INTRODUCTION TO INTERTROCHANTERIC FEMORAL FRACTURES
Intertrochanteric femoral fractures represent one of the most frequently encountered injuries in orthopedic traumatology, predominantly affecting the geriatric population following low-energy falls. In younger cohorts, these fractures are typically the result of high-energy trauma. Because the intertrochanteric region is entirely extracapsular and composed of highly vascularized cancellous bone, these fractures boast a robust healing potential. However, the complex biomechanical forces acting across the proximal femur make achieving and maintaining stable surgical fixation a profound clinical challenge.
The primary goal of operative intervention is to achieve stable fixation that permits immediate postoperative mobilization, thereby mitigating the devastating systemic complications associated with prolonged recumbency, such as deep vein thrombosis (DVT), pulmonary embolism, pneumonia, and decubitus ulcers.
CLASSIFICATION SYSTEMS
Accurate classification is paramount for preoperative planning, implant selection, and predicting the biomechanical stability of the fracture pattern. Over the decades, numerous classification systems for peritrochanteric and intertrochanteric femoral fractures have been proposed.
The Boyd and Griffin Classification
Historically significant, Boyd and Griffin initially described four distinct types of peritrochanteric femoral fractures in 1949. While largely superseded by modern systems, understanding this classification provides valuable insight into fracture morphology:
- Type 1: Fractures that extend linearly along the intertrochanteric line. These are generally stable and easily reduced.
- Type 2: Comminuted fractures with the main fracture line coursing along the intertrochanteric line, accompanied by multiple secondary fracture lines. This may include a coronal fracture line visible on the lateral radiograph, indicating posteromedial comminution.
- Type 3: Fractures that extend to, or are distal to, the lesser trochanter. These represent a transition toward subtrochanteric patterns and exhibit significant mechanical instability.
- Type 4: Complex fractures of the trochanteric region and proximal shaft involving fracture lines in at least two planes, often requiring advanced intramedullary fixation techniques.
The AO/OTA Classification
Today, the most universally accepted and clinically useful classification for intertrochanteric femoral fractures is the AO/OTA classification. This system is critical for evaluating treatment outcomes and standardizing academic literature. It divides these fractures (designated as segment 31) into three primary groups based on the status of the lateral femoral wall and the degree of comminution:
- 31A1 (Simple Pertrochanteric): Fractures are not comminuted. The lateral wall remains intact, and the fracture line extends from the greater to the lesser trochanter. These are highly stable once reduced.
- 31A2 (Multifragmentary Pertrochanteric): Fractures exhibit increasing comminution, specifically involving the posteromedial cortex (lesser trochanter). The lateral wall remains intact but may be tenuous.
- 31A3 (Intertrochanteric): Fractures include reverse obliquity patterns or subtrochanteric extensions. The lateral wall is incompetent. These are inherently unstable and biomechanically unsuitable for standard sliding hip screws.
Clinical Pearl: The integrity of the lateral femoral wall is the single most critical determinant in implant selection. A lateral wall thickness of less than 20.5 mm on the preoperative anteroposterior (AP) radiograph is highly predictive of postoperative lateral wall fracture and subsequent fixation failure if a dynamic hip screw is utilized.
CLINICAL EVALUATION AND IMAGING
Standard radiographic evaluation must include an AP view of the pelvis, an AP view of the affected hip, and a cross-table lateral view. In cases of severe comminution or when the extension of the fracture into the subtrochanteric region is unclear, a computed tomography (CT) scan with 3D reconstruction is highly recommended.
