Introduction & Epidemiology
Hip arthroscopy has emerged as a critical advancement in the diagnosis and treatment of intra-articular and peritrochanteric hip pathology. Historically, the hip joint, due to its deep anatomical position and inherent stability, was considered a technically challenging joint for arthroscopic intervention. However, significant progress in instrumentation, surgical techniques, and a refined understanding of hip biomechanics and pathology have broadened its indications and improved outcomes. This minimally invasive approach offers advantages over traditional open procedures, including reduced soft tissue dissection, potentially lower morbidity, and faster rehabilitation for appropriate patients.
The evolution of hip arthroscopy has largely paralleled the increased recognition of femoroacetabular impingement (FAI) as a primary etiology for early osteoarthritis and chronic hip pain in young, active individuals. FAI, characterized by abnormal contact between the proximal femur and the acetabular rim, leads to labral tears and chondral damage. Prior to widespread recognition of FAI, many patients with these symptoms were managed symptomatically or faced progression to end-stage arthritis and total hip arthroplasty. The ability to address these structural abnormalities arthroscopically represents a paradigm shift in hip preservation surgery.
Epidemiologically, hip pain is a common complaint, particularly among athletes and young adults. Studies indicate a high prevalence of FAI morphology in asymptomatic individuals, suggesting that symptomatology arises from a combination of morphology and activity levels leading to repetitive microtrauma. Labral tears are frequently encountered, often coexisting with FAI, and their incidence is reported to be substantial in populations undergoing MRI for hip pain. Conditions such as synovial chondromatosis, pigmented villonodular synovitis, and certain forms of osteonecrosis, while less common, also contribute to the spectrum of pathologies amenable to arthroscopic management. The increasing demand for active lifestyles and hip preservation underscores the growing importance of advanced arthroscopic techniques.
Surgical Anatomy & Biomechanics
A thorough understanding of the intricate anatomy and biomechanics of the hip joint is paramount for safe and effective hip arthroscopy. The hip is a diarthrodial ball-and-socket joint, designed for both stability and mobility.
Bony Anatomy
The primary bony constituents are the acetabulum of the pelvis and the femoral head.
*
Acetabulum:
Formed by the ilium, ischium, and pubis, it presents a horseshoe-shaped articular surface (lunate surface) and a non-articular acetabular fossa. The acetabular rim is crucial in FAI pathology. Acetabular orientation (anteversion, inclination) is critical, assessed by parameters such as the lateral center-edge angle (LCEA) and acetabular index. Pincer impingement results from excessive acetabular coverage.
*
Femoral Head and Neck:
The femoral head articulates with the acetabulum. The femoral neck connects the head to the shaft, and its morphology, particularly the head-neck junction, is central to cam impingement. An increased alpha angle on imaging indicates a reduced head-neck offset, contributing to cam-type FAI.
Soft Tissue Structures
- Articular Cartilage: Covers the lunate surface of the acetabulum and the femoral head, providing a low-friction articulating surface. Chondral lesions are common findings in FAI and traumatic injuries.
- Acetabular Labrum: A fibrocartilaginous rim that attaches to the acetabular rim, deepening the socket and contributing to the suction seal of the joint. It is richly innervated and vascularized, particularly at its periphery. Tears are a common cause of mechanical hip pain.
-
Joint Capsule:
Composed of three strong ligaments:
- Iliofemoral Ligament (Y ligament of Bigelow): The strongest ligament, preventing hyperextension.
- Pubofemoral Ligament: Prevents excessive abduction and external rotation.
-
Ischiofemoral Ligament:
Limits internal rotation and extension.
These ligaments contribute significantly to hip stability and are often partially released during capsulotomy for improved visualization and then repaired.
- Ligamentum Teres: Originates from the acetabular fossa and inserts into the fovea of the femoral head. Its role in adult hip stability is debated, but it contains a small artery (foveal artery) that contributes to femoral head vascularity, particularly in children. Tears can be a source of pain.
- Synovium: Lines the non-articular surfaces of the joint capsule. Synovial pathology, such as pigmented villonodular synovitis (PVNS) or synovial chondromatosis, can be addressed arthroscopically.
Neurovascular Structures
The proximity of vital neurovascular structures necessitates meticulous portal placement and surgical technique to prevent iatrogenic injury.
*
Femoral Nerve, Artery, and Vein:
Located anteriorly, medial to the anterolateral portal, deep to the iliopsoas muscle.
*
Lateral Femoral Cutaneous Nerve (LFCN):
Superficial, crosses the anterior hip, susceptible to injury from portals, traction, or even compression from edema.
*
Sciatic Nerve:
Posteriorly, deep to the gluteus maximus, at risk with posterior portals or excessive traction, particularly in extension.
*
Pudendal Nerve:
Can be compressed by the perineal post on the traction table, leading to temporary or rarely permanent sensory or motor deficits.
*
Gluteal Nerves and Vessels:
Superior and inferior gluteal neurovascular bundles are relevant for peritrochanteric procedures.

Biomechanics
- Stability: The hip joint's stability is derived from its bony configuration, strong capsular ligaments, muscular support, and the labral suction seal.
- Impingement: FAI occurs when incongruent bony morphology at the head-neck junction (cam) or acetabular rim (pincer) leads to abnormal contact during hip motion, particularly flexion and internal rotation. This repetitive microtrauma to the labrum and articular cartilage is thought to initiate a cascade of degenerative changes.
- Labral Function: The labrum deepens the acetabulum, increases the contact area, contributes to fluid pressure regulation, and creates a suction seal, which is critical for joint lubrication and stability. Tears compromise this seal, leading to instability and increased stress on the articular cartilage.

