Comprehensive Introduction and Patho-Epidemiology
Intraarticular fractures of the phalanges and metacarpals present a profoundly complex biomechanical challenge to the orthopedic hand surgeon. The preservation of absolute articular congruity, joint stability, and a frictionless gliding surface is paramount to maintaining the intricate kinematics of the human hand. Fractures that disrupt the articular surface inevitably alter the distribution of forces across the joint, predisposing the patient to rapid-onset post-traumatic osteoarthritis, intractable stiffness, and profound functional impairment if managed inadequately. Unlike extraarticular diaphyseal fractures, which can often tolerate minor degrees of angulation or shortening, the articular surfaces of the hand demand meticulous anatomical restoration to preserve the highly specialized prehensile functions of grasp, pinch, and fine manipulation.
Epidemiologically, these injuries exhibit a bimodal distribution. High-energy axial loads, crush injuries, and shearing forces typically affect young, active males, often resulting from athletic trauma, industrial accidents, or interpersonal violence. Conversely, low-energy falls represent the primary mechanism in the elderly, osteopenic population. The metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints are most frequently implicated, with condylar fractures of the proximal and middle phalanges representing a particularly unstable and challenging subset of these injuries. The inherent lack of robust soft tissue envelopes surrounding these joints further complicates management, as periarticular scarring rapidly tethers the extensor mechanism and collateral ligaments.
The pathoanatomy of intraarticular disruption is dictated by the precise location of the fracture line and the deforming forces exerted by the intrinsic and extrinsic musculature. When an intraarticular fracture yields a single fragment that involves one-third or more of the joint surface, the structural integrity of the joint is fundamentally compromised. Such fractures are frequently accompanied by subluxation or frank dislocation due to the unopposed pull of the flexor or extensor tendons, combined with the destabilization of the collateral ligament complex. The ensuing incongruity creates a focal stress riser on the remaining intact cartilage, accelerating mechanical wear.
Furthermore, the spectrum of malunion in neglected or poorly managed intraarticular fractures presents a formidable salvage scenario. Rotational malalignment and angular deformities cause notable aesthetic and functional hand deformity, most dramatically accentuated when the patient attempts to make a composite fist, leading to digital overlapping or "scissoring." Patients frequently report a disturbance in their kinesthetic sense—a profound loss of fine proprioceptive control during complex hand tasks. The surgical philosophy regarding these injuries must balance the absolute necessity of anatomical reduction against the iatrogenic trauma of surgical exposure, which can itself precipitate the very stiffness the surgeon seeks to prevent.
Detailed Surgical Anatomy and Biomechanics
A rigorous understanding of the surgical anatomy and biomechanics of the hand is the foundation upon which all successful intraarticular fracture management is built. The stability of the metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints relies on a delicate, highly synchronized balance between the bony architecture, the volar plate, and the collateral ligaments. The metacarpal and phalangeal heads are not simple spheres; they are asymmetric condyles that exhibit a "cam effect." As the joint flexes, the collateral ligaments, which are eccentrically attached dorsal to the axis of rotation, become maximally taut. This anatomical nuance dictates that the joints must be immobilized in flexion to prevent collateral ligament contracture, a principle that governs all postoperative rehabilitation.
In condylar fractures, the fracture line typically propagates sagittally or coronally through the articular surface, effectively detaching the origin or insertion of the collateral ligament. Because the collateral ligament originates on the condyle, the displaced articular fragment is subjected to immense rotational and translational forces. The intact collateral ligament exerts a continuous tethering effect, often rotating the fragment out of the articular plane and drawing it proximally. However, this precise anatomical relationship can be leveraged surgically: the intact collateral ligament attached to the fractured condyle can be utilized as a tension band to assist in closed or percutaneous reduction via ligamentotaxis, guiding the fragment back into its anatomical bed when longitudinal traction and angular forces are applied.
The biomechanics of metacarpal neck fractures and their subsequent malunions highlight the critical importance of compensatory mobility within the carpometacarpal (CMC) joints. The tolerance for angular deformity varies drastically depending on the specific ray involved. The fifth CMC joint possesses approximately 20 to 30 degrees of anteroposterior mobility, and the fourth possesses 10 to 15 degrees. Consequently, flexion deformities of 40 degrees (and sometimes up to 50 degrees) in the fifth metacarpal neck can easily be accepted with excellent functional outcomes. When the fifth metacarpal head is displaced volarward due to a malunited fracture, the mobile CMC joint allows dorsal displacement of the distal end of the bone. When a hard object is grasped, the palm yields, preventing the metacarpal head from acting as a painful pressure point.