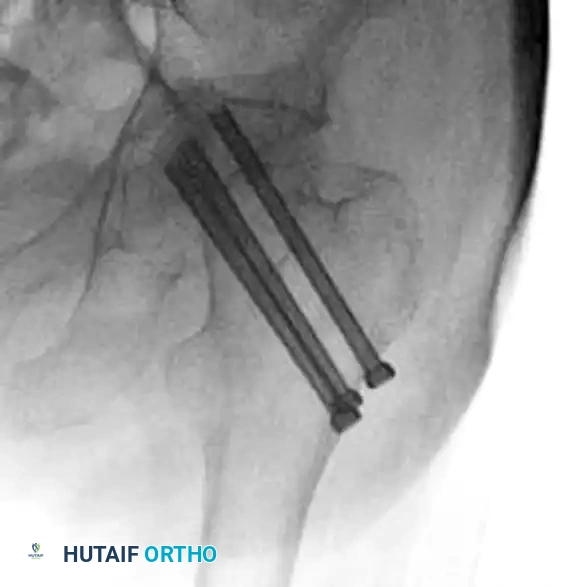
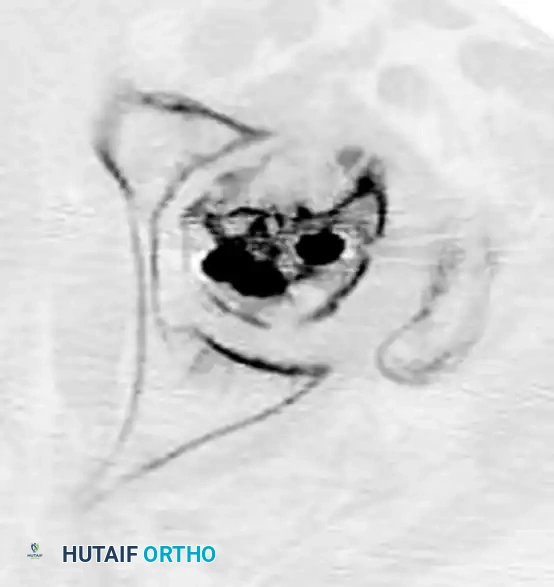
While osteonecrosis (avascular necrosis) is classically associated with intracapsular femoral neck fractures, proximal femoral trauma and its subsequent surgical management can occasionally compromise the vascular supply to the femoral head, particularly in combined fracture patterns or following aggressive surgical dissection.
FIGURE 55-19 Osteonecrosis after treatment of proximal femoral fracture. Anteroposterior radiograph (A), axial CT scan (B), and coronal CT scan (C) demonstrating advanced collapse and hardware penetration.

INDICATIONS FOR TREATMENT
Nonoperative Management
Nonoperative treatment of intertrochanteric femoral fractures is exceedingly rare in modern orthopedic practice. It is strictly reserved for nonambulatory, bedbound patients with severe medical comorbidities where the perioperative mortality risk unacceptably outweighs the benefits of surgery, provided that adequate pain control can be achieved through conservative measures.
Operative Management
Internal fixation is the definitive standard of care for the vast majority of intertrochanteric femoral fractures. Optimal fixation is predicated on the inherent stability of the fracture pattern. The mainstay of treatment involves either a screw-side plate device (Dynamic Hip Screw) or a cephalomedullary nail.
SURGICAL BIOMECHANICS AND IMPLANT SELECTION
Treatment with Screw-Side Plate Devices (Dynamic Hip Screws)
Compression or dynamic hip screws (DHS) remain an excellent, evidence-based option for the treatment of stable intertrochanteric femoral fractures (AO/OTA 31A1 and select 31A2 fractures with a robust lateral wall).
The biomechanical principle of the DHS relies on controlled collapse. The lag screw is allowed to slide within the barrel of the side plate, enabling the fracture fragments to impact and compress under physiological weight-bearing loads. This dynamic compression promotes primary bone healing and enhances construct stability.
Furthermore, the implant cost is significantly less with screw-side plate devices compared to intramedullary nails. The surgical technique for DHS placement is familiar to most experienced orthopedic surgeons; however, it is noted that recent graduates who have trained predominantly in the era of intramedullary nailing may require deliberate practice to master this classic procedure.
Surgical Warning: The use of a DHS in reverse obliquity fractures (31A3) or fractures with an incompetent lateral wall is strictly contraindicated. In these patterns, the femoral shaft will medialize, leading to catastrophic implant cut-out and fixation failure.
Treatment with Intramedullary Devices (Cephalomedullary Nails)
For unstable fracture patterns (AO/OTA 31A2 with lateral wall comminution and all 31A3 reverse obliquity fractures), cephalomedullary nailing is the implant of choice. Intramedullary devices offer a shorter lever arm, transferring weight-bearing forces more directly to the femoral shaft and bypassing the compromised lateral cortex.
PREOPERATIVE PLANNING AND PATIENT POSITIONING
Meticulous patient positioning is the foundation of a successful proximal femur fracture fixation.
- Anesthesia and Setup: The patient is placed supine on a radiolucent fracture table following the administration of spinal or general anesthesia.
- Traction and Reduction: The operative leg is placed in a traction boot. Gross traction is applied to restore leg length, followed by 10 to 15 degrees of internal rotation to correct the anteversion of the femoral neck and bring it parallel to the floor.
- Fluoroscopy: An image intensifier (C-arm) is positioned between the patient's legs (if the unaffected leg is placed in a hemilithotomy position) or angled obliquely if the legs are positioned in a "scissor" configuration. Perfect AP and lateral fluoroscopic views of the femoral head and neck must be obtained before prepping and draping.