Indications & Contraindications
Patient selection is critical for successful outcomes in hip arthroscopy. Indications have broadened considerably, while contraindications aim to prevent poor results or iatrogenic harm.
Indications for Hip Arthroscopy
The primary indications revolve around pathologies causing mechanical symptoms, pain, and functional limitation, where non-operative management has failed.
-
Labral Tears:
- Often associated with FAI, trauma, or dysplasia.
- Symptoms include groin pain, clicking, catching, or giving way.
- Imaging: MRA is the gold standard.
-
Treatment: Repair (preferred, especially for FAI-related tears), or debridement for irreparable tears or calcified lesions.

-
Femoroacetabular Impingement (FAI):
-
Cam Impingement:
Abnormal morphology of the femoral head-neck junction (pistol grip deformity), leading to abutment against the acetabular rim, particularly in flexion and internal rotation.
-
Imaging: Increased alpha angle on lateral radiographs or MRI.
-
Imaging: Increased alpha angle on lateral radiographs or MRI.
-
Pincer Impingement:
Overcoverage of the femoral head by the acetabulum. Can be global or focal (e.g., retroversion).
- Imaging: Crossover sign, deep acetabulum, or increased LCEA on radiographs.
- Mixed Impingement: Combination of cam and pincer lesions, most common.
- Treatment: Femoral osteochondroplasty for cam lesions, acetabular rim trimming (cheilectomy) for pincer lesions, often combined with labral repair.
-
Cam Impingement:
Abnormal morphology of the femoral head-neck junction (pistol grip deformity), leading to abutment against the acetabular rim, particularly in flexion and internal rotation.
-
Chondral Lesions:
- Articular cartilage damage, often secondary to FAI or trauma.
- Diagnosis: MRI. Arthroscopy allows direct visualization and staging.
- Treatment: Debridement for unstable flaps, microfracture for focal full-thickness defects (<2-3 cm²), rarely chondroplasty. Large or diffuse lesions are less amenable to successful arthroscopic intervention.
-
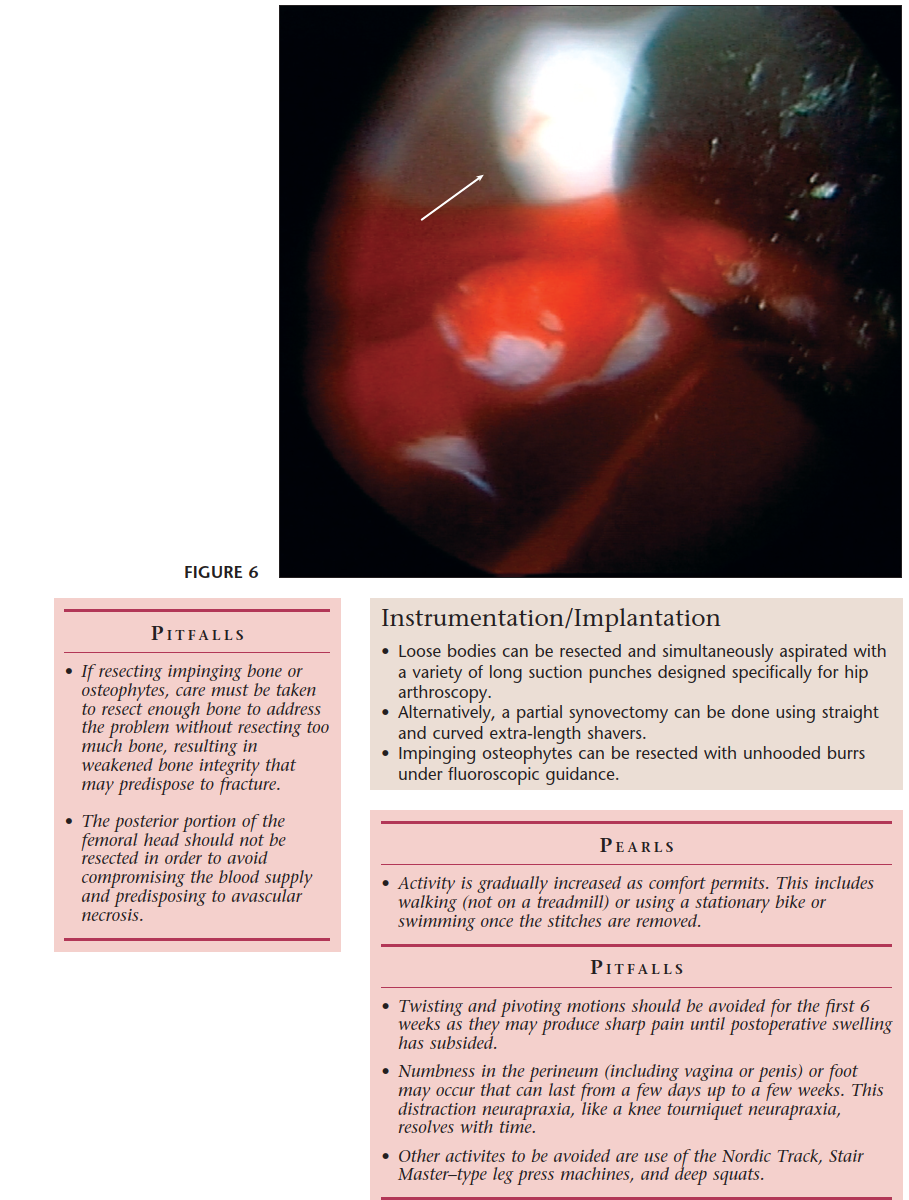
Loose Bodies:
- Cartilaginous or osteochondral fragments within the joint, causing mechanical symptoms (locking, catching).
- Etiology: Osteochondral fractures, synovial chondromatosis, degenerative changes.
- Treatment: Arthroscopic retrieval.
-
Synovial Diseases:
- Synovial Chondromatosis: Metaplastic cartilaginous nodules within the synovium, which can detach and become loose bodies.
- Pigmented Villonodular Synovitis (PVNS): Benign proliferative disorder of the synovium, causing pain and effusions.
- Inflammatory Arthropathy: Diagnostic arthroscopy for synovial biopsy.
- Treatment: Synovectomy, loose body removal.
-
Trauma:
- Post-traumatic arthrofibrosis, adhesions, or specific osteochondral fractures.
- Treatment: Debridement, lysis of adhesions, fragment removal.
-
Crystalline Diseases (Gout, Pseudogout):
- Rarely, diagnostic arthroscopy may be indicated for synovial biopsy and crystal identification in atypical presentations.
-
Early-stage Osteonecrosis (ONFH):
- Core decompression for pre-collapse stages of ONFH. Arthroscopy can be combined to confirm diagnosis and decompress.
-
Peritrochanteric Space Pathology:
- Gluteus Medius/Minimus Tears: Refractory gluteal tendinopathy or partial/full-thickness tears.
- Trochanteric Bursitis: Chronic, refractory cases.
- Iliotibial Band (ITB) Friction Syndrome: External snapping hip.
- Ischiofemoral Impingement: Quadratus femoris pathology.
- Treatment: Endoscopic repair of gluteal tendons, bursectomy, ITB release, decompression of the ischiofemoral space.
-
Snapping Hip Syndrome:
- Internal: Iliopsoas tendon snapping over the iliopectineal eminence. Arthroscopic iliopsoas release (Z-lengthening) for refractory cases.
- External: ITB snapping over the greater trochanter (addressed in peritrochanteric pathology).
-
Diagnostic Arthroscopy:
- When clinical examination and advanced imaging (MRI/MRA) are inconclusive but suspicion for intra-articular pathology remains high, and symptoms are functionally limiting.
Table of Operative vs. Non-Operative Indications
| Pathology | Primary Non-Operative Management | Primary Operative (Arthroscopic) Indication |
|---|---|---|
| Femoroacetabular Impingement | Activity modification, physical therapy, NSAIDs, corticosteroid injections | Symptomatic FAI with structural deformity (cam/pincer) unresponsive to conservative care |
| Labral Tears | Activity modification, physical therapy, NSAIDs, intra-articular injections | Symptomatic tears causing mechanical pain (clicking, catching) |
| Chondral Lesions | Activity modification, physical therapy, NSAIDs, injections | Focal, contained lesions causing mechanical symptoms, suitable for microfracture/debridement |
| Loose Bodies | N/A (mechanical symptoms often necessitate removal) | Symptomatic loose bodies (locking, catching, pain) |
| Synovial Chondromatosis/PVNS | N/A | Symptomatic disease (pain, effusion, mechanical symptoms) requiring synovectomy/removal |
| Ligamentum Teres Tears | Activity modification, physical therapy | Symptomatic tears with instability or persistent pain after conservative measures |
| Peritrochanteric Pain Syndrome | Physical therapy, activity modification, NSAIDs, injections | Refractory symptoms, gluteal tendon tears amenable to repair, recalcitrant bursectomy |
| Snapping Hip (Iliopsoas) | Physical therapy, stretching, injections | Refractory symptomatic snapping after failed conservative management |
| Early-stage Osteonecrosis | Activity modification, bisphosphonates | Pre-collapse ONFH (e.g., Ficat Stage I/II) for core decompression |
Contraindications for Hip Arthroscopy
Absolute contraindications are few, but relative contraindications require careful consideration of risk-benefit.
-
Advanced Degenerative Joint Disease (Osteoarthritis):
- Tönnis Grade 2-3, or significant joint space narrowing on radiographs, indicates poor outcomes with hip arthroscopy. Patients are better candidates for total hip arthroplasty.
-

