HEREDITARY MOTOR AND SENSORY NEUROPATHIES
Hereditary motor and sensory neuropathies (HMSN) encompass a broad, heterogeneous group of inherited neuropathic disorders affecting the peripheral nervous system. The most prevalent disorder within this classification is Charcot-Marie-Tooth (CMT) disease. Historically, hereditary motor and sensory neuropathies have been classified into seven distinct types based on clinical presentation, inheritance patterns, and neurophysiological findings. Types I, II, and III predominantly manifest in the pediatric population, whereas types IV, V, VI, and VII typically present in adulthood.
Classification of Hereditary Motor Sensory Neuropathies
- Type I: Peroneal atrophy, Charcot-Marie-Tooth disease (hypertrophic form), Roussy-Lévy syndrome (areflexic dystasia) — Autosomal dominant
- Type II: Charcot-Marie-Tooth disease (neuronal form) — Variable inheritance
- Type III: Dejerine-Sottas disease — Autosomal recessive
- Type IV: Refsum disease — Autosomal recessive
- Type V: Neuropathy with spastic paraplegia
- Type VI: Optic atrophy with peroneal muscle atrophy
- Type VII: Retinitis pigmentosa with distal muscle weakness and atrophy
Charcot-Marie-Tooth Disease (Peroneal Muscular Atrophy)
Charcot-Marie-Tooth disease is an inherited, progressive degenerative disorder of the peripheral nervous system that induces profound distal muscle atrophy, weakness, and a marked loss of proprioception. While it is most frequently inherited as an autosomal dominant trait, X-linked recessive and autosomal recessive variants exist. The epidemiological incidence of the various forms of CMT ranges from 20 per 100,000 to 1 per 2,500 individuals.
In the classic autosomal dominant form, muscle atrophy is steadily progressive. Less commonly, the disease may arrest completely or exhibit an intermittent clinical course. Conversely, the autosomal recessive forms are characterized by an early onset (typically within the first or second decade of life) and a much more rapid, aggressive progression.
Clinical Presentation and Diagnosis
Initial clinical complaints usually center around generalized weakness of the foot and an increasingly unsteady gait. Patients frequently present with a constellation of foot problems, including intractable pain under the metatarsal heads, rigid claw toes, rapid foot fatigue, and significant difficulty fitting into standard footwear. Distal loss of proprioception and spinal ataxia are common concomitant findings.
Clinical Pearl: Charcot-Marie-Tooth disease must be at the top of the differential diagnosis in any patient presenting with bilateral claw toes, high arches (cavus), "stork-like" thin legs (due to calf atrophy), poor balance, and a steppage gait.

Clinical presentation of severe cavovarus foot deformity characteristic of Charcot-Marie-Tooth disease, demonstrating profound intrinsic wasting and hindfoot varus.

Fig. 32-18 Cavovarus foot deformity in Charcot-Marie-Tooth disease. A, Clawing of left great toe. B, Fixed varus deformity of left hindfoot. C, Supination and cavus deformity of forefoot.

Further clinical views demonstrating the classic "tripod" weight-bearing mechanism and severe forefoot pronation.
Diagnostic confirmation relies on a combination of meticulous physical examination, detailed family history, and electromyography (EMG). EMG typically reveals an increased amplitude in the duration of response and markedly slow nerve conduction velocities, pathognomonic for the demyelinating forms of the disease.
Advances in molecular biology have revolutionized the diagnostic algorithm for CMT, allowing for precise differentiation between genetic variants. A mutation of the connexin 32 gene is strongly associated with the most common form of X-linked CMT. Furthermore, Type IA CMT (often presenting as hereditary neuropathy with liability to pressure palsies) is directly associated with a duplication or deletion of the peripheral myelin protein 22 gene (PMP22). This specific genetic anomaly is present in approximately 70% of patients with Type IA CMT. Southern blot analysis and targeted genetic sequencing can now definitively confirm these abnormalities, allowing orthopaedic surgeons to provide highly specific prognostic information and tailored treatment recommendations.