SURGICAL APPROACH AND TECHNIQUE: DYNAMIC HIP SCREW
1. The Lateral Approach
A straight lateral incision is made starting at the tip of the greater trochanter and extending distally for approximately 8 to 10 cm. The fascia lata is incised in line with the skin incision. The vastus lateralis is elevated off the lateral intermuscular septum and retracted anteriorly, or split longitudinally, to expose the lateral femoral cortex.
2. Capsulotomy (When Indicated)
While routine capsulotomy is not required for standard extracapsular intertrochanteric fractures, it may be necessary for hematoma evacuation or if there is an associated intracapsular component.
Clinical Pearl: When performing a deep capsulotomy, the risk of the scalpel blade dissociating from the handle deep within the wound is a known hazard.
FIGURE 55-20 Strip of Ioban placed around the junction of the scalpel blade and handle to prevent dissociation of the blade from the handle during deep capsulotomy.

3. Guide Wire Placement
An angle guide (typically 135 degrees) is placed against the lateral cortex. A 2.8 mm guide wire is advanced through the lateral cortex, up the femoral neck, and into the center of the femoral head.
The position of the guide wire is the most critical step of the operation. It must be perfectly centered in the femoral head on both the AP and lateral fluoroscopic views. The Tip-Apex Distance (TAD), defined by Baumgaertner, must be strictly calculated. A TAD of less than 25 mm significantly reduces the risk of lag screw cut-out.
4. Reaming and Tapping
The guide wire is measured to determine the appropriate lag screw length. A triple reamer is assembled and advanced over the guide wire to ream the lateral cortex, the femoral neck, and to countersink the plate-barrel junction. If the patient has dense, young bone, tapping of the femoral head may be required; however, in osteoporotic bone, tapping is generally avoided to maximize screw purchase.
5. Lag Screw and Plate Insertion
The selected lag screw is inserted over the guide wire. The side plate is then slid over the back of the lag screw and impacted against the lateral femoral shaft. The plate is secured to the femoral shaft using 4.5 mm cortical screws. Traction is released, and the fracture is allowed to compress.
COMPLICATIONS AND SALVAGE PROCEDURES
Despite optimal surgical technique, complications can arise, particularly in severely osteoporotic bone or highly unstable fracture patterns.
Implant Cut-Out
Cut-out of the lag screw through the superior aspect of the femoral head is the most common mechanical failure, usually resulting from a TAD > 25 mm, varus malreduction, or unrecognized lateral wall incompetence.
Conversion to Total Hip Arthroplasty (THA)
In cases of catastrophic fixation failure, nonunion, severe post-traumatic osteonecrosis, or pre-existing symptomatic osteoarthritis, salvage via Total Hip Arthroplasty (THA) is indicated. Converting a failed intertrochanteric fracture to a THA is technically demanding due to distorted anatomy, retained hardware, and compromised bone stock.
FIGURE 55-21 Total hip arthroplasty for the treatment of proximal femoral fracture complications. A, Preoperative anteroposterior radiograph demonstrating hardware failure and joint destruction. B, One year after total hip arthroplasty utilizing a long-stem diaphyseal engaging implant.


When performing a salvage THA, the surgeon must be prepared to use diaphyseal-fitting long stems to bypass the stress risers created by the previous screw holes in the proximal femur. Calcar replacement stems may also be necessary if the medial cortex is severely deficient.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The postoperative management of intertrochanteric fractures is as critical as the surgical execution.
- Weight-Bearing: For stable fracture patterns fixed with a DHS or IM nail, patients are encouraged to bear weight as tolerated immediately postoperatively. Early mobilization is the primary defense against cardiopulmonary complications.
- VTE Prophylaxis: Chemical prophylaxis (e.g., Low Molecular Weight Heparin or Direct Oral Anticoagulants) combined with mechanical prophylaxis is mandatory for a minimum of 28 to 35 days postoperatively, barring contraindications.
- Osteoporosis Management: An intertrochanteric fracture is a fragility fracture. Postoperative protocols must include a formal osteoporosis workup, including DEXA scanning, Vitamin D and Calcium supplementation, and the initiation of bisphosphonates or anabolic agents to prevent secondary fractures.
By adhering to strict biomechanical principles, accurate classification, and precise surgical techniques, orthopedic surgeons can reliably restore function and minimize morbidity in patients suffering from intertrochanteric femoral fractures.