-
Severe Hip Dysplasia:
- Lateral center-edge angle (LCEA) < 20°. Arthroscopy in dysplastic hips may exacerbate instability. Periacetabular osteotomy (PAO) is often a more appropriate intervention.
-
Active Infection:
- Systemic or local infection at the surgical site. Diagnostic aspiration and culture are appropriate, but elective arthroscopy is deferred.
-
Systemic Coagulopathy:
- Uncorrected bleeding disorders.
-
Significant Medical Comorbidities:
- Patients medically unfit for anesthesia or prolonged traction.
-
Unrealistic Patient Expectations:
- Crucial for managing patient satisfaction and defining success.
-
Morbid Obesity:
- Can complicate traction, portal placement, visualization, and rehabilitation (relative contraindication).
-
Skeletal Immaturity with Open Physes:
- Relative contraindication for procedures involving osteochondroplasty, due to risk of growth disturbance.
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and precise patient positioning are fundamental for the successful and safe execution of hip arthroscopy.
Pre-Operative Planning
-
Patient Evaluation:
- History: Detailed account of pain characteristics (location, quality, duration, exacerbating/alleviating factors), mechanical symptoms (clicking, locking, giving way), previous treatments, and functional limitations.
-
Physical Examination:
- Gait analysis.
- Range of Motion (ROM): Assess for limitations, especially in flexion and internal rotation (classic for FAI).
-
Specific Impingement Tests:
- FADIR test (Flexion, Adduction, Internal Rotation): Reproduces anterior impingement pain.
- FABER test (Flexion, Abduction, External Rotation): Assesses for hip internal pathology, iliopsoas pathology, or sacroiliac joint dysfunction.
- McCarthy Sign: Provocative test for labral tears.
- Trochanteric palpation, muscle strength, neurovascular status.
-
Imaging:
-
Standard Radiographs:
Essential for bony morphology.
- Anteroposterior (AP) pelvis: Assess LCEA, acetabular inclination, Tönnis grade, crossover sign for acetabular retroversion.
- Cross-table lateral (or 90° Dunn view): Assess femoral head-neck offset and alpha angle for cam impingement.
- False profile view: Assesses anterior acetabular coverage.
-
Magnetic Resonance Imaging (MRI) / Magnetic Resonance Arthrography (MRA):
- MRA with intra-articular contrast is the gold standard for evaluating labral tears, chondral lesions, and ligamentum teres pathology.
-
MRI can also assess for synovial abnormalities, bone edema, and soft tissue pathology (e.g., gluteal tendinopathy).

