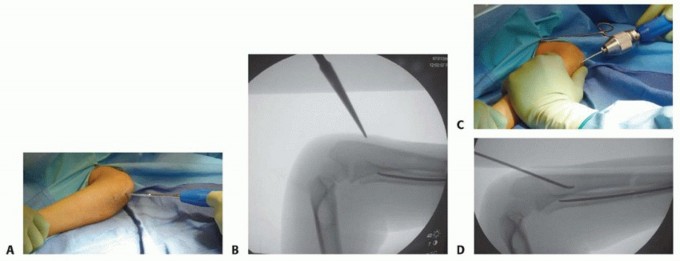
TECH FIG 1 •(continued)C,D. AP and lateral fluoroscopic confirmation of entry point. E. Well-seated and slightly angulated awl. After fluoroscopic confirmation of starting awl position, partial right and left rotations (not full turns) are used to gain satisfactory distal radial entry. A two-handed awl technique is used.Satisfactory intramedullary awl position is confirmed by a gentle “bounce” against the far cortex as well as fluoroscopic AP and lateral projections ( TECH FIG 1C-E).The awl is temporarily left in its intraosseous position before insertion of the radial flexible intramedullary nail. Thus, the surgeon's ability to judge both the portal location and the angle of nail entry will be facilitated by immediate sequential awl removal and nail tip insertion. Reduction and Nail Passage within the Radius


TECH FIG 2 • Insertion and passing of the radial nail. A. Gentle contouring of the distal aspect of the radial nail is important, as overbending effectively increases the diameter of the implant and may lead to nail incarceration. B. The “channel bender” is an effective tool for creating a properly contoured radial nail. C. The apex of the contoured nail should be placed so as to recreate appropriate radial bow (slightly distal of midshaft radius).(continued)

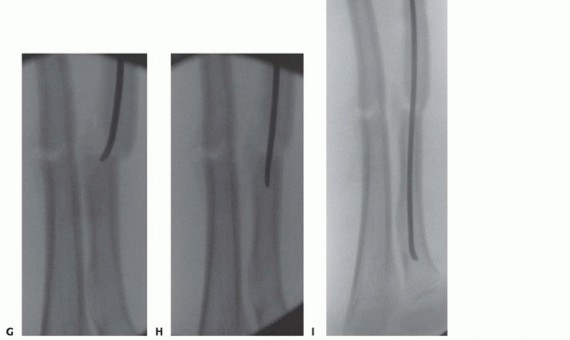
TECH FIG 2 •(continued)D. Under direct visualization, the contoured radial nail is manually inserted into the previously prepared entry point. Distinctive intramedullary tactile feedback (scrape) should be detected, and the implant advanced as far as possible using only the surgeon's hands. Note the trajectory of the nail (tip points radially), as this nail orientation should be maintained during most of the procedure. E. Appropriate longitudinal traction needs to be applied by an assistant as well as supplemental reduction forces such as that provided by the broad flat surface of a vinyl Meyerding mallet. F. The bent tip of the nail (the “fang”) approaches the fracture site after being advanced as far as possible without using a hammer. “Manual forces only” should be used as much as possible to advance the nail within the canal using a properly tightened T handle or similar chuck. G. As the fang crosses the fracture site, proximal fragment
TECH FIG 3 • Insertion and passing of the ulnar nail. A. As opposed to the radial entry point where a true incision is very important to allow protection of nerves and tendons, true percutaneous entry is an option for the anconeus starting point (distal to olecranon physis and just lateral off the ridge of the ulna). B. Radiographic confirmation of an acceptable awl entry point as well as awl trajectory is necessary. Anconeus entry is preferred over true tip-of-the-olecranon entry for two reasons: the anconeus entry point avoids unnecessary physeal injury and also decreases the likelihood of large painful olecranon bursae. C. The ulnar nail is contoured in a far more gentle fashion, as the ulna is a predominantly straight bone compared to the radius. After manual nail entry, the ulnar nail is advanced with the use of a chuck. Note the 90-degree flexed position of the elbow and the 90-degree external rotation of the shoulder. D. Similar nail advancement technique is used for the ulna, with the exception of any dramatic nail rotation maneuver at the end of nail insertion.Proper position within the proximal ulna is confirmed fluoroscopically ( TECH FIG 3D). Reduction and Nail Passage within the Ulna


