Principles of Diagnostic and Therapeutic Injection Studies
Whenever a clinical diagnosis remains equivocal, or when a patient's pathological condition presents as diffuse and multi-segmental, the precise identification of the primary pain generator becomes a complex diagnostic challenge. In these scenarios, spinal injection studies utilizing local anesthetics, contrast media, and corticosteroids serve as indispensable tools in the armamentarium of the orthopedic spine surgeon.
These interventions are relatively simple, highly safe when performed under strict imaging protocols, and minimally painful. By systematically isolating specific anatomical structures—such as facet joints, exiting nerve roots, or the epidural space—surgeons can correlate ambiguous imaging abnormalities with the patient's subjective pain experience.
Clinical Pearl: Structural abnormalities visualized on MRI or CT do not universally correlate with symptomatic pain. Diagnostic injections bridge the gap between radiological findings and clinical symptomatology, preventing unwarranted surgical interventions on asymptomatic degenerative lesions.

Pharmacological Agents in Spinal Injections
The selection of pharmacological agents is critical to both the efficacy and safety of spinal injection studies. The injectate typically consists of a triad: contrast media, local anesthetics, and corticosteroids.
Contrast Media
The optimal contrast medium for documenting structures outside the subarachnoid space must be absorbable and possess low neuro-reactivity, mitigating the risk of chemical arachnoiditis in the event of inadvertent intrathecal administration.
* Preferred Agents: Iohexol (Omnipaque) and metrizamide (Amipaque) are the least reactive, most widely accepted, and best-tolerated nonionic contrast media currently available.
* Alternative Agents: Diatrizoate meglumine (Hypaque), iothalamate meglumine (Conray), and iopamidol have also been utilized safely for discography and epidural blocks.

Local Anesthetics
Local anesthetics such as lidocaine (Xylocaine), tetracaine (Pontocaine), and bupivacaine (Marcaine) are frequently employed for epidural and intradural anesthesia.
* Bupivacaine Warning: The use of bupivacaine must be strictly limited to low concentrations and low volumes. There are well-documented reports of severe cardiovascular collapse and death following epidural anesthesia utilizing bupivacaine concentrations of 0.75% or higher.
Corticosteroids
Steroids prepared for intramuscular injection are frequently repurposed for the epidural space. However, the choice of steroid is paramount to patient safety.
* Historical Pitfalls: In the past, spinal arachnoiditis was strongly associated with the epidural administration of methylprednisolone acetate (Depo-Medrol). This catastrophic complication was traced to the suspending agent, polyethylene glycol. Although this agent has since been eliminated from the preparation, caution remains.
* Preferred Agent: We strongly advocate for the use of Celestone Soluspan (a mixture of betamethasone sodium phosphate and betamethasone acetate). It provides both immediate and long-term duration of action, is highly soluble (non-particulate), and contains no harmful preservatives. If unavailable, triamcinolone (40 mg/mL) serves as an acceptable substitute.

Clinical Evaluation and Diagnostic Pain Diary
When discrete, well-controlled injection techniques are directed at specific targets in and around the spine, grading the degree of pain before and after the injection is the definitive method for localizing the pain generator.
The patient must be instructed to grade their pain on a standardized 0-to-10 scale prior to the procedure and at specific intervals post-injection.
The Pain Scale and Diary (Box 39-2)
- 0: No pain
- 1: Mild pain that you are aware of but not bothered by
- 2: Moderate pain that you can tolerate without medication
- 3: Moderate pain that is discomforting and requires medication
- 4-5: More severe pain; you begin to feel antisocial
- 6: Severe pain
- 7-9: Intensely severe pain
- 10: Most severe pain; contemplating suicide over it
Diagnostic Threshold: If a selective spinal injection performed under strict fluoroscopic control results in a 50% or greater decrease in the level of pain (corresponding to the pharmacological duration of the anesthetic agent used), the targeted anatomical area is presumed to be the primary pain generator.
Epidural Corticosteroid Injections: Efficacy and Safety
Epidural injections in the cervical, thoracic, and lumbosacral spine were developed to both diagnose and treat spinal pain. Because severe pain from an acute disc injury (with or without radiculopathy) is often time-limited, therapeutic injections manage acute pain phases, facilitating physical therapy and decreasing reliance on oral opioid analgesics.
Clinical Efficacy
The literature contains over 40 studies encompassing more than 4,000 patients evaluating the efficacy of lumbar and caudal epidural corticosteroid injections.
* Response Rates: Kepes and Duncalf calculated an average favorable response rate of 60% for lumbar epidural steroid injections, while White reported a favorable response rate of 75%.
* Prognostic Value: Patients with acute back and leg pain (< 3 months duration) respond significantly better to epidural corticosteroids. Furthermore, patients who achieve substantial (even if temporary) relief of leg pain from a well-placed transforaminal injection are highly likely to benefit from definitive surgical decompression. Conversely, patients who fail to respond and have endured radicular pain for >12 months are statistically unlikely to benefit from surgery.