-
Computed Tomography (CT) / 3D CT Reconstruction:
- Valuable for complex FAI morphology, precise planning of osteochondroplasty, and assessment of torsion.
- Provides detailed bony architecture not fully appreciated on radiographs.
-
Standard Radiographs:
Essential for bony morphology.
-
Anesthesia Consultation: Evaluate patient fitness for general anesthesia and potential regional nerve blocks (e.g., fascia iliaca block) for post-operative pain management.
-
Informed Consent: Detailed discussion of the procedure, potential benefits, risks (neurovascular injury, infection, HO, fluid extravasation, failure to relieve symptoms), alternatives, and post-operative expectations.
Patient Positioning
The most common position for hip arthroscopy is the supine position on a specialized traction table.
-
Table Setup:
- Patient is placed supine on a fracture table or traction table.
- Adequate padding is crucial at all pressure points (heels, sacrum, elbows, shoulders) to prevent nerve palsies and skin breakdown.
- A well-padded perineal post is essential to provide counter-traction. Careful placement to avoid pudendal nerve compression or skin breakdown in the perineum.
- Both feet are secured in traction boots. The operative leg is positioned for distraction, while the non-operative leg is typically in slight abduction and flexion to facilitate C-arm access.
-
Traction:
- Distraction: Longitudinal traction is applied to the operative leg to create sufficient space between the femoral head and acetabulum to safely introduce arthroscopic instruments into the central compartment. This usually requires 25-50 lbs of traction.
- Fluoroscopic Guidance: An image intensifier (C-arm) is used to confirm adequate distraction. A minimum of 7-10 mm of joint space is typically aimed for. Ensure the femoral head is centered in the acetabulum to avoid excessive stress on the labrum or articular cartilage.
- Duration: Traction time should be minimized, typically < 2 hours, to reduce risks of neurapraxia (e.g., pudendal nerve, LFCN). Intermittent periods of traction release can be considered.
- Hip Position: The hip is typically positioned in 10-20 degrees of flexion and slight abduction to open the anterior aspect of the joint and facilitate portal placement. Internal rotation can further open the joint space anteriorly.
-
C-arm Positioning:
- The C-arm is draped sterilely and positioned to allow unobstructed fluoroscopic views in both AP and lateral planes (cross-table or true lateral) throughout the procedure. This is critical for portal placement and verifying bony resections.
-
Sterile Preparation and Draping:
- The entire operative leg, hip, and ipsilateral abdomen are prepared with an antiseptic solution and sterilely draped to create a wide surgical field.

Detailed Surgical Approach / Technique
Hip arthroscopy involves a systematic approach, often divided into central compartment, peripheral compartment, and sometimes peritrochanteric space procedures.
Portal Placement and Joint Access
Accurate portal placement, typically guided by fluoroscopy and anatomical landmarks, is crucial to minimize neurovascular risk and optimize visualization and instrument maneuverability.
-
Landmarking:
- Anatomical landmarks are marked: Anterior Superior Iliac Spine (ASIS), greater trochanter (GT), pubic symphysis.
- Fluoroscopy is used to identify the femoral head, acetabular rim, and femoral neck.
- A line drawn from ASIS to the anterior margin of the GT helps guide anterior portal placement.
-
Standard Portals for Central Compartment:
-
Anterolateral Portal (AL):
Typically 2-3 cm anterior and 2-3 cm superior to the tip of the GT. Used for initial visualization, inflow, and instrument access. Located within the safe zone, avoiding the LFCN which often lies more medially.

