Introduction to Hemipelvectomy
Hemipelvectomy, historically referred to as hindquarter amputation or interilioabdominal amputation, is one of the most radical and technically demanding ablative procedures in orthopedic surgery. It is most frequently performed for the extirpation of primary malignant bone and soft-tissue tumors of the pelvis and proximal thigh that cannot be adequately resected by limb-sparing techniques or standard hip disarticulation.
In contrast to hip disarticulation, all types of hemipelvectomy involve the resection of the pelvic ring and inherently remove the inguinal and iliac lymph node basins. While oncologic control remains the primary indication, other critical indications include life-threatening necrotizing infections, intractable pelvic osteomyelitis, and end-stage arterial insufficiency. Furthermore, as reported by Chan et al., hemipelvectomy may be indicated as a salvage procedure for massive, recalcitrant decubitus ulcers complicated by systemic sepsis in patients with spinal cord injuries.
Surgical Warning: All variations of hemipelvectomy are extremely invasive, mutilating procedures associated with massive fluid shifts and potential for catastrophic hemorrhage. They require rigorous preoperative optimization of the patient’s nutritional and hemodynamic status, extensive preparation for massive blood transfusion, and invasive intraoperative hemodynamic monitoring (e.g., arterial lines, central venous catheters).
Classification of Hemipelvectomy
The surgical approach is dictated by the anatomic location of the pathology, the required oncologic margins, and the availability of soft tissue for closure. The primary classifications include:
- Standard Hemipelvectomy: Employs a posterior or gluteal myocutaneous flap. The bony resection involves disarticulation through the symphysis pubis anteriorly and the sacroiliac (SI) joint posteriorly.
- Extended Hemipelvectomy: Involves a more proximal posterior bony transection that passes directly through the sacrum, often required for tumors invading the SI joint or sacral ala.
- Conservative Hemipelvectomy: A supraacetabular amputation where the bony transection divides the ilium above the acetabulum (typically through the greater sciatic notch), preserving the superior crest of the ilium and minimizing abdominal wall disruption.
- Internal Hemipelvectomy: A limb-sparing resection that achieves proximal and medial margins equivalent to a corresponding amputation but preserves the distal extremity. (Note: This is a distinct limb-salvage topic and is not the focus of the ablative techniques described herein).
Preoperative Planning and Rehabilitation Considerations
The decision to proceed with a hemipelvectomy must be made within a multidisciplinary tumor board setting. Advanced imaging, including MRI of the pelvis and thigh, CT of the chest/abdomen/pelvis, and often CT angiography, is mandatory to delineate tumor extent and vascular involvement.
Psychological and Prosthetic Realities
Appropriate emotional and psychological support is a paramount component of the preoperative and postoperative phases. The loss of a hemipelvis alters sitting balance, bowel and bladder mechanics, and body image profoundly.
Clinical Pearl: While advanced, highly engineered prostheses (such as the Canadian hip disarticulation prosthesis modified for hemipelvectomy) are available, the reality is that very few patients find them functionally useful for daily ambulation due to the massive energy expenditure required and the lack of a stable pelvic suspension point. Most patients ultimately rely on crutches or a wheelchair for primary mobility.
Furthermore, nearly all patients experience significant phantom limb pain in the early postoperative course. Preemptive analgesia, including perioperative gabapentinoids, ketamine infusions, and regional anesthesia catheters (when anatomically feasible), should be integrated into the surgical plan. Flap necrosis and wound sloughs are the most common local complications, necessitating meticulous tissue handling and strategic flap design.
Technique 12-3: Standard Hemipelvectomy (Posterior Flap)
The standard hemipelvectomy utilizes a posterior gluteal flap and is the workhorse procedure for large anterior or medial tumors where the posterior tissues are free of disease.
Positioning and Preparation
- Catheterization: Insert a Foley catheter to decompress the bladder and monitor urine output.
- Positioning: Place the patient in a full lateral decubitus position with the involved side up. Secure the patient meticulously using a beanbag or pegboard system so that the operating table can be safely tilted (airplaned) to facilitate alternating anterior and posterior dissection without compromising sterility.
- Draping: Prepare the skin from the costal margin to the toes. Drape the extremity free to allow for manipulation during the disarticulation phase.
Anterior Dissection and Vascular Control
- Incision: Make an anterior incision extending from 5 cm proximal to the anterior superior iliac spine (ASIS), curving inferiorly and medially to the pubic tubercle.
- Abdominal Wall Release: Deepen the incision through the tensor fascia lata, the external oblique aponeurosis, and the internal oblique and transversalis muscles.
