Introduction to Hip Arthroscopy
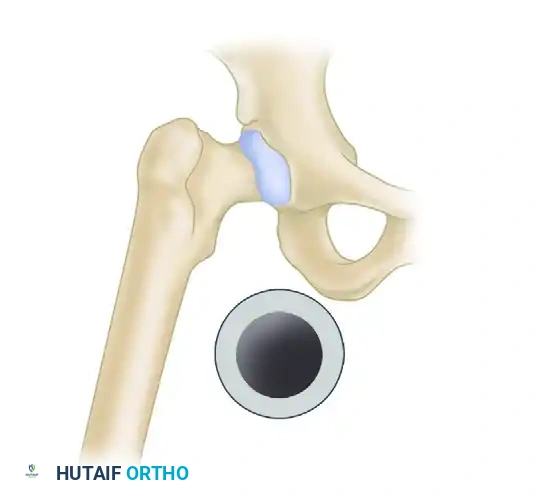
Over the past two decades, arthroscopy of the hip has evolved from a diagnostic novelty into a highly efficacious therapeutic intervention. As surgical techniques, optical technologies, and specialized instrumentation have advanced, the indications for hip arthroscopy have expanded exponentially. However, arthroscopy of the hip remains a technically demanding procedure. The inherent sphericity of the femoral head, the deep anatomical location of the joint, and the dense, highly constrained capsuloligamentous complex (comprising the iliofemoral, pubofemoral, and ischiofemoral ligaments) present unique challenges to joint access and maneuverability.
Arthroscopy of the hip provides the orthopedic surgeon with minimally invasive access to three distinct anatomical zones:
* The Central Compartment: Defined as the intra-articular space medial to the acetabular labrum. This includes the articular cartilage of the femoral head and the acetabular lunate surface, the acetabular fossa, the labrum itself, and the ligamentum teres.
* The Peripheral Compartment: Defined as the space lateral to the labrum but contained within the capsular boundaries. This includes the femoral neck, the retinacular vessels, the surrounding joint capsule, and the synovial lining.
* The Peritrochanteric Space: An extra-articular compartment that includes the greater trochanter, the gluteus medius and minimus insertions, the trochanteric bursa, and the iliotibial band.
Mastery of hip arthroscopy requires a profound understanding of three-dimensional anatomy, precise portal placement, and the biomechanics of joint distraction.
Indications and Evidence-Based Medicine
The decision to proceed with hip arthroscopy must be grounded in a meticulous clinical examination, advanced imaging (including MR arthrography or high-resolution non-contrast MRI), and a failure of conservative management.
Primary Indications
- Acetabular Labral Tears: This remains the most common indication for hip arthroscopy. Labral pathology is rarely isolated and is frequently secondary to underlying morphological abnormalities.
- Femoroacetabular Impingement (FAI): Encompassing Cam lesions (aspherical femoral head-neck junction), Pincer lesions (acetabular overcoverage), or mixed morphology. Arthroscopic osteochondroplasty and rim trimming have become the gold standard for symptomatic FAI.
- Loose Bodies: Often secondary to synovial chondromatosis, trauma, or osteochondritis dissecans.
- Chondral Lesions: Focal full-thickness cartilage defects can be addressed via debridement, microfracture, or advanced cartilage restoration techniques.
- Ligamentum Teres Pathology: Ruptures or hypertrophic fraying can cause mechanical symptoms and microinstability.
- Synovial Abnormalities: Including pigmented villonodular synovitis (PVNS) or inflammatory arthropathies requiring synovectomy.
- Extra-articular Syndromes: Snapping hip syndromes (internal/iliopsoas or external/iliotibial band) and gluteus medius/minimus tears.
- Joint Sepsis: Arthroscopic irrigation and debridement offer a less morbid alternative to open arthrotomy for septic arthritis.