Conversely, the biomechanics of the index and long fingers are entirely different. There is little to no motion in the second and third CMC joints; they form the rigid central pillar of the hand. Because these joints cannot yield dorsally, any significant volar displacement of the metacarpal head results in a prominent, unyielding bony mass in the palm. Patients with malunions of the second or third metacarpal neck frequently experience severe pain with firm grasp and a profound mechanical block to flexion. Therefore, the threshold for surgical correction in the second and third metacarpals is exceptionally low, with angular deformities greater than 15 degrees often requiring corrective osteotomy. Furthermore, profound volar displacement alters the MCP joint biomechanics, forcing the proximal phalanx into compensatory hyperextension to achieve digital extension, which over time leads to secondary contracture of the collateral ligaments in a shortened position.
Exhaustive Indications and Contraindications
The decision-making algorithm for operative intervention in intraarticular hand fractures requires a synthesis of radiographic parameters, patient demands, and functional expectations. Non-operative management of displaced intraarticular fractures involving greater than 30% of the articular surface with associated subluxation universally leads to poor functional outcomes, rendering anatomical reduction and stable fixation absolute indications. Any articular step-off exceeding 1.0 millimeter is generally considered intolerable, as it exponentially increases contact stresses across the joint surface, precipitating early and aggressive post-traumatic osteoarthritis.
When evaluating malunited fractures, the philosophy of intervention must be strictly guided by functional deficit rather than radiographic appearance. Not every malunited fracture requires surgical intervention. Ill-advised surgical treatment of asymptomatic malunions usually fails to improve function and, due to the risks of scarring and stiffness, frequently exacerbates the patient's condition. Absolute indications for malunion correction include debilitating weakness of grasp, painful palmar prominences (particularly in the rigid 2nd and 3rd rays), and profound rotational deformities causing digital scissoring that mechanically impedes the function of adjacent normal digits.
Contraindications to surgical intervention, whether acute or reconstructive, must be carefully respected. Severe soft tissue compromise, such as extensive crush injuries with impending compartment syndrome or compromised vascularity, precludes immediate internal fixation. Active surgical site infection or profound systemic illness are absolute contraindications. Furthermore, relative contraindications include severe pre-existing osteoarthritis of the involved joint, where an osteotomy or ORIF would merely restore alignment to a fundamentally destroyed joint; in such cases, salvage procedures like arthrodesis or arthroplasty are more appropriate. Patient non-compliance, particularly an inability to adhere to rigorous postoperative rehabilitation, heavily favors non-operative or definitive salvage management.
Indications and Contraindications Summary
| Category | Absolute Indications | Relative Indications | Contraindications |
|---|---|---|---|
| Acute Intraarticular Fractures | Articular step-off > 1.0 mm; >30% joint surface involvement; Joint subluxation/dislocation; Rotational deformity. | Open fractures (requires immediate washout/fixation); Multiple adjacent fractures; Polytrauma patient requiring early hand mobilization. | Active local infection; Severe soft tissue crush precluding coverage; Medically unstable patient. |
| Malunited Fractures | Digital scissoring preventing composite fist; Painful palmar prominence in 2nd/3rd rays; Intolerable loss of grip strength. | Unacceptable aesthetic deformity (patient-dependent); Mild kinesthetic sense loss in high-demand professionals (e.g., musicians, surgeons). | Asymptomatic radiographic malunion; Severe pre-existing osteoarthritis; Stiff, painless joint in an elderly/low-demand patient. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the sine qua non of successful intraarticular fracture management. Standard radiographic evaluation must include true anteroposterior (AP), true lateral, and oblique views of the specific affected digit, rather than the entire hand, to prevent superimposition of adjacent bony structures. For intraarticular fractures of the metacarpal head, a Brewerton view (MCP joints flexed to 65 degrees, with the radiographic beam angled 15 degrees ulnar to radial) is invaluable for visualizing collateral ligament avulsion fractures and occult condylar splitting. In cases of severe comminution or complex fracture-dislocations, a fine-cut computed tomography (CT) scan with 3D reconstructions is highly recommended to map the precise location, size, and orientation of the articular fragments, guiding the surgical approach and implant selection.