TECH FIG 4 • My preferred closure, dressing, and splinting technique. A. Several interrupted absorbable sutures (typically 3-0 Vicryl) are used for closure of the subcutaneous and subcuticular portion of the radial wound. Steri-Strips are added for final wound closure (B), followed by Xeroform and sterile gauze (C), and a Tegaderm dressing (D). E. A similar dressing consisting of Xeroform, sterile gauze, and Tegaderm is applied to the proximal ulnar wound. F. A removable Velcro forearm fracture brace is applied at the end ofthe procedure.
PEARLS AND PITFALLS
Which bone to reduce and fix first?1.Once one bone is successfully reduced and stabilized via indirect techniques, achieving the same for the second bone will be more difficult. Thus, the radius should be stabilized first, as it is “deeper.” Then, if required, exposure of the nearly subcutaneous ulna is relatively easy.How much flexible nail should be left extruding from the bone?2.If it is too long, soft tissue adjacent to sharp nail edges is at risk. If it is too short, nail removal will be needlessly difficult.At what point should efforts at closed reduction be abandoned in favor of a limited open reduction?1.The author use the “three strikes and you're out” rule (three low-amplitude shots at crossing the fracture site) or the “11-minute rule.” Once either or both are violated, the author convert the case to an open reduction. Remember, cases of forearm compartment syndrome have been attributed to extended efforts at indirect reduction.What if an intramedullary nail seems to become incarcerated after crossing the fracture site?2.The surgeon should remove the nail and convert to one of a smaller diameter before creating new comminution or distracting the fracture site. Distracted fracture fragments may lead to nonunion.What if sterile intraoperative radiographs suggest malrotation of one or both of the forearm bones?1.The surgeon should back the offending nail up a bit and see if improved rotational alignment of the fracture fragments can be obtained via forearm rotation and T-handle chuck manipulation. The surgeon then readvances the nail to hold position. If this does not work, the surgeon should consider switching to a smaller diameter nail, as intramedullary interference fit may be excessive.When should the flexible nails be removed?3.The originators of this technique suggest nail removal by about the sixth postoperative month. Forearm shaft fractures have the highest refracture rate (about 12%) of all pediatric fractures.
POSTOPERATIVE CARE