Evidence-Based Clinical Pearl: According to comprehensive literature reviews, including foundational work by Stevens et al., there is fair-to-good evidence supporting hip arthroscopy in the treatment of femoroacetabular impingement. However, historically, only poor-to-fair quality evidence supported its isolated use for labral tears, extra-articular lesions, sepsis, loose bodies, and osteoarthritis. Modern high-quality randomized controlled trials (such as the FAIT and FASHIoN trials) have since provided robust Level I evidence supporting arthroscopic intervention for FAI over conservative physiotherapy. Arthroscopy in the setting of advanced osteoarthritis (Tönnis grade 2 or 3) is generally contraindicated due to poor outcomes and rapid progression to total hip arthroplasty.
Patient Positioning and General Setup
Arthroscopy of the hip can be performed with the patient in either the supine or the lateral decubitus position. Both orientations offer distinct advantages, and the choice is largely dependent on surgeon preference, institutional equipment, and specific patient factors.
The Supine Position
The supine position is the most widely utilized setup globally. It offers ease of patient positioning, excellent spatial orientation for the surgeon, and the ability to utilize a standard fracture table if a dedicated hip distractor is unavailable.

Commercially available distraction device utilized for supine hip arthroscopy, allowing for precise, micro-adjustable traction.
Advantages of Supine Positioning:
* Familiar anatomical orientation for anterior and anterolateral approaches.
* Easier airway access and management for the anesthesia team.
* Facilitates dynamic intraoperative assessment of hip range of motion (impingement testing) once traction is released.
The Lateral Decubitus Position
The lateral position is often preferred for obese patients, as the adipose tissue falls away from the lateral trochanteric region, effectively shortening the distance from the skin to the joint capsule. It may also allow easier access to the posterior joint and is advantageous when significant posterior acetabular osteophytes are present.
Advantages of Lateral Positioning:
* Gravity assists in clearing soft tissue in obese patients.
* Excellent access to the posterior and lateral peritrochanteric spaces.
* Requires specific, commercially available distraction devices adapted for the operating table.
Biomechanics of Joint Distraction
Regardless of the chosen position, accessing the central compartment requires the affected leg to be placed in longitudinal traction. The hip joint is a highly congruent ball-and-socket joint sealed by a strong capsule and a negative intra-articular pressure (the "vacuum seal").
Patient positioned supine on a fracture table with the operative leg secured in traction. Note the positioning of the perineal post.
Traction Parameters
To safely introduce 4.5-mm or 5.5-mm arthroscopic cannulas without causing iatrogenic scuffing of the femoral head or acetabular cartilage, a minimum of 10 to 12 mm of joint distraction is required.
* Force: When utilizing devices equipped with tensiometers, approximately 50 lbs (22.7 kg) of traction force is typically needed to overcome the capsular constraints and the vacuum seal.
* Time Limit: It is a strict surgical maxim that continuous traction time must be limited to less than 2 hours. Prolonged traction exponentially increases the risk of traction neurapraxia, most commonly affecting the pudendal, sciatic, and femoral nerves.
The Perineal Post and Vector Mechanics
The perineal post is the fulcrum against which traction is applied. A well-padded, often oversized perineal post must be used to distribute pressure and protect the pudendal nerve and perineal soft tissues.
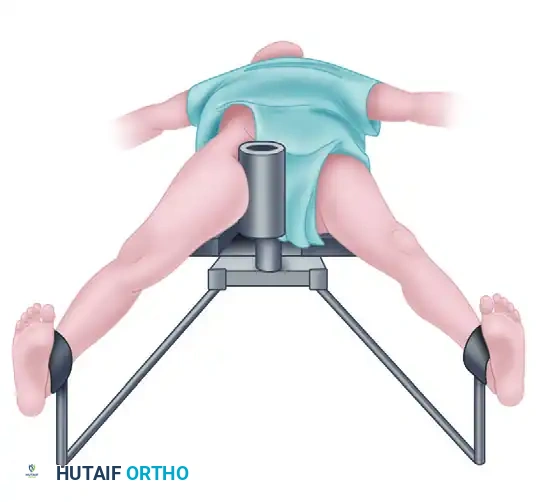
Diagram illustrating the distraction vector and pressure distribution against the perineal post. Proper lateralization of the post is critical to optimize the vector and minimize pudendal nerve compression.