- Mid-Anterior Portal (MAP): Typically 1-2 cm anterior to the AL portal, inferior to the ASIS. Used for instrument access, often primary working portal for labral repair and FAI. Care must be taken to avoid the femoral neurovascular bundle, which lies medial to this portal.
- Distal Anterolateral Portal (DAL): More distal and lateral to the AL, often used for cam resection, providing a better angle for osteochondroplasty.
-
Anterolateral Portal (AL):
Typically 2-3 cm anterior and 2-3 cm superior to the tip of the GT. Used for initial visualization, inflow, and instrument access. Located within the safe zone, avoiding the LFCN which often lies more medially.
-
Technique for Portal Creation (Outside-in):
- Skin incision, blunt dissection to the capsule (or fascia for peripheral compartment).
- A spinal needle is inserted under fluoroscopic guidance into the central compartment to confirm position.
- An obturator and cannula system are then advanced, ensuring an intra-articular position.
- Initial Distraction and Cannula Placement: After confirmation of adequate distraction on fluoroscopy, the AL portal is often established first. A spinal needle is used to target the joint, followed by a blunt trocar to minimize iatrogenic chondral damage.
- Inflow: An arthroscopic pump maintains continuous saline inflow for joint distension and clear visualization, typically at pressures of 50-80 mmHg.
Diagnostic Arthroscopy of the Central Compartment
Once cannulated, a systematic diagnostic arthroscopy is performed to confirm and fully delineate all intra-articular pathologies.
-
Central Compartment:
- Articular Cartilage: Inspect the femoral head and acetabulum for chondral lesions (fibrillation, delamination, full-thickness defects), using probes to assess stability.
-
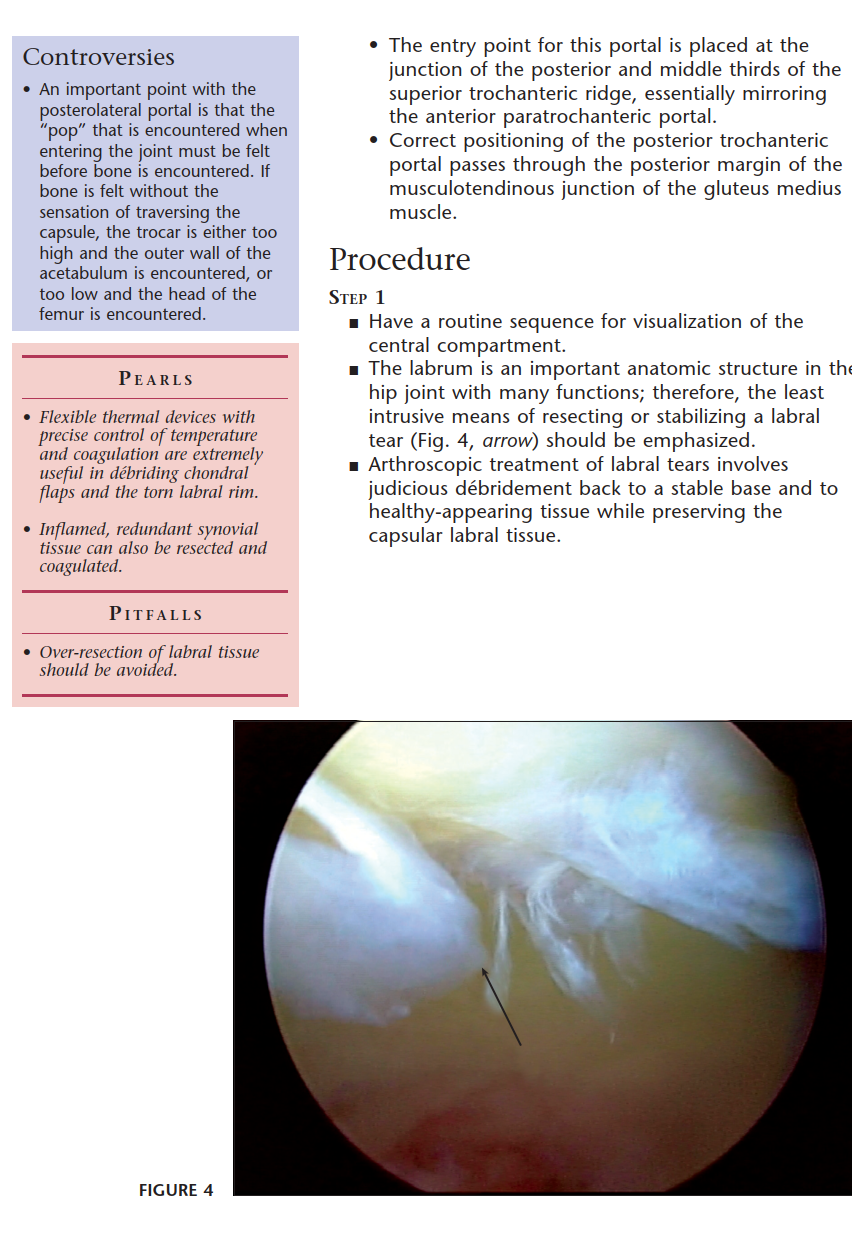
Labrum:
Evaluate for tears (radial, longitudinal, avulsion), degeneration, and detachment. Assess the labral-chondral junction.

- Ligamentum Teres: Assess for tears, hypertrophy, or impingement.
- Synovium: Inspect for signs of inflammation, synovitis, loose bodies, or synovial proliferation (PVNS, synovial chondromatosis).
- Capsule: Assess for integrity and signs of laxity.
Addressing Pathology (Central Compartment)
-
Labral Tears:
- Debridement: For irreparable tears, degenerated tissue, or calcified labrum, minimal debridement to a stable rim is performed.
-
Repair/Refixation:
Preferred treatment for FAI-related tears, especially when the labrum is healthy and detachable from the acetabular rim.
- Suture anchors (typically 2-4) are placed into the acetabular rim.
-
Non-absorbable sutures are passed through the labrum and tied to re-fix it to the rim, restoring the suction seal and anatomy.

-
Femoroacetabular Impingement (FAI) Correction:
-
Acetabular Rim Trimming (Pincer Lesion):
- Under fluoroscopic guidance, the prominent acetabular rim is resected using a burr, typically from the 12 o'clock to 3 o'clock position (right hip).
- Care is taken to avoid over-resection, which can lead to iatrogenic dysplasia, and to protect the labrum.
-
Adequate decompression is confirmed by dynamic impingement testing intra-operatively.
-
Femoral Osteochondroplasty (Cam Lesion):
- Traction is released to enter the peripheral compartment (see below).
- The prominent aspect of the femoral head-neck junction is resected using a burr.
- Fluoroscopy is used to guide the resection, confirming restoration of the head-neck offset and reduction of the alpha angle.
-
Dynamic impingement testing in the central compartment confirms adequate bony resection without impingement in provocative positions.