Templating is particularly critical when planning corrective osteotomies for malunions. Contralateral, uninjured digit radiographs should be obtained to serve as an anatomical template. The surgeon must meticulously calculate the angle of deformity and plan the precise dimensions of the closing or opening wedge osteotomy. Implant selection must be predetermined; while smooth Kirschner wires (K-wires) remain the workhorse for acute condylar fractures, corrective osteotomies often demand the rigid stability provided by low-profile titanium mini-plates (1.3 mm to 2.0 mm systems) or headless compression screws to facilitate immediate postoperative mobilization and overcome the deforming forces of the contracted soft tissues.
Anesthetic considerations profoundly influence the intraoperative workflow. While regional blocks (axillary or supraclavicular) or local wrist blocks are standard, the advent of Wide-Awake Local Anesthesia No Tourniquet (WALANT) has revolutionized hand surgery. Utilizing a mixture of lidocaine and epinephrine allows for a bloodless field without the need for a pneumatic tourniquet. More importantly, WALANT permits the surgeon to intraoperatively assess the tenodesis effect and ask the patient to actively flex and extend the digit. This real-time, active functional assessment is invaluable for confirming the absolute stability of the fixation and ensuring that no rotational malalignment or scissoring persists under physiological load.
If traditional anesthesia is utilized, the patient is positioned supine with the operative arm extended on a radiolucent hand table. A well-padded pneumatic upper arm tourniquet is applied and inflated to 250 mm Hg following exsanguination with an Esmarch bandage. The positioning of the fluoroscopy unit is critical; a mini-C-arm must be brought in parallel to the hand table, allowing the surgeon to obtain seamless AP, lateral, and oblique intraoperative imaging by rotating the C-arm rather than manipulating the fragile, provisionally reduced fracture.
Step-by-Step Surgical Approach and Fixation Technique
Condylar fractures are notoriously unstable, and their surgical management demands exacting precision. The initial step involves a thorough fluoroscopic assessment of displacement. Displaced, unstable condylar fractures almost universally require open reduction and internal fixation (ORIF) or precise percutaneous pinning if closed reduction is successful.
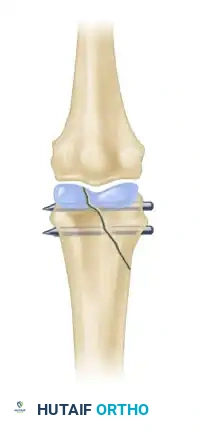
Figure 1: Displaced, unstable condylar fracture. The articular step-off and rotational deformity necessitate intervention to restore joint congruity.
Before committing to a formal open approach, closed manipulation via ligamentotaxis should be meticulously attempted. By applying longitudinal traction and utilizing the intact collateral ligament, the surgeon can often guide the displaced condylar fragment back into its anatomical bed. The finger is typically flexed to tighten the collateral ligaments, which pulls the fragment into alignment with the intact condyle.

Figure 2: Manipulation of the fracture using the intact collateral ligament. This tension permits the precise insertion of a Kirschner wire to provisionally hold the reduction.
Once anatomical reduction is confirmed fluoroscopically, percutaneous pinning is performed. A 0.035-inch or 0.045-inch K-wire is driven transversely across the condyles. A single K-wire acts merely as an axis of rotation; even if the fracture appears perfectly reduced on AP and lateral views, a single wire cannot control the rotational forces exerted by the collateral ligament during postoperative mobilization. Therefore, to prevent the reduced fragment from spinning around the primary wire, a second K-wire must be inserted. This second wire can be placed parallel to the first or in a divergent configuration, depending on the size of the fragment.

Figure 3: Two wires are strictly necessary to avoid rotation of the reduced fragment and ensure absolute stability of the articular surface.
If closed reduction is inadequate (articular step-off >1 mm), an open approach is mandated. A mid-axial or dorsal approach is utilized, carefully splitting or retracting the extensor apparatus to preserve its gliding paratenon. The joint capsule is incised longitudinally to visualize the articular surface directly. Hematoma, bone debris, and soft tissue interposition (often the collateral ligament or volar plate) are meticulously cleared from the fracture site. The fragment is reduced under direct vision using a pointed reduction forceps, taking extreme care not to crush the fragile articular cartilage. Fixation is achieved with two transverse K-wires or, if the fragment is large enough to accommodate the core diameter without splitting, miniature interfragmentary screws (1.0 mm or 1.2 mm).