Pathoanatomy of the Cavovarus Foot Deformity
Charcot-Marie-Tooth disease is the single most common neuromuscular etiology of cavovarus foot deformity in children and adolescents. The cavovarus foot is a highly complex, multiplanar deformity involving both the forefoot and the hindfoot.
Biomechanics of Muscle Imbalance
The neuropathic cavovarus deformity is driven by a predictable, progressive pattern of intrinsic and extrinsic muscle weakness. The pathogenesis begins with the denervation and subsequent weakness of the intrinsic foot muscles (lumbricals and interossei) and the anterior tibial muscle. Crucially, the antagonist muscles—the posterior tibial and peroneus longus muscles—retain normal strength for a prolonged period. The triceps surae also progressively weakens and may develop secondary contractures.
This specific pattern of muscle imbalance creates a cascade of deforming forces:
1. Plantarflexed First Ray: The strong, unopposed peroneus longus aggressively plantarflexes the first metatarsal.
2. Equinus and Pronation: The forefoot is pulled into equinus relative to the hindfoot. The forefoot becomes rigidly pronated into a valgus position with mild adduction of the metatarsals.
3. Claw Toes: The long toe extensors (extensor digitorum longus and extensor hallucis longus) attempt to recruit and assist the weakened anterior tibial tendon in ankle dorsiflexion. However, because the intrinsics are weak, this recruitment hyperextends the metatarsophalangeal (MTP) joints and flexes the interphalangeal (IP) joints, creating rigid claw toes and further depressing the metatarsal heads.
4. Hindfoot Varus: Initially, the foot remains supple and plantigrade during weight-bearing. However, as the first ray becomes rigidly plantarflexed, it acts as a kickstand. During the stance phase of gait, the rigid plantarflexed first ray forces the hindfoot into a compensatory varus position.
Ultimately, weight-bearing is reduced to a pathological "tripod" mechanism, with the entire body weight borne exclusively on the heel, the first metatarsal head, and the fifth metatarsal head.
Clinical and Radiographic Evaluation
The Coleman Block Test
Clinical evaluation of the cavovarus deformity must determine the flexibility and primary driver of the hindfoot varus. This is definitively assessed using the Coleman Block Test.
Surgical Warning: Never perform a primary hindfoot osteotomy or arthrodesis for a cavovarus foot without first performing a Coleman block test. If the hindfoot varus is entirely driven by a rigid plantarflexed first ray, correcting the forefoot alone will spontaneously correct the hindfoot.
To perform the test, the patient stands with the heel and the lateral border of the foot (metatarsals 2-5) on a 1-inch wooden block, allowing the plantarflexed first metatarsal to drop off the medial edge of the block into free space. If the hindfoot varus corrects to a neutral or valgus alignment, the hindfoot is deemed flexible, and the deformity is primarily driven by the forefoot. If the hindfoot remains in varus, the deformity is fixed, necessitating a concurrent calcaneal osteotomy or arthrodesis.
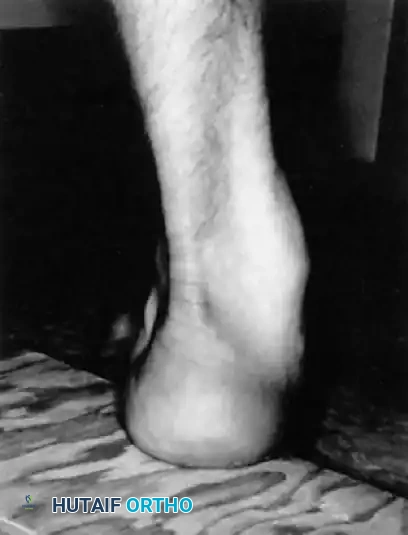
Fig. 32-19 Coleman block test shows flexible hindfoot. The heel and lateral border of the foot are placed on a 1-inch block, allowing the rigidly plantarflexed first ray to drop to the floor. Correction of the heel varus indicates a flexible hindfoot.
Radiographic Assessment
Standard weight-bearing anteroposterior (AP), lateral, and oblique radiographs of the foot and ankle are mandatory. Non-weight-bearing films are virtually useless for assessing the true structural relationships of the cavovarus foot.