Complications and Contraindications
While generally safe, serious complications have been reported, including epidural abscess, epidural hematoma, durocutaneous fistula, and iatrogenic Cushing syndrome.
* Vasovagal Syncope: The most common immediate adverse reaction during the procedure.
* Dural Puncture: Occurs in 0.5% to 5% of patients. Postdural puncture headaches (positional) occur in 7.5% to 75% of these cases, with the highest incidence associated with large-bore (16-gauge and 18-gauge) needles.
* Non-Dural Puncture Headaches: Occur in approximately 2% of patients, attributed to air injected into the epidural space or increased intrathecal pressure from fluid volume.
* Minor Reactions: Nonpositional headaches, facial flushing, insomnia, low-grade fever, and transient exacerbation of radicular pain.
Absolute Contraindications:
1. Localized infection at the injection site.
2. Systemic infection or sepsis.
3. Bleeding diathesis or therapeutic anticoagulation.
4. Uncontrolled diabetes mellitus.
5. Severe congestive heart failure.

The Imperative of Fluoroscopic Guidance
We mandate the use of fluoroscopy for all diagnostic and therapeutic epidural injections. Performing these procedures "blind" (relying solely on tactile feedback) is academically and clinically unacceptable in modern practice.
- High Miss Rates: Even in the hands of highly experienced clinicians, needle misplacement occurs in 40% of caudal and 30% of lumbar epidural injections when performed without fluoroscopic guidance.
- Intravascular Injection: Accidental intravascular injection is common. The absence of blood return upon needle aspiration is a notoriously unreliable indicator of intravascular placement. Only real-time fluoroscopic contrast flow can confirm extravascular placement.
- Anatomical Anomalies: Midline epidural septa or loculated epidural compartments can restrict the flow of injectate. Without an epidurogram, the surgeon remains blind to these flow restrictions, leading to false-negative diagnostic results.

Cervical Epidural Injections
Cervical epidural steroid injections are highly effective for treating cervical spondylosis associated with acute disc disruption, cervical radiculopathies, postlaminectomy pain syndromes, and acute viral brachial plexitis. The most robust clinical outcomes are observed in patients with acute soft disc herniations presenting with well-defined radicular symptoms.
Interlaminar Approach (Technique 39-2)
The interlaminar approach is the gold standard for cervical epidural access. It is routinely performed at the C7-T1 interspace, as the epidural space is widest at this level, minimizing the risk of dural puncture or spinal cord injury. If previous posterior surgery has altered this anatomy, the C6-7 or T1-2 levels are utilized.
Step-by-Step Surgical Technique:
1. Positioning: Place the patient prone on a radiolucent pain management table (low-attenuated carbon fiber tabletop) to permit unobstructed C-arm fluoroscopy. Secure the patient’s face in a cervical prone cutout cushion to maintain neutral cervical alignment.
2. Preparation: Aseptically prepare the skin with chlorhexidine gluconate (Hibiclens) or povidone-iodine, covering several segments above and below the target interspace. Drape in a standard sterile fashion.
3. Localization: Using anteroposterior (AP) fluoroscopic imaging, identify the target laminar interspace.
4. Local Anesthesia: Raise a skin wheal over the target interspace (paramedian, on the side of the patient’s pain) using a 27-gauge needle and 1-2 mL of 1% preservative-free lidocaine. (Pearl: Buffer the lidocaine with 3 mL of 8.4% sodium bicarbonate per 30 mL to eliminate burning).
5. Needle Insertion: Nick the skin with an 18-gauge hypodermic needle. Under continuous AP fluoroscopic control, advance a 22-gauge, 3 ½-inch spinal needle vertically until contact is made with the upper edge of the T1 lamina, 1 to 2 mm lateral to the midline. Anesthetize the periosteum and soft tissue tract upon withdrawal.