Intraoperative imaging must confirm absolute articular congruity and appropriate implant length, ensuring screws or wires do not protrude into the contralateral joint space or tether the collateral ligaments.

Figure 4: Anteroposterior radiograph demonstrating a condylar fracture anatomically reduced and fixed with two crossed Kirschner wires.

Figure 5: Lateral radiograph of the same condylar fracture, confirming restoration of the articular contour and appropriate wire placement.
For the surgical correction of malunions, a dorsal longitudinal incision is made over the affected metacarpal or phalanx. A closing wedge or opening wedge osteotomy is performed at the apex of the deformity, which is usually the old fracture site. Rigid internal fixation is mandatory to allow early mobilization, typically achieved with a low-profile titanium mini-plate. Importantly, if the malunion is chronic and the metacarpal head was markedly displaced volarward, the MCP joint will have hyperextended, leading to secondary contracture of the collateral ligaments. In these complex cases, simply performing a corrective osteotomy will not restore motion; a concomitant dorsal capsulotomy and collateral ligament release must be performed.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, intraarticular hand fractures and malunion corrections are fraught with potential complications. The most ubiquitous complication is postoperative stiffness, primarily resulting from capsular contracture, extensor tendon adhesions, and prolonged immobilization. The highly reactive nature of the periarticular soft tissues in the hand means that even minor hematomas can organize into dense, restrictive scar tissue. Prevention through rigid internal fixation that permits immediate, controlled active motion is the most effective strategy against stiffness.
Post-traumatic osteoarthritis (PTOA) and avascular necrosis (AVN) represent severe, late-stage complications. PTOA is the direct consequence of residual articular step-off, which alters joint kinematics and accelerates cartilage wear. AVN, particularly of the condylar fragments or the metacarpal head, can occur if the delicate vascular supply is stripped during an overly aggressive open reduction. Hardware failure, including pin migration, breakage, or loss of reduction, occurs in approximately 5-10% of cases, often necessitating revision surgery. Pin tract infections are common with percutaneous K-wires but generally resolve with local care and oral antibiotics; however, deep intraarticular sepsis is a catastrophic complication requiring immediate hardware removal, joint washout, and intravenous antibiotics.
When acute fixation fails, or severe intraarticular malunion leads to impending joint destruction accompanied by intractable pain, salvage procedures are indicated. Simple osteotomy is insufficient in the face of widespread cartilage loss. In these scenarios, osteoarticular grafts, such as transferring a portion of the toe proximal phalanx or performing a hemi-hamate arthroplasty for PIP joint reconstruction, can restore a functional, pain-free arc of motion. Alternatively, in high-demand patients requiring absolute stability, arthrodesis is the gold standard. The MCP joint is typically fused at 25-30 degrees of flexion, while the PIP joint is fused at varying degrees of flexion depending on the digit (e.g., 40 degrees for the index, progressing to 55 degrees for the small finger) to optimize the cascade of the hand. For low-demand, elderly patients, silicone interpositional arthroplasty remains a viable option to maintain motion and relieve pain.
Complications and Salvage Management Summary
| Complication | Estimated Incidence | Pathophysiology | Salvage / Management Strategy |
|---|---|---|---|
| Joint Stiffness / Adhesions | 30 - 50% | Capsular contracture, paratenon scarring, prolonged immobilization. | Intensive hand therapy, dynamic splinting; late surgical tenolysis/capsulotomy (after 6 months). |
| Post-Traumatic Osteoarthritis | 15 - 25% | Residual articular step-off >1mm, cartilage necrosis, altered joint kinematics. | NSAIDs, intraarticular injections; Arthrodesis or Silicone Arthroplasty for end-stage destruction. |
| Pin Tract Infection | 10 - 15% | Bacterial colonization of percutaneous K-wires (typically Staph aureus). | Oral antibiotics, daily chlorhexidine pin care; immediate removal if deep joint space is threatened. |
| Avascular Necrosis (AVN) | < 5% | Disruption of intraosseous or capsular blood supply during ORIF. | Osteoarticular grafting (hemi-hamate or toe phalanx transfer); definitive arthrodesis. |
Phased Post-Operative Rehabilitation Protocols
The ultimate functional outcome of both acute intraarticular fracture fixation and malunion correction relies as heavily on meticulous postoperative rehabilitation as it does on the surgical execution. The rehabilitation protocol must be carefully phased, balancing the biomechanical stability of the fixation against the physiological necessity of early motion to prevent restrictive adhesions.