* AP View: Documents the degree of forefoot adduction and talonavicular coverage.
* Lateral View: Quantifies the severity of the cavus via Meary's angle (the angle between the longitudinal axis of the talus and the longitudinal axis of the first metatarsal). A normal Meary's angle is 0 degrees; in a cavovarus foot, the angle is increased with the apex directed dorsally.
* Block Test Radiographs: Lateral radiographs taken while the patient performs the Coleman block test can radiographically document the flexibility of the subtalar joint.
Principles of Orthopaedic Treatment
Nonoperative treatment (e.g., stretching, orthotics, custom footwear) is generally unsuccessful at halting the progression of the cavovarus deformity, though AFOs may assist with foot drop. Surgical intervention is frequently required to stabilize the foot, restore a plantigrade weight-bearing surface, and prevent long-term joint degeneration.
Surgical procedures are categorized into three main types:
1. Soft-Tissue Procedures: Plantar fascia release, tendon lengthenings, and tendon transfers.
2. Osteotomies: First metatarsal dorsal closing wedge, midfoot osteotomies, and calcaneal osteotomies (Dwyer or sliding).
3. Joint Stabilizing Procedures: Triple arthrodesis (reserved as a salvage procedure).
Age and Deformity-Based Algorithm
- Children < 8 years (Supple Hindfoot): Respond well to radical plantar releases and appropriate tendon transfers (e.g., posterior tibial tendon transfer to the dorsum).
- Children < 12 years (Rigid Forefoot, Flexible Hindfoot): Require radical plantar-medial release combined with a dorsal closing wedge osteotomy of the first metatarsal.
- Adolescents/Adults (Rigid Hindfoot): Require the above forefoot procedures combined with a calcaneal osteotomy. If the heel is prominent, a Dwyer lateral closing wedge osteotomy is preferred. If not prominent, a lateralizing sliding calcaneal osteotomy is highly effective.
- Severe/Degenerative Deformity: Triple arthrodesis is utilized as a salvage procedure. Wukich and Bowen reported that with aggressive early soft-tissue and osteotomy management, only 14% of CMT patients ultimately require a triple arthrodesis.
Surgical Techniques
Radical Plantar-Medial Release and Dorsal Closing Wedge Osteotomy (Coleman)
This procedure is the cornerstone of correcting the rigid forefoot pronation and cavus in a patient with a flexible hindfoot.
Indications: Rigid plantarflexed first ray, severe cavus, flexible hindfoot (positive Coleman block test).
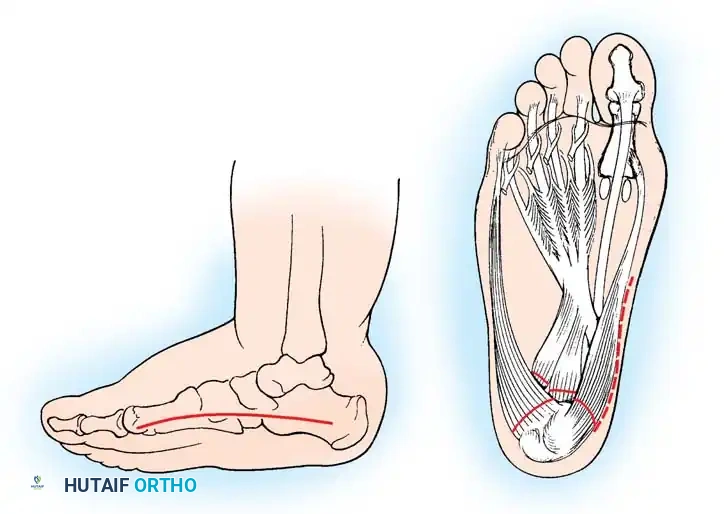
Fig. 32-22 Radical plantar-medial release and dorsal closing wedge osteotomy for cavovarus deformity. A, Incision. B, Release of musculotendinous mass.
Surgical Steps:
1. Incision: Make a generous curved incision over the medial aspect of the foot, extending anteriorly from the medial tuberosity of the calcaneus to the base of the first metatarsal.