- Tuohy Needle Advancement: Insert an 18-gauge, 3 ½-inch Tuohy epidural needle through the anesthetized tract. Advance vertically until bony contact is made with the T1 lamina.
- Loss of Resistance: Carefully "walk off" the superior edge of the lamina with the Tuohy needle, directing it anteriorly into the ligamentum flavum. Remove the stylet. Attach a 10-mL glass syringe filled halfway with air and sterile saline. Advance the needle millimeter by millimeter using continuous pressure on the plunger. A sudden "loss of resistance" indicates breaching of the ligamentum flavum and entry into the epidural space.
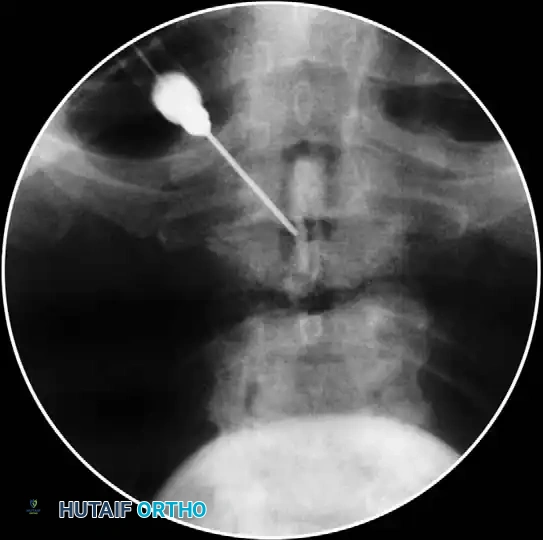
- Aspiration and Contrast: Aspirate to ensure no CSF or blood return. Attach a 5-mL syringe containing 1.5 mL of nonionic contrast dye (e.g., Iohexol).
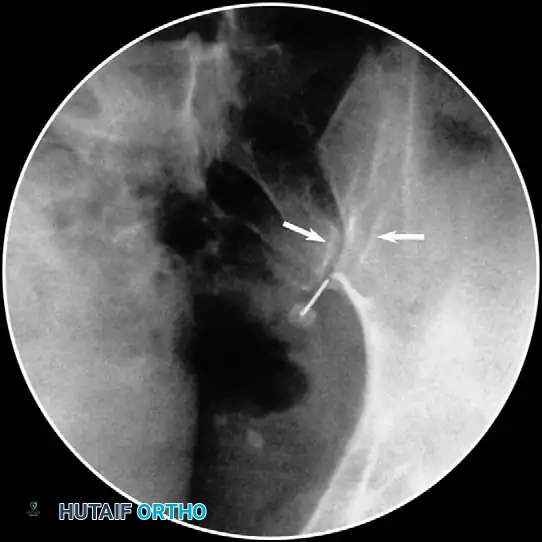
- Epidurogram Confirmation: Inject the contrast under live fluoroscopy to produce an epidurogram. Adjust the C-arm to a lateral perspective to definitively document posterior epidural spread and rule out intrathecal or intravascular flow.
- Test Dose and Injection: Inject a test dose of 1-2 mL of 1% preservative-free lidocaine. Wait 3 minutes. Monitor for signs of spinal anesthesia (apnea, profound paresthesias). If negative, slowly inject a mixture of 2 mL of 1% lidocaine and 2 mL of Celestone Soluspan (6 mg/mL).

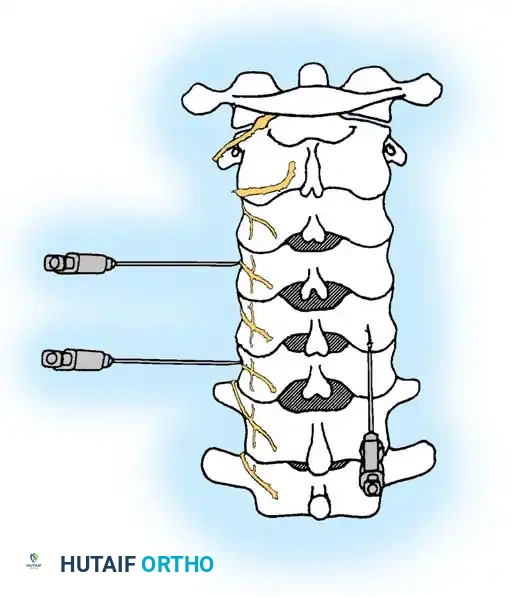
Transforaminal Approach (Technique 39-3)
🚨 SURGICAL WARNING: CERVICAL TRANSFORAMINAL INJECTIONS 🚨
At this time, many academic centers strictly avoid cervical transforaminal injections. There is an alarming increase in case reports detailing catastrophic spinal cord and brainstem infarctions following this procedure. These injuries result from inadvertent intraarterial injection of particulate steroids into a reinforcing radicular artery or the vertebral artery. If this approach is deemed absolutely necessary, it must be performed with non-particulate steroids (e.g., dexamethasone) and real-time digital subtraction angiography (DSA).
Step-by-Step Surgical Technique:
1. Positioning: Place the patient in a modified lateral decubitus position with the symptomatic side facing up. Prepare and drape the lateral neck.
2. Fluoroscopic Orientation: Identify the target neuroforamen. Tilt the C-arm slightly caudad-to-cephalad and anterior-to-posterior to maximize the visualization of the oval neuroforamen.
3. Needle Trajectory: Insert a 25-gauge, 3 ½-inch spinal needle. Advance slowly under live fluoroscopy until contact is made with the lower aspect of the superior articular process.
* Crucial Step: You must stay strictly posterior to the foramen to avoid the vertebral artery, which runs in the anterior aspect of the foramen. Orient the needle bevel notch anteriorly to force the needle tip posteriorly during advancement.