Surgical Warning: The perineal post should be placed eccentrically, lateralized against the medial thigh of the operative leg rather than resting directly in the perineum. This lateralization pushes the proximal femur laterally and inferiorly, improving the vector of the traction force (distracting the head out of the acetabulum rather than just pulling it distally) and significantly decreasing the risk of pudendal neurapraxia.
Once the initial portals are established and the capsule is vented (punctured), the intra-articular vacuum seal is broken. At this stage, the surgeon should immediately reduce the traction force. Often, significantly less traction is needed to maintain the 10-12 mm of distraction after venting, thereby relieving unnecessary tension on the neurovascular structures.
Arthroscopic Equipment and Instrumentation
The depth of the hip joint and the thickness of the surrounding soft tissue envelope necessitate specialized equipment. Standard knee or shoulder arthroscopy instruments are generally of insufficient length.
- Arthroscopes: Both 30-degree and 70-degree arthroscopes are mandatory. The 70-degree scope is often considered the "workhorse" of hip arthroscopy, as it allows the surgeon to look "around the corner" of the spherical femoral head to visualize the anterior and posterior labrum and acetabular cartilage.
- Cannulas and Dilators: Extra-long, slotted cannulas are highly helpful. The slots allow for the easy introduction and exchange of curved instruments and suture anchors without losing the portal tract.
- Fluid Management: A dedicated arthroscopic fluid pump is required to maintain joint distension and clear visualization. However, fluid pressure must be carefully monitored to prevent massive fluid extravasation into the thigh or, catastrophically, into the retroperitoneal space or abdominal cavity.
Portal Anatomy and Placement
Portal placement in hip arthroscopy relies heavily on precise anatomical landmarks and extensive use of image intensification (fluoroscopy). The primary portals are established based on their relationship to the greater trochanter and major neurovascular bundles.

Surface landmarks outlined prior to portal placement: The femoral artery, vein, and nerve (medial); the greater trochanter (lateral); and the anterosuperior iliac spine (ASIS) (superior).
Standard Portals and Neurovascular Risks
-
Anterolateral (AL) Portal:
- Location: Placed 1 to 2 cm superior and 1 to 2 cm anterior to the tip of the greater trochanter.
- Significance: This is universally the first portal established because it is the safest. It enters the joint centrally and carries the lowest risk of neurovascular injury.
- Risk: The superior gluteal nerve lies approximately 4 to 6 cm superior to this portal.
-
Anterior Portal:
- Location: Placed at the intersection of a sagittal line drawn distally from the Anterior Superior Iliac Spine (ASIS) and a transverse line drawn medially from the AL portal.
- Significance: Provides excellent visualization of the anterior labrum and is the primary working portal for anterior pathology.
- Risk: The Lateral Femoral Cutaneous Nerve (LFCN) is highly variable but typically lies approximately 1.5 cm medial to this portal. Several branches of the LFCN may be even closer. The terminal branches of the ascending lateral circumflex femoral artery are also at risk. The femoral neurovascular bundle lies significantly medial to this portal.
-
Posterolateral (PL) Portal:
- Location: Placed 1 to 2 cm posterior to the tip of the greater trochanter.
- Significance: Used for viewing the posterior labrum and posterior femoral neck.
- Risk: The sciatic nerve lies approximately 2.2 to 3.0 cm posterior to this portal. To maximize safety, the hip should be placed in internal rotation during PL portal establishment, which moves the sciatic nerve further posterior and away from the trochanter.
Surgical Technique: Step-by-Step Approach
1. Accessing the Central Compartment
Under fluoroscopic guidance, a 17-gauge spinal needle is introduced via the planned Anterolateral (AL) portal trajectory. The needle is advanced aiming for the lateral edge of the acetabular sourcil.
Once the capsule is breached, a distinct "pop" is often felt. The joint is then vented, breaking the vacuum seal, which may visibly increase the joint space on fluoroscopy. Intra-articular placement is confirmed by injecting a small amount of sterile saline; backflow confirms correct positioning.