- Pelvic Exposure: Retract the spermatic cord (or round ligament) medially. Expose the iliac fossa via blunt dissection. Carefully elevate the parietal peritoneum off the iliac vessels, permitting the peritoneal sac and viscera to fall medially and inferiorly.
- Vascular Ligation: Ligate the inferior epigastric vessels. Release the rectus abdominis muscle and its sheath from the pubis.
- Major Vessel Transection: Identify the common iliac vessels. Retract the ureter medially to protect it. Double-ligate and divide the common iliac artery and vein.
- Deep Pelvic Dissection: Apply lateral traction on the distal stumps of the iliac artery and vein. Ligate and divide their visceral branches supplying the sacrum, rectum, and bladder. Separate the rectum and bladder from the pelvic side wall, exposing the sacral nerve roots.
- Note: If exposure is severely limited by a massive tumor, the symphysis pubis and sacroiliac joint may be divided early to allow the hemipelvis to "open like a book."
- Packing: Pack the anterior wound with warm, moist laparotomy sponges to achieve hemostasis while transitioning to the posterior approach.
Posterior Dissection and Flap Elevation
- Posterior Incision: Create a posterior skin incision starting from the superior extent of the anterior incision (5 cm above the ASIS). Course it over the anterior aspect of the greater trochanter, parallel the gluteal crease posteriorly around the thigh, and connect it to the inferior end of the anterior incision at the pubis.
- Flap Elevation: Raise the posterior myocutaneous flap by dissecting the gluteal fascia directly off the gluteus maximus. The fascia must be included with the flap to preserve the subdermal plexus. Whenever oncologically safe, include the medial portion of the gluteus maximus with the flap to enhance vascularity and bulk, as recommended by Karakousis and Vezeridis.
- Muscle Detachment: Superiorly, elevate the flap off the iliac crest. Divide the external oblique, sacrospinalis, latissimus dorsi, and quadratus lumborum from their insertions on the iliac crest. Reflect the gluteus maximus from the sacrotuberous ligament, coccyx, and sacrum.
Pelvic Disarticulation
- Neuromuscular Transection: Divide the iliopsoas muscle. Sharply transect the genitofemoral, obturator, and femoral nerves, as well as the lumbosacral nerve trunk at the level of the iliac crest.
- Symphyseal Division: Abduct the hip to place tension on the soft tissues surrounding the symphysis pubis. Pass a large right-angle clamp (e.g., a Mixter or Satinsky) behind the symphysis to protect the bladder and urethra, and divide the fibrocartilaginous disc with a heavy scalpel.
- Sacroiliac Division: Divide the sacral nerve roots, taking extreme care to preserve the nervi erigentes (pelvic splanchnic nerves) to maintain contralateral bowel and bladder function. Reflect the iliacus muscle laterally to expose the anterior SI joint. Divide the anterior SI ligaments and the iliolumbar ligament with a scalpel or osteotome.
- Pelvic Floor Release: Apply considerable distal and lateral traction on the extremity to separate the pelvic side wall from the viscera. Proceeding anterior to posterior under direct tension, divide the urogenital diaphragm, pubococcygeus, ischiococcygeus, iliococcygeus, piriformis, sacrotuberous ligament, and sacrospinous ligament.
- Completion: Move the extremity anteriorly to expose and divide the posterior aspect of the SI joint, completing the amputation.
Closure and Aftertreatment
Place large-bore closed-suction drains in the massive dead space. Suture the gluteal fascia of the posterior flap directly to the fascia of the anterior abdominal wall. Close the subcutaneous tissues and skin meticulously.
* Postoperative Care: Leave drains and the Foley catheter in place for several days until output is minimal. It is critical to keep direct pressure off the posterior flap; the patient should be nursed in a lateral or prone position on a specialized pressure-relieving mattress.