OUTCOMES

COMPLICATIONS
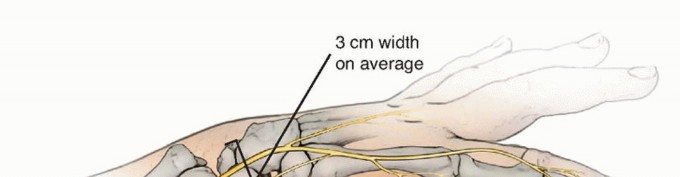
Sensory neurapraxia (usually the superficial branch of the radial nerve) occurs at a rate of at least 2% after flexible intramedullary nailing. These deficits are almost always temporary, resolving over weeks to months. The branching pattern of this nerve is such that it presents itself throughout the region of thefirst, second, and third extensor compartments ( FIG 8).2 FIG 8 • Relevant anatomy of superficial branch of the radial nerve in the region of the first, second, and third extensor compartments. The deep infection rate (osteomyelitis) after flexible intramedullary nailing of pediatric forearm shaft fractures is less than 0.5%; this can be compared to the reported 5% rate of osteomyelitis after plate fixation of similar fractures. 13Extensor tendon injury (especially the extensor pollicis longus) has been reported by multiple authors and may occur during nail insertion or nail removal as well as when tendons repetitively glide past a sharp nail tip (slowly sawing the tendon in two). Radial entry through the floor of the first compartment mayminimize this complication (vs. entry between the second and third compartments). 9,16In the clinical setting of forearm shaft fractures coexisting with ipsilateral humeral fracture (floating elbow), the incidence of compartment syndrome may be as high as 33%. When longer operative times arerequired (about 2 hours), a 7.5% rate of compartment syndrome has also been reported. 18P.113Delayed union and nonunion are decidedly rare after flexible intramedullary nailing of pediatric forearmfractures. If either delayed union or nonunion occurs, there is usually some explanation, such as atechnical error (eg, too large an intramedullary implant distracting the ulnar fracture site), infection, or neurofibromatosis.There should be a 5% or less chance of long-term forearm stiffness (defined as exceeding a 20 degree loss of pronation or supination) after flexible intramedullary forearm shaft fixation. 1
REFERENCES
- Antabak A, Luetic T, Ivo S, et al. Treatment outcomes of both-bone diaphyseal paediatric forearm fractures. Injury 2013;44(suppl 3):S11-S15.
- Auerbach DM, Collins ED, Kunkle KL, et al. The radial sensory nerve. An anatomic study. Clin Orthop Rel Res 1994;(308):241-249.
- Blackman AJ, Wall LB, Keeler KA, et al. Acute compartment syndrome after intramedullary nailing of isolated radius and ulna fractures in children. J Pediatr Orthop 2014;34(1):50-54.
- Bowman EN, Mehlman CT, Lindsell CJ, et al. Nonoperative treatment of both-bone forearm shaft fractures in children: predictors of early radiographic failure. J Pediatr Orthop 2011;31:23-32.
- Cheng JC, Ng BK, Ying SY, et al. A 10-year study of the changes in the pattern and treatment of 6,493 fractures. J Pediatr Orthop 1999;19:344-350.
- Colaris J, Reijman M, Allerma JH, et al. Single-bone intramedullary fixation of unstable both-bone diaphyseal forearm fractures in children leads to increased re-displacement: a multicenter randomized controlled trial. Arch Orthop Trauma Surg 2013;133:1079-1087.
- Davis DR, Green DP. Forearm fractures in children: pitfalls and complications. Clin Orthop Relat Res 1976;(120):172-183.
- Johari AN, Sinha M. Remodeling of forearm fractures in children. J Pediatr Orthop B 1999;8:84-87.
- Kravel T, Sher-Lurie N, Ganel A. Extensor pollicis longus rupture after fixation of radius and ulna fracture with titanium elastic nail (TEN) in a child: a case report. J Trauma 2007;63:1169-1170.
- Lascombes P, Prevot J, Ligier JN, et al. Elastic stable intramedullary nailing in forearm shaft fractures in children: 85 cases. J Pediatr Orthop 1990;10:167-171.
- Mehlman CT. Fractures of the forearm, wrist, and hand. Orthopaedic Knowledge Update 9. Rosemont, IL: AAOS, 2008.
- Mehlman CT, Araghi A, Roy DR. Hyphenated history: the Hueter-Volkmann law. Am J Orthop 1997;26:798-800.
- Mehlman CT, Wall EJ. Injuries to the shafts of the radius and ulna. In: Beaty JH, Kasser JR, eds. Rockwood and Wilkins' Fractures in Children, ed 6. Philadelphia: Lippincott Williams & Wilkins, 2006:399-441.
- Price CT, Scott DS, Kurzner ME, et al. Malunited forearm fractures in children. J Pediatr Orthop 1990;10:705-712.
- Schock CC. The crooked straight: distal radial remodeling. J Ark Med Soc 1987;84:97-100.
- Sproule JA, Roche SJ, Murthy EG. Attritional rupture of extensor pollicis longus tendon: a rare complication following elastic stable intramedullary nailing of a paediatric radial fracture. Hand Surg 2011;16:69-72.
- Younger AS, Tredwell SJ, Mackenzie WG, et al. Accurate prediction of outcome after pediatric forearm fracture. J Pediatr Orthop 1994;14:200-206.
- Yuan PS, Pring ME, Gaynor TP, et al. Compartment syndrome following fixation of pediatric forearm fractures. J Pediatr Orthop 2004;24:370-375.