-
Acetabular Rim Trimming (Pincer Lesion):
-
Chondral Lesions:
- Debridement: Unstable chondral flaps are débrided to a stable edge.
-
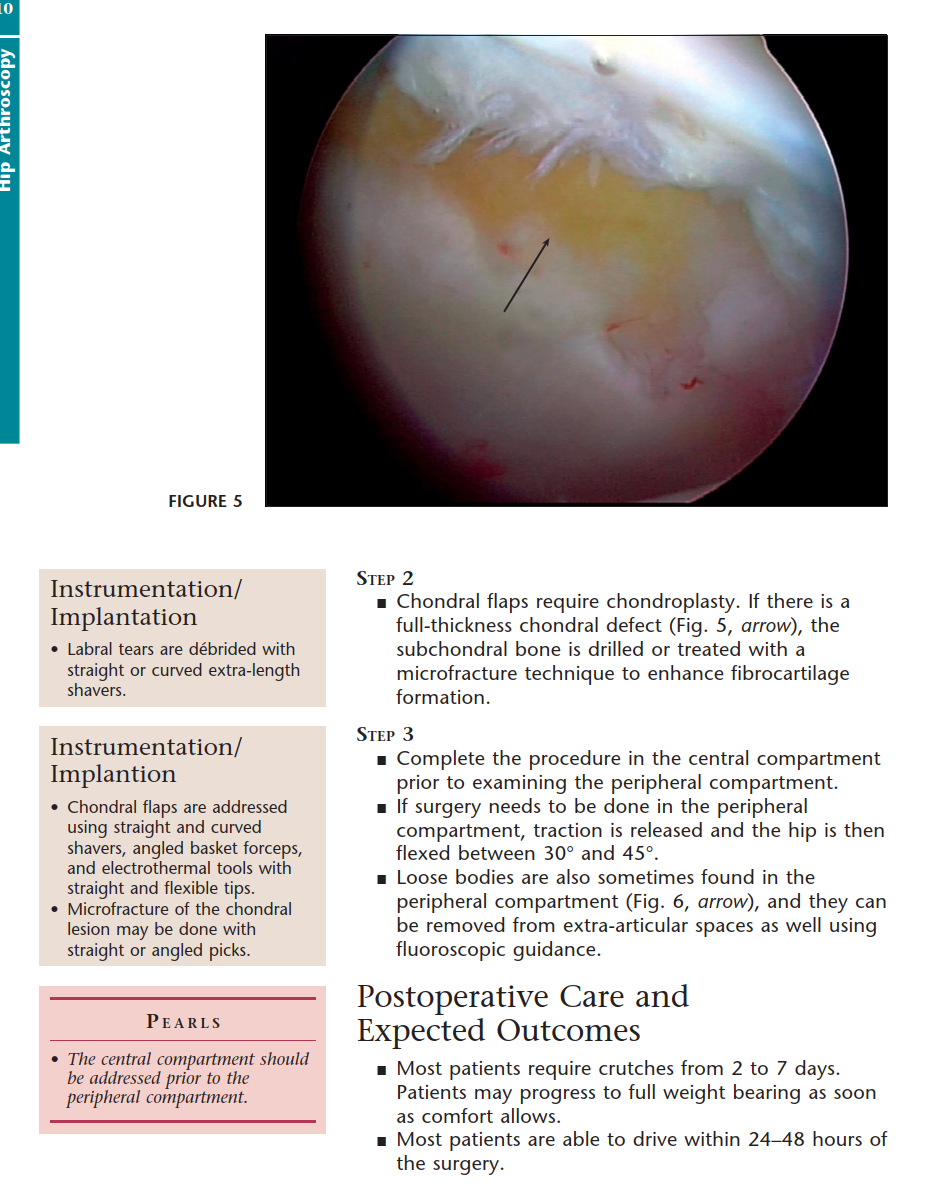
Microfracture:
For focal full-thickness chondral defects (<2-3 cm²), subchondral bone is penetrated with an awl to promote fibrocartilage formation.

-
Loose Body Removal: Identified fragments are grasped and extracted.

-
Synovectomy: Partial or complete synovectomy for PVNS, synovial chondromatosis, or inflammatory synovitis using a shaver.
Peripheral Compartment Procedure
After central compartment work, traction is released, and the hip is positioned in slight flexion, abduction, and external rotation (FABER-like position) to open the peripheral compartment.
-
Peripheral Compartment Portals:
- Often utilize existing portals or accessory portals.
- The camera can be moved to a different portal to optimize visualization of the peripheral compartment (e.g., using an anterolateral portal for camera, and a distal anterolateral for instruments).
- The interval between the rectus femoris and iliopsoas, or between the iliofemoral ligament and the iliopsoas tendon, is often the entry point.
-
Diagnostic Arthroscopy of Peripheral Compartment:
- Inspect the femoral neck, femoral head-neck junction, and the anterior capsule.
- Assess for impingement lesions not fully addressed in the central compartment.
- Iliopsoas tendon: Assess for signs of snapping or tendinopathy.
-
Addressing Pathology (Peripheral Compartment):
- Femoral Osteochondroplasty: This is where cam resection (as described above) is primarily performed.
-
Capsulotomy/Capsular Repair:
- A capsulotomy (e.g., T-capsulotomy, interportal capsulotomy) is often performed to facilitate visualization and access to the central compartment, especially for FAI correction.
-
Current practice increasingly favors capsular repair or plication after central compartment work, particularly in patients with borderline dysplasia or ligamentous laxity, to restore stability and minimize post-operative microinstability. Suture anchors are placed into the acetabular rim, and sutures are passed through the capsule.