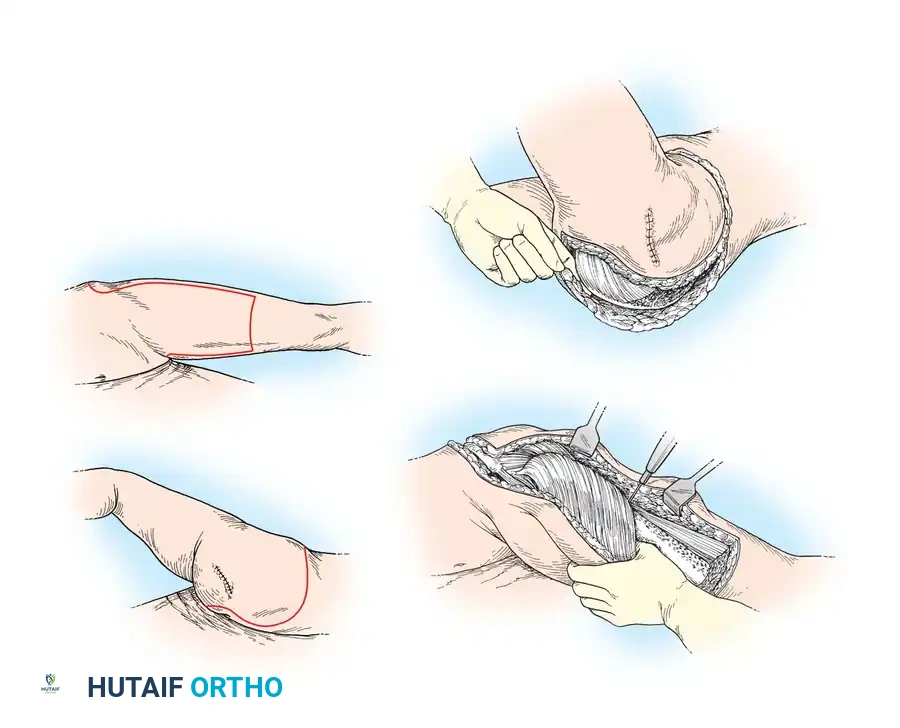
Technique 12-4: Anterior Flap Hemipelvectomy
Anterior flap hemipelvectomy is specifically indicated for massive lesions of the buttock or posterior proximal thigh that preclude the use of a standard posterior flap. In this technique, the large posterior defect is covered by a massive quadriceps myocutaneous flap, which is uniquely maintained by preserving the superficial femoral artery and vein.
Incision and Posterior Dissection
- Preparation: Position the patient in the lateral decubitus position. Mark the skin incisions carefully, ensuring the length and width of the anterior flap will adequately cover the massive posterior defect.
- Incision: Make a superior incision across the iliac crest to the midlateral point, curving around the buttock just lateral to the anus, and extending to the midmedial point of the thigh. Carry the incision distally down the anterior thigh far enough to generate sufficient flap length, then cross the anterior thigh to the midlateral point, and course superiorly to join the starting incision.
- Posterior Release: Perform the posterior dissection first. Preserve a strict skin margin of at least 3 cm from the anal verge to prevent fecal contamination and preserve sphincter function. Detach the gluteus maximus and sacrospinalis from the sacrum. Release the external oblique, sacrospinalis, latissimus dorsi, and quadratus lumborum from the iliac crest.
- Deep Posterior Dissection: Flex the hip to place the gluteal tissues under tension. Detach the remaining origins of the gluteus maximus from the coccyx and sacrotuberous ligament. Bluntly dissect lateral to the rectum, entering the ischiorectal fossa.
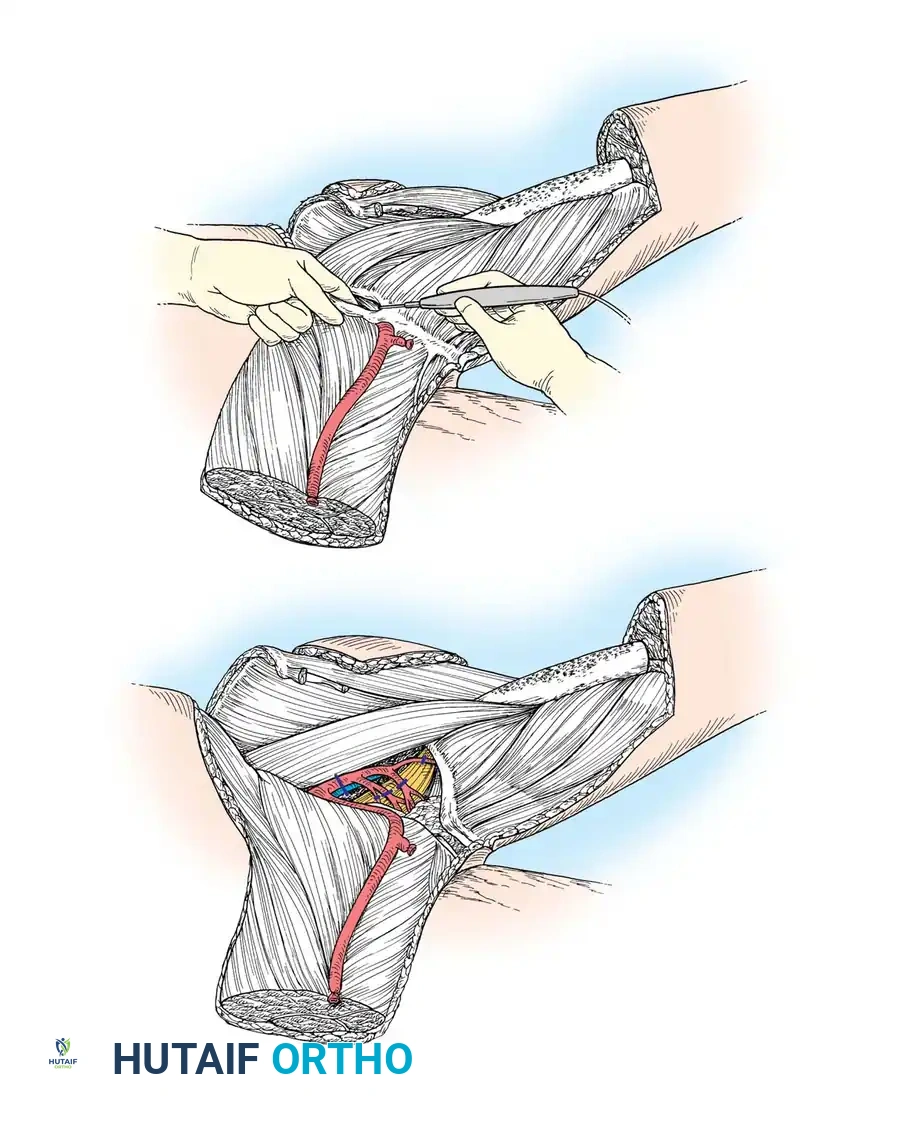
Anterior Dissection and Flap Mobilization
- Flap Creation: Move to the anterior aspect of the patient. Deepen the distal anterior incision (at the junction of the middle and distal thirds of the thigh) directly through the quadriceps muscle down to the femur.
- Lateral Release: Continue the dissection laterally and cephalad toward the ASIS. Sever the vastus lateralis from the linea aspera of the femur. Separate the tensor fascia lata from its investing fascia so that it remains with the tumor specimen.