- Foraminal Entry: Redirect the needle to "walk off" the bone into the posterior foramen by 3 to 4 mm. Do not advance further medially than the midpoint of the articular pillar on the AP view.
- Contrast Flow: Remove the stylet. Aspirate vigorously. Inject 0.5 mL of nonionic contrast under live fluoroscopy. You must observe filling of the oval neuroforamen and distal flow along the exiting nerve root. If rapid vascular washout is seen, abort the procedure immediately.
- Therapeutic Injection: Once an acceptable, non-vascular dye pattern is confirmed, slowly inject 1 mL of solution (0.5 mL of 2% preservative-free lidocaine mixed with 0.5 mL of non-particulate steroid).
Thoracic Epidural Injections
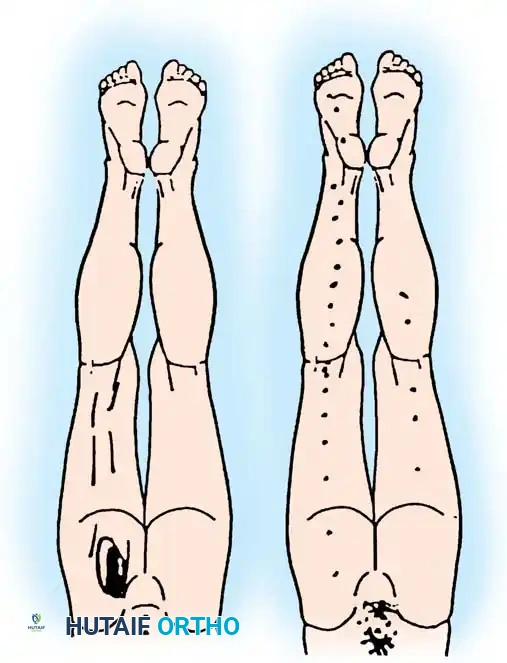
Epidural steroid injections in the thoracic spine are technically demanding due to the acute angulation of the thoracic spinous processes and the proximity of the spinal cord. However, they provide profound relief for thoracic radicular pain secondary to disc herniations, acute trauma, diabetic thoracic polyneuropathy, herpes zoster (shingles), and idiopathic thoracic neuralgia.
The interlaminar approach in the thoracic spine requires a steeper paramedian trajectory to bypass the overlapping laminae. Fluoroscopic confirmation with a lateral epidurogram is mandatory to ensure the injectate remains posterior to the thecal sac, avoiding cord compression.

Lumbar Epidural and Transforaminal Injections
Lumbar injections are the most frequently performed spinal procedures in orthopedic practice. They are highly diagnostic for isolating specific nerve root pathology in the setting of multilevel lumbar spondylosis or lateral recess stenosis.
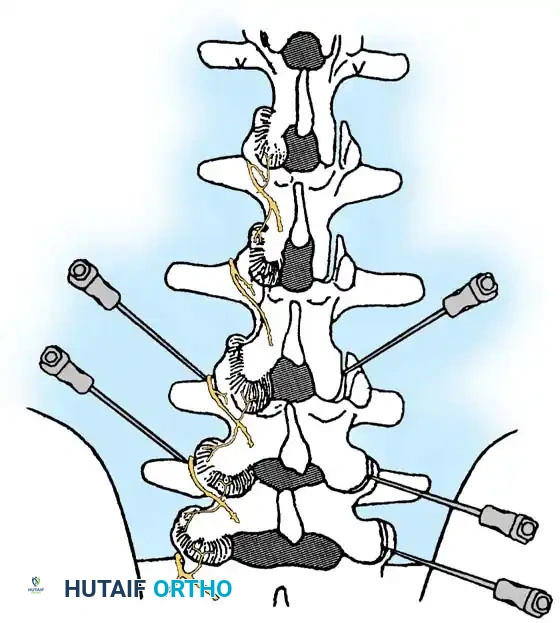
Lumbar Transforaminal Epidural Steroid Injection (TFESI)
The transforaminal approach (selective nerve root block) places the medication directly at the ventral interface between the herniated disc and the inflamed nerve root.