A nitinol guidewire is passed through the spinal needle. The needle is removed, and a small skin incision is made. Cannulated dilators are passed over the wire to gently spread the dense capsular tissue, followed by the introduction of the arthroscopic cannula and the 70-degree arthroscope.
The Anterior portal is then established under direct intra-articular visualization (inside-out technique) combined with fluoroscopic guidance, ensuring the needle enters the joint safely anterior to the labrum without penetrating the chondral surfaces.
2. Central Compartment Procedures
With access established, a diagnostic sweep is performed. The ligamentum teres, acetabular fossa, lunate cartilage, and labrum are systematically inspected.
* Labral Repair: Tears are debrided of non-viable tissue. The acetabular rim is prepared with a burr to create a bleeding bony bed. Suture anchors are placed, and the labrum is refixed using looped or mattress suture configurations.
* Pincer Resection: Overcoverage is addressed by trimming the bony acetabular rim using a motorized burr, often requiring detachment and subsequent refixation of the labrum.
3. Accessing the Peripheral Compartment
After completion of the central compartment procedures, the traction is completely released. The operative hip is flexed to approximately 45 degrees.
Clinical Pearl: Flexing the hip relaxes the robust iliofemoral ligament (the Y-ligament of Bigelow) and the anterior capsule. This relaxation dramatically increases the working volume of the peripheral compartment, allowing the surgeon to navigate the femoral neck safely.
The arthroscope is redirected into the peripheral compartment. This is the anatomical location for addressing Cam lesions.
4. Peripheral Compartment Procedures
- Cam Osteochondroplasty: The aspherical portion of the femoral head-neck junction is resected using a high-speed burr. The hip is dynamically rotated (internally and externally) and flexed under direct visualization to ensure adequate resection and to confirm that impingement against the acetabular rim has been eliminated.
- Capsular Management: Depending on the extent of the capsulotomy performed for access, the capsule may be left open, partially closed, or completely plicated. In patients with borderline dysplasia or generalized hyperlaxity, meticulous capsular closure is mandatory to prevent postoperative iatrogenic microinstability or dislocation.
Postoperative Protocol and Rehabilitation
Postoperative rehabilitation is highly dependent on the specific procedures performed.
* Uncomplicated Debridement/Osteochondroplasty: Patients may begin immediate weight-bearing as tolerated with crutches for 1-2 weeks to prevent fatigue falls.
* Labral Repair or Microfracture: Protected weight-bearing (typically 20 lbs flat-foot touch) is strictly enforced for 4 to 6 weeks to protect the repair or the maturing marrow clot.
* Range of Motion: Early, controlled passive range of motion (often utilizing a continuous passive motion [CPM] machine or stationary bike with zero resistance) is initiated immediately to prevent intra-articular adhesions and capsular scarring.
* Return to Play: Return to high-impact sports or pivoting activities generally requires 4 to 6 months of structured, progressive physical therapy focusing on core stability, gluteal strengthening, and proprioception.
Complications and Avoidance
While generally safe, hip arthroscopy carries a complication rate of approximately 1.5% to 5%.
1. Traction Neurapraxia: The most common complication. Avoided by limiting traction time (< 2 hours), minimizing traction force, and utilizing a well-padded, lateralized perineal post.
2. Iatrogenic Chondral/Labral Injury: Caused by poor portal trajectory or insufficient joint distraction prior to instrument insertion. Always use fluoroscopy and ensure 10-12 mm of distraction.
3. Fluid Extravasation: Can lead to scrotal/labial edema, thigh compartment syndrome, or intra-abdominal fluid accumulation. Monitor pump pressures closely and minimize surgical time.
4. Heterotopic Ossification (HO): Prophylaxis with NSAIDs (e.g., Naproxen or Indomethacin) for 2-3 weeks postoperatively is routinely recommended to prevent HO in the capsular tissues.
5. Iatrogenic Instability: Over-resection of the acetabular rim or failure to repair a large capsulotomy can lead to devastating postoperative subluxation or dislocation. Careful preoperative planning and meticulous capsular management are essential.