Phase I: Immediate Postoperative Period (Days 0-14)
Immediately postoperatively, the hand is placed in a bulky soft compressive dressing and a custom-molded volar orthosis. The hand must be strictly positioned in the "intrinsic plus" (or safe) position: the wrist extended 20 to 30 degrees, the MCP joints flexed 70 to 90 degrees, and the PIP and DIP joints fully extended. This precise positioning is non-negotiable; it maintains the collateral ligaments of the MCP joints at their maximal length, preventing the devastating complication of extension contracture. Strict elevation and active digital motion of the uninvolved fingers are initiated immediately to control edema.
Phase II: Early Motion and Splint Weaning (Weeks 2-6)
If rigid internal fixation was achieved (e.g., interfragmentary screws or mini-plates), gentle, supervised active range of motion (AROM) of the affected digit may begin within 3 to 5 days. The patient is transitioned to a removable thermoplastic splint, worn between exercise sessions. If percutaneous K-wires were utilized, the joint is typically protected for a longer duration, and motion may be restricted to adjacent joints until early callus formation is evident. Pin site care is instituted using chlorhexidine or half-strength hydrogen peroxide to prevent superficial colonization.
Phase III: Hardware Removal and Progressive Motion (Weeks 6-12)
K-wires are typically removed in the clinic at 4 to 6 weeks once radiographic evidence of bridging callus is observed and clinical stability is confirmed. Following hardware removal, the rehabilitation protocol aggressively escalates. Passive range of motion (PROM) exercises are initiated to overcome residual capsular tightness. Dynamic or static progressive splinting may be introduced if specific joint contractures persist (e.g., a dynamic extension splint for PIP flexion contractures). Progressive strengthening, utilizing therapy putty and grip strengthening devices, is delayed until absolute clinical and radiographic union is confirmed, usually around 6 to 8 weeks postoperatively.
Phase IV: Return to Function and Late Interventions (3+ Months)
Patients are gradually cleared for a full return to occupational and athletic activities. The surgeon and therapist must monitor for plateauing of functional gains. If a patient exhibits a rigid, unyielding contracture despite 4 to 6 months of compliant, aggressive hand therapy, surgical intervention such as tenolysis, dorsal capsulotomy, or collateral ligament release may be considered, provided the underlying bony architecture has solidly united and remodeled.
Summary of Landmark Literature and Clinical Guidelines
The contemporary management of intraarticular hand fractures is heavily informed by decades of evolving biomechanical research and clinical outcomes studies. The foundational principles of articular fracture management in the hand were largely codified by the early works of Hastings and Carroll, who established the critical distinction between stable, reducible fractures and those requiring absolute rigid internal fixation to prevent rapid articular degradation. Their classification systems continue to guide the initial assessment of condylar and base of phalanx fractures.
Regarding the management of malunions, the landmark biomechanical and clinical studies by Ali et al. and Ford et al. fundamentally shifted the paradigm of metacarpal neck fracture treatment. Their research definitively established the compensatory mobility of the carpometacarpal joints, proving that the 5th CMC joint's 20 to 30 degrees of mobility allows for the functional acceptance of up to 40 to 50 degrees of flexion deformity in the fifth metacarpal neck. This literature serves as the primary defense against the over-treatment of boxer's fractures and their subsequent malunions, emphasizing that radiographic perfection is secondary to clinical function.
Biomechanical comparisons of fixation modalities have also shaped current guidelines. Studies evaluating crossed K-wires versus interfragmentary miniature screws demonstrate that while screws provide superior compressive forces and torsional stability for large, single fragments, they carry a higher risk of iatrogenic comminution in smaller fragments. Consequently, the American Academy of Orthopaedic Surgeons (AAOS) and the American Society for Surgery of the Hand (ASSH) guidelines maintain that percutaneous or open K-wire fixation remains the highly effective, gold-standard technique for comminuted or small-fragment condylar fractures, provided that at least two non-collinear wires are utilized to control rotation.
Current clinical consensus strictly mandates that any articular step-off exceeding 1.0 mm in a weight-bearing or primary gliding zone of the hand requires surgical reduction. The literature universally supports the axiom that in the realm of intraarticular hand trauma, the surgeon must weigh the functional deficits against the inherent risks of surgical exposure, always prioritizing the restoration of a stable, congruent, and mobile joint over the mere pursuit of a radiographically straight bone.