2. Superficial Dissection: Identify the origin of the abductor hallucis muscle. Carefully separate it from its bony and soft-tissue attachments proximally and distally, leaving it attached only at its absolute origin and insertion.
3. Neurovascular Protection: Identify the posterior tibial neurovascular bundle as it divides into the medial and lateral plantar branches. Meticulous retraction is required as these structures enter the intrinsic musculature of the foot.
4. Deep Release: Identify the tendinous origin of the abductor hallucis at its attachment on the calcaneus (located between the medial and lateral plantar branches). Sever it to free the origin.
5. Plantar Fascia and Short Flexors: Sever the origins of the plantar aponeurosis and the flexor digitorum brevis from their attachments to the calcaneus. Gently dissect this entire musculotendinous mass distally and extraperiosteally as far as the calcaneocuboid joint.
6. First Metatarsal Osteotomy: If the first metatarsal remains rigidly plantarflexed after the soft-tissue release, proceed to a bony correction. Expose the base of the first metatarsal. Make a dorsally based closing wedge osteotomy immediately distal to the physis (in children) or the tarsometatarsal joint (in adults). Remove sufficient bone to correct the lateral talo-first metatarsal angle (Meary's angle) to 0 degrees.
7. Fixation: Secure the osteotomy with a smooth Steinmann pin or heavy Kirschner wires.
8. Closure: Close the wound in a routine fashion. Apply a well-padded short leg cast with the foot held in the corrected, plantigrade position.
Postoperative Protocol: If there is excessive tension on the medial skin edges during closure, the foot may be casted in slight plantarflexion initially. A cast change is performed at 2 weeks under sedation or in the clinic to bring the foot into a fully corrected position. Pins and casts are typically removed at 6 to 8 weeks, followed by transition to a walking boot and aggressive physical therapy.
Tendon Transfers for Claw Toe Deformity
Flexible claw toe deformities often resolve spontaneously once the midfoot and forefoot cavus is corrected. However, rigid clawing or severe anterior tibial weakness requires dedicated tendon transfers.
The Jones Procedure (Extensor Hallucis Longus Transfer)
Indications: Rigid clawing of the great toe, weakness of ankle dorsiflexion.
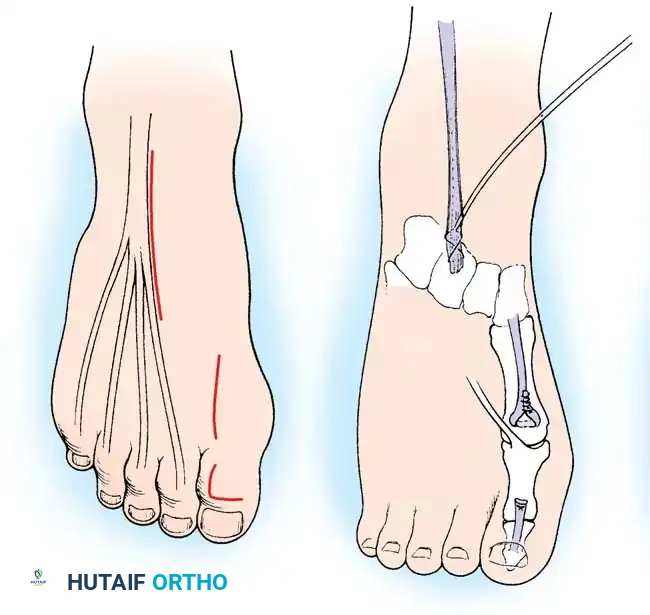
Transfer of the extensor hallucis longus tendon to the first metatarsal neck.