- Iliopsoas Tendon Release: For refractory internal snapping hip, a fractional lengthening or tenotomy can be performed.
Peritrochanteric Space Arthroscopy
This involves distinct portals and is performed without traction, typically in a lateral decubitus position, but can also be done in supine.
-
Portals:
- Typically two or three portals over the greater trochanter, ensuring a wide working space.
- Landmarks: Greater trochanter, ITB.
-
Pathologies Addressed:
- Gluteus Medius/Minimus Tears: Endoscopic repair using suture anchors.
- Trochanteric Bursitis: Bursectomy.
- Iliotibial Band (ITB) Release: For refractory external snapping hip.
- Ischiofemoral Impingement: Decompression of the quadratus femoris space by resection of bone from the lesser trochanter or ischium.
Closure
- After completion of all procedures, ensure thorough lavage of the joint.
- The capsule, if opened, is often repaired (especially with T-capsulotomy) using suture anchors or direct repair to prevent iatrogenic instability.
- All portals are closed with sutures or adhesive strips.
- A sterile dressing is applied.
- Fluid management: Careful monitoring of inflow and outflow to minimize fluid extravasation.
Complications & Management
While hip arthroscopy is generally safe, potential complications can arise, requiring prompt recognition and appropriate management.
Common Complications and Management Strategies
| Complication | Incidence (Approximate) | Etiology/Mechanism | Management / Salvage Strategy |
|---|---|---|---|
| Iatrogenic Chondrolabral Injury | 5-15% | Poor portal placement, instrument impingement, uncontrolled distraction | Prevention: Careful portal placement, protective cannulas. Treatment: Debridement, microfracture if full-thickness. |
| Nerve Injury | |||
| Pudendal Nerve Neurapraxia | 1-5% | Compression by perineal post, prolonged traction | Prevention: Proper padding, minimal traction time. Treatment: Usually resolves spontaneously; severe cases rare, consider nerve block. |
| Lateral Femoral Cutaneous Nerve | 2-10% | Direct trauma from anterolateral portal, traction, thermal injury, fluid extravasation | Prevention: Careful portal placement, blunt dissection. Treatment: Usually resolves; gabapentin/nerve block for persistent symptoms. |
| Sciatic Nerve Neurapraxia | <1% | Excessive traction, posterior portal placement, hip extension during traction | Prevention: Limit traction time/force, avoid extreme hip positions. Treatment: Immediate traction release; observation. |
| Femoral Nerve/Vessel Injury | <0.1% | Medial placement of anterior portals, deep penetration | Prevention: Fluoroscopic guidance, blunt dissection, awareness of anatomy. Treatment: Urgent vascular/neurological consult. |
| Fluid Extravasation | 5-20% (minor) | Prolonged high pump pressure, capsular defects, communication with other spaces | Prevention: Minimize pump pressure, limit traction time, meticulous capsular closure. Treatment: Discontinue traction, observation, rarely drainage. |
| Infection (Septic Arthritis) | <0.5% | Breach in sterile technique | Prevention: Standard sterile technique, prophylactic antibiotics. Treatment: Urgent arthroscopic washout, debridement, IV antibiotics. |
| Heterotopic Ossification (HO) | 1-5% (post-op, mild) | Periosteal trauma, FAI resections (especially cam), male gender, prior HO history | Prevention: NSAIDs (Indomethacin) post-op for 3-6 weeks, radiation (controversial). Treatment: Excision if symptomatic and mature. |
| Thromboembolic Events (DVT/PE) | <0.5% | Prolonged immobilization, patient comorbidities | Prevention: Early mobilization, chemical prophylaxis (aspirin) per protocol. Treatment: Anticoagulation. |
| Post-operative Pain | Common (variable) | Surgical trauma, residual inflammation, persistent pathology | Prevention: Meticulous technique, multimodal analgesia. Treatment: PT, injections, nerve blocks, rarely revision surgery. |
| Adhesions/Arthrofibrosis | 1-3% | Insufficient post-op motion, inflammatory response | Prevention: Aggressive rehabilitation, early motion. Treatment: MUA (Manipulation Under Anesthesia), rarely revision arthroscopy. |
| Failure to Relieve Symptoms / | 10-20% | Incorrect diagnosis, inadequate decompression, progression of underlying OA | Re-evaluation of diagnosis, imaging. Revision arthroscopy or open surgery. Consideration of joint replacement. |
| Progression of OA |
Management Principles
- Prevention: The cornerstone of complication management. This includes meticulous pre-operative planning, precise surgical technique, appropriate patient positioning, limited traction time, and judicious use of arthroscopic pumps. Prophylactic measures (e.g., NSAIDs for HO, DVT prophylaxis) are often employed.
- Early Recognition: Vigilance for signs and symptoms of complications post-operatively.
- Prompt Intervention: Timely management is crucial for optimal outcomes. For severe complications like infection or significant neurovascular injury, immediate re-intervention may be required.
- Multidisciplinary Approach: Collaboration with neurologists, vascular surgeons, or infectious disease specialists as needed.
Post-Operative Rehabilitation Protocols
A structured and progressive post-operative rehabilitation protocol is integral to optimizing outcomes following hip arthroscopy. Protocols are tailored to the specific procedures performed (e.g., labral repair vs. debridement, capsular repair, microfracture, cam/pincer resection) and the surgeon's preferences. The overarching goals are to protect healing tissues, restore range of motion (ROM), improve strength, and facilitate a safe return to activity.
General Principles
- Tissue Protection: Adherence to weight-bearing restrictions and ROM precautions to protect repaired structures (labrum, capsule) or healing cartilage (microfracture).
- Pain and Edema Control: Early focus on reducing post-operative pain and swelling through RICE (rest, ice, compression, elevation), pain medication, and modalities.
- Progressive Loading: Gradual increase in stress on the joint and surrounding musculature.
- Neuromuscular Control: Emphasis on restoring proprioception, balance, and motor control.
- Patient Education: Crucial for compliance and understanding the rationale behind each phase.
Phased Rehabilitation Approach
Phase I: Protection & Early Motion (Weeks 0-6)
Goals: Protect surgical repairs, minimize pain/inflammation, establish basic neuromuscular control, achieve early, controlled range of motion.
-
Weight Bearing:
- Labral Repair/Microfracture/Capsular Repair: Typically Non-Weight Bearing (NWB) or Touch-Down Weight Bearing (TDWB) with crutches for 2-4 weeks. Gradually progress to Partial Weight Bearing (PWB) (25-50%) from weeks 4-6.
- Debridement/Cam/Pincer Resection Only: PWB or Weight Bearing As Tolerated (WBAT) immediately post-op, often with crutches for comfort for 1-2 weeks.
-
Range of Motion:
- Passive ROM (PROM): Continuous Passive Motion (CPM) machine often used for 4-6 hours daily for 4-6 weeks to promote chondral health and prevent adhesions.
- Controlled Active-Assisted ROM (AAROM) and Active ROM (AROM): Within pain-free limits.
- Precautions: Avoid combined hip flexion > 90°, adduction past midline, and internal rotation for 4-6 weeks to protect labral and capsular repairs. Avoid active hip flexion against resistance if iliopsoas release was performed.
-
Therapeutic Exercises:
- Gluteal sets, quadriceps sets, ankle pumps.
- Gentle hip abduction (isometric or non-weight bearing).
- Core stabilization exercises (gentle transversus abdominis activation).
- Upper body conditioning.
Phase II: Controlled Progression (Weeks 6-12)
Goals: Restore full, pain-free ROM; progress to full weight bearing; begin moderate strengthening; improve gait mechanics.
- Weight Bearing: Progress to full weight bearing and discontinue crutches as tolerated, ensuring good gait mechanics.
- Range of Motion: Progress to full AROM in all planes, respecting any specific precautions.
-
Therapeutic Exercises:
-
Strengthening:
- Isometric hip strengthening (flexion, extension, abduction, adduction, internal/external rotation).
- Progress to light resistance exercises: supine abduction/adduction, clam shells, side-lying leg lifts.
- Mini-squats, lunges (shallow, controlled).
- Glute bridge progression.
- Core Strengthening: Plank, bird-dog, anti-rotation exercises.
- Proprioception/Balance: Single-leg stance, wobble board activities.
- Stationary cycling (no resistance initially), elliptical trainer.
-
Strengthening:
Phase III: Advanced Strengthening & Return to Activity (Weeks 12-24+)
Goals: Achieve maximum strength and endurance, restore dynamic stability, perform sport-specific activities, safe return to high-impact activities.
-
Therapeutic Exercises:
- Progressive Resistance: Increase intensity and load of strengthening exercises.
- Functional Exercises: Step-ups, plyometric exercises (box jumps, hopping), agility drills.
- Sport-Specific Training: Gradually introduce movements and drills specific to the patient's desired activities or sport.
- Running Progression: Begin with walk-jog intervals, gradually increasing duration and intensity.
- Continue advanced core strengthening and balance exercises.
-
Return to Sport Criteria:
Typically not before 4-6 months, and depends on objective criteria:
- Pain-free full ROM.
- Absence of impingement signs.
- No tenderness with palpation.
- Isokinetic strength testing (limb symmetry index > 85-90%).
- Completion of sport-specific functional testing.
- Patient confidence.
Specific Considerations
- Capsular Repair/Plication: May require more restrictive ROM precautions in early phases to protect capsular integrity.
- Microfracture: Strict NWB and CPM compliance are critical for cartilage healing.
- Iliopsoas Tenotomy: Avoid active hip flexion against resistance for 4-6 weeks to allow tendon healing/lengthening.
- Gluteal Tendon Repair: NWB/TDWB for 4-6 weeks, avoid active hip abduction initially.
Successful rehabilitation hinges on close communication between the surgeon, physical therapist, and patient, with regular reassessment and adaptation of the protocol based on individual progress and response to treatment.