Key Procedural Steps:
1. Oblique Fluoroscopy: The C-arm is rotated to an ipsilateral oblique angle (typically 15-25 degrees) to visualize the "Scotty Dog" anatomy. The target is the "safe triangle" located just inferior to the pedicle (the "eye" of the Scotty Dog) and superior to the exiting nerve root.
2. Needle Placement: A 22-gauge or 25-gauge spinal needle is advanced down the beam of the fluoroscope until the tip rests in the 6 o'clock position relative to the pedicle.
3. Lateral Confirmation: The C-arm is rotated to a true lateral view to ensure the needle tip is in the superior-anterior aspect of the neuroforamen, avoiding dural puncture medially.
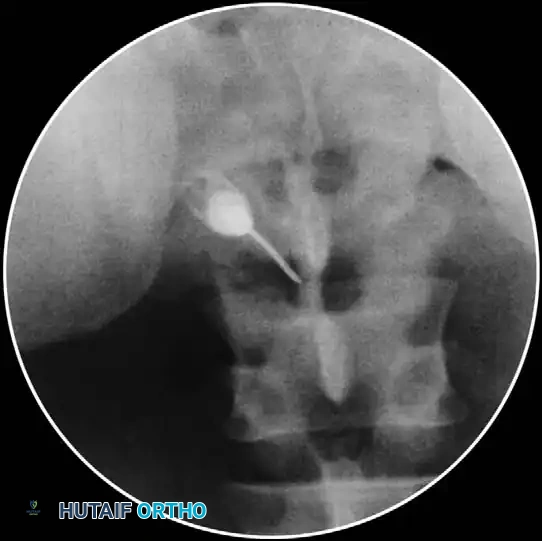
- Contrast Injection: Live fluoroscopy during contrast injection must demonstrate medial flow into the epidural space and lateral flow outlining the exiting spinal nerve.
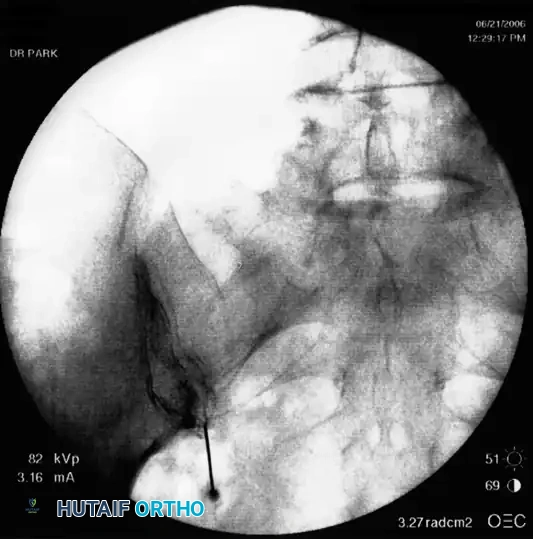
Clinical Pearl: The absence of epidural flow during a lumbar transforaminal injection often indicates severe foraminal stenosis or perineural fibrosis. In these cases, the diagnostic value is high, confirming that the nerve root is mechanically tethered and likely requires surgical decompression.

Postoperative Protocols and Complication Management
Following any spinal injection study, the patient must be transferred to a monitored recovery area.
Immediate Post-Procedure Care
- Neurological Assessment: Evaluate motor and sensory function in the extremities. Transient weakness is common due to the local anesthetic, but profound motor block requires observation until resolution.
- Hemodynamic Monitoring: Monitor blood pressure and heart rate to rule out delayed vasovagal responses or systemic anesthetic toxicity.
- Pain Diary Completion: The patient must complete the post-injection pain diary (Box 39-2) at 30 minutes, 2 hours, and 6 hours post-procedure. This data is the primary outcome measure for surgical planning.
Managing Complications
If a dural puncture occurs (evidenced by CSF return in the needle hub), the procedure at that level should be aborted. The patient should be advised of the risk of a postdural puncture headache. Conservative management includes aggressive oral hydration, caffeine supplementation, and bed rest. If the headache persists beyond 48-72 hours and is severely debilitating, an autologous epidural blood patch is the definitive treatment.