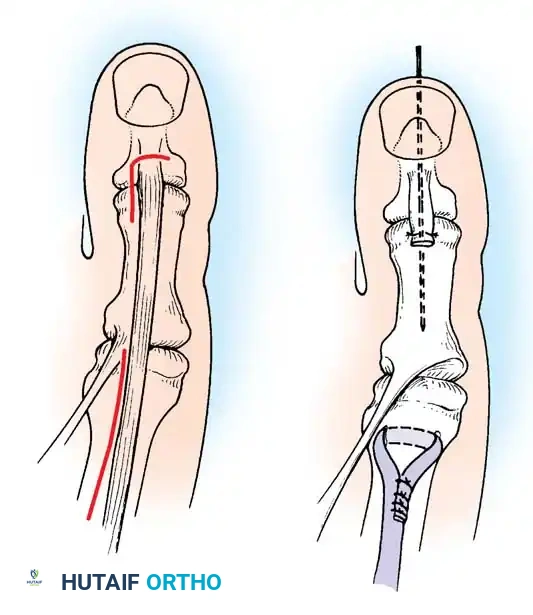
Fig. 32-23 Transfer of extensor hallucis longus tendon for claw toe deformity (Jones procedure). A, Incisions. B, Completed procedure with IP joint fusion.
Surgical Steps:
1. Exposure: Expose the interphalangeal (IP) joint of the great toe through an L-shaped or dorsal longitudinal incision.
2. Tendon Harvest: Isolate the Extensor Hallucis Longus (EHL) tendon. Transect it just proximal to its insertion at the base of the distal phalanx.
3. IP Joint Fusion: To prevent the development of a severe hallux malleus (drop toe) post-transfer, the IP joint must be arthrodesed. Denude the articular cartilage of the IP joint and fix it with a longitudinal K-wire or a headless compression screw.
4. Tendon Routing: Make a second incision over the neck of the first metatarsal. Retrieve the EHL tendon proximally into this wound.
5. Fixation: Drill a transverse hole through the neck of the first metatarsal. Pass the EHL tendon through the bone tunnel and suture it back onto itself under physiological tension with the ankle held in neutral dorsiflexion.
The Hibbs Procedure
For adolescents with severe global weakness of the anterior tibial muscle and clawing of the lesser toes, the Hibbs procedure is indicated. This involves transferring all the long toe extensors (EDL) to the middle cuneiform to act as primary ankle dorsiflexors, combined with fusion of the proximal interphalangeal joints of the lesser toes.
Salvage Reconstruction: Triple Arthrodesis
Because of the progressive nature of CMT, patients with neglected deformities often develop severe, rigid hindfoot varus with early degenerative osteoarthritic changes in the subtalar, talonavicular, and calcaneocuboid joints. In these scenarios, joint-sparing osteotomies will fail, and a Triple Arthrodesis is required as a definitive salvage procedure.
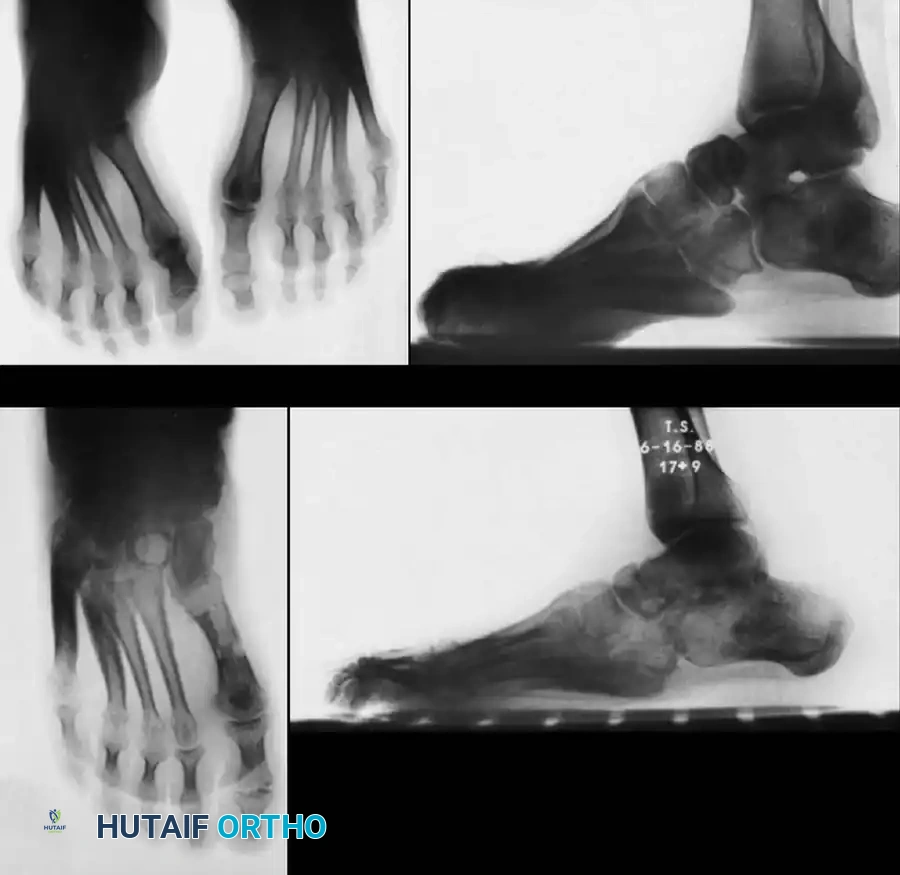