Summary of Key Literature / Guidelines
The evidence base for hip arthroscopy has grown substantially, supporting its role in hip preservation, particularly for FAI and associated labral pathology.
Efficacy of Hip Arthroscopy for FAI and Labral Tears
- Randomized Controlled Trials (RCTs): Several high-quality RCTs, such as the ANCHOR study and the FASHION trial, have demonstrated superior outcomes for hip arthroscopy combined with physical therapy compared to physical therapy alone in patients with symptomatic FAI. These trials consistently report significant improvements in patient-reported outcome measures (PROMs) such as the modified Harris Hip Score (mHHS), Hip Outcome Score (HOS), and International Hip Outcome Tool (iHOT-33/12).
- Systematic Reviews and Meta-analyses: These studies generally support the effectiveness of hip arthroscopy for improving pain and function in appropriately selected patients with FAI and labral tears. Outcomes are generally favorable for patients without significant pre-existing osteoarthritis.
- Long-Term Outcomes: While long-term data (>10 years) are still maturing, existing studies suggest that hip arthroscopy can delay or potentially prevent the progression to total hip arthroplasty in a significant proportion of patients, especially those with minimal pre-existing chondral damage. However, a subset of patients, particularly those with advanced chondral lesions, may still require arthroplasty within 5-10 years.
Key Factors Influencing Outcomes
- Pre-operative Osteoarthritis: The most consistent predictor of poor outcome and progression to total hip arthroplasty after hip arthroscopy. Patients with Tönnis Grade 2 or higher osteoarthritis typically have significantly inferior results.
- Chondral Lesion Severity: Extensive or full-thickness chondral damage, particularly on the acetabular side, is associated with less favorable outcomes.
- Labral Condition: While labral repair generally yields better results than debridement, the intrinsic quality of the labrum and the ability to achieve a stable repair are important.
- Surgeon Experience/Volume: Higher volume surgeons and centers are often associated with better outcomes and lower complication rates.
- Capsular Management: Emerging evidence suggests that routine capsular repair or plication, particularly in patients with borderline dysplasia or generalized ligamentous laxity, may improve outcomes and reduce the incidence of post-operative microinstability.
- Patient Selection: Age (younger patients often fare better), activity level, and realistic expectations are important considerations.
Evolving Indications and Techniques
- Peritrochanteric Arthroscopy: Endoscopic gluteal tendon repair, bursectomy, and ITB release are becoming more common, with good short- to mid-term outcomes reported for refractory cases.
- Ligamentum Teres Debridement/Reconstruction: While primary debridement is common, the role of reconstruction remains investigational.
- Biologic Augmentation: The use of platelet-rich plasma (PRP), bone marrow aspirate concentrate (BMAC), or other orthobiologics in conjunction with microfracture or labral repair is an area of ongoing research, with some promising early results but lacking definitive high-level evidence.
- Imaging Advances: Advanced imaging techniques, including 3D CT reconstruction and quantitative MRI, are improving diagnostic accuracy and surgical planning.
Professional Guidelines
- International Society for Hip Arthroscopy (ISHA): Provides consensus statements and recommendations regarding indications, surgical techniques, and rehabilitation protocols for hip arthroscopy. These guidelines emphasize the importance of patient selection, thorough pre-operative assessment, and a structured rehabilitation program.
- American Academy of Orthopaedic Surgeons (AAOS): While not specific guidelines for hip arthroscopy, their broader clinical practice guidelines for hip pain and osteoarthritis inform decisions regarding the timing and appropriateness of hip preservation procedures versus joint replacement.
In conclusion, hip arthroscopy is a sophisticated and effective procedure for addressing a wide range of hip pathologies, most notably FAI and labral tears, in appropriately selected patients. Continued research, particularly on long-term outcomes and the integration of new technologies and biologic treatments, will further refine its role in hip preservation surgery.




Clinical & Radiographic Imaging