Fig. 32-20 Cavovarus deformity in Charcot-Marie-Tooth disease. A and B, Preoperative weight-bearing radiographs demonstrating severe cavus and hindfoot varus. C and D, Postoperative radiographs after triple arthrodesis, Achilles tendon lengthening, and posterior tibial tendon transfer.
Surgical Principles of Triple Arthrodesis in CMT:
* Deformity Correction: The Hoke arthrodesis (or a modification) is frequently utilized. Appropriate biplanar wedge resections are critical to correct the hindfoot varus and the midfoot component of the cavus deformity.
* Muscle Balancing: Arthrodesis alone is insufficient. Soft-tissue release and muscle balancing (e.g., transferring the strong posterior tibial tendon anteriorly through the interosseous membrane to the dorsum of the foot) are mandatory to prevent recurrence of the deformity and eliminate the need for a postoperative ankle-foot orthosis (AFO).
* Achilles Tendon Lengthening (ATL): McCluskey, Lovell, and Cummings emphasize that ATL should be performed after the forefoot and midfoot are corrected. Performing an ATL too early in the procedure can result in the force used to dorsiflex the forefoot inadvertently dorsiflexing the calcaneus into an unacceptable calcaneus deformity.
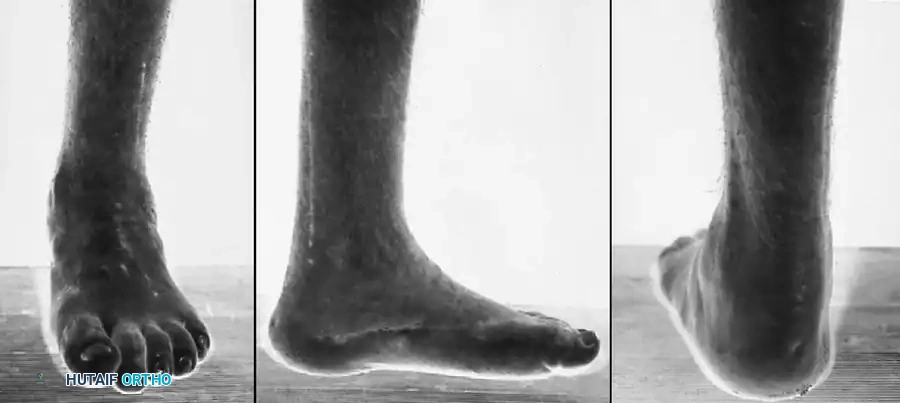
Fig. 32-21 Clinical appearance of the foot in Fig. 32-20 after triple arthrodesis, Achilles tendon lengthening, and posterior tibial tendon transfer. A, Anterior view showing restored alignment. B, Medial correction of the cavus arch. C, Posterior correction of the hindfoot varus to a neutral, stable weight-bearing axis.
Outcomes: When combined with appropriate tendon transfers, triple arthrodesis yields excellent long-term results in severe CMT. Wukich and Bowen reported good or excellent functional outcomes in 88% of their patients treated with triple arthrodesis and concurrent posterior tibial tendon transfer, successfully producing a painless, stable, and plantigrade foot.