- Vascular Dissection (The Critical Step): Begin the medial dissection at Hunter’s canal (adductor canal). Identify, ligate, and divide the superficial femoral vessels at this distal level. Trace these vessels superiorly toward the inguinal ligament. Carefully divide and ligate the multiple small muscular branches feeding the adductor compartment, while strictly preserving the main superficial femoral trunk, which will provide axial blood supply to the quadriceps flap.
- Profunda Ligation: Place upward traction on the myocutaneous flap. Detach the vastus medialis and vastus intermedius from the femur. Identify the profunda femoris artery and vein at their origin from the common femoral vessels; ligate and divide them to devascularize the posterior/medial thigh compartments while preserving the superficial femoral vessels.
Pelvic Resection and Inset
- Abdominal Release: Separate the myocutaneous flap from the pelvis by releasing the abdominal musculature from the iliac crest, the sartorius from the ASIS, the rectus femoris from the anterior inferior iliac spine (AIIS), and the rectus abdominis from the pubis.
- Internal Iliac Ligation: Retract the flap medially and dissect along the femoral nerve into the pelvis to expose the iliac vessels. Ligate and divide the internal iliac vessels at their origin from the common iliacs.
- Pelvic Floor and Nerve Division: Divide the symphysis pubis, protecting the bladder. Apply medial traction to the viscera and divide the visceral branches of the internal iliacs. Divide the psoas muscle, the underlying obturator nerve, the lumbosacral trunk, and the sacral nerve roots. Crucially, protect the femoral nerve as it enters the quadriceps flap to maintain muscle tone and prevent profound atrophy.
- Specimen Removal: Elevate the extremity to place traction on the pelvic diaphragm. Divide the urogenital diaphragm, levator ani, and piriformis near their pelvic attachments. Divide the SI joint and iliolumbar ligament, and deliver the specimen.
- Flap Inset: Rotate the massive quadriceps myocutaneous flap posteriorly to cover the defect. Suture the quadriceps muscle to the abdominal wall fascia, sacrospinalis, sacrum, and remnants of the pelvic diaphragm over multiple suction drains.
Clinical Pearl: Skin slough and flap necrosis are significantly less common with the anterior quadriceps flap compared to the classic posterior flap, provided the superficial femoral artery is meticulously preserved and not kinked during posterior rotation.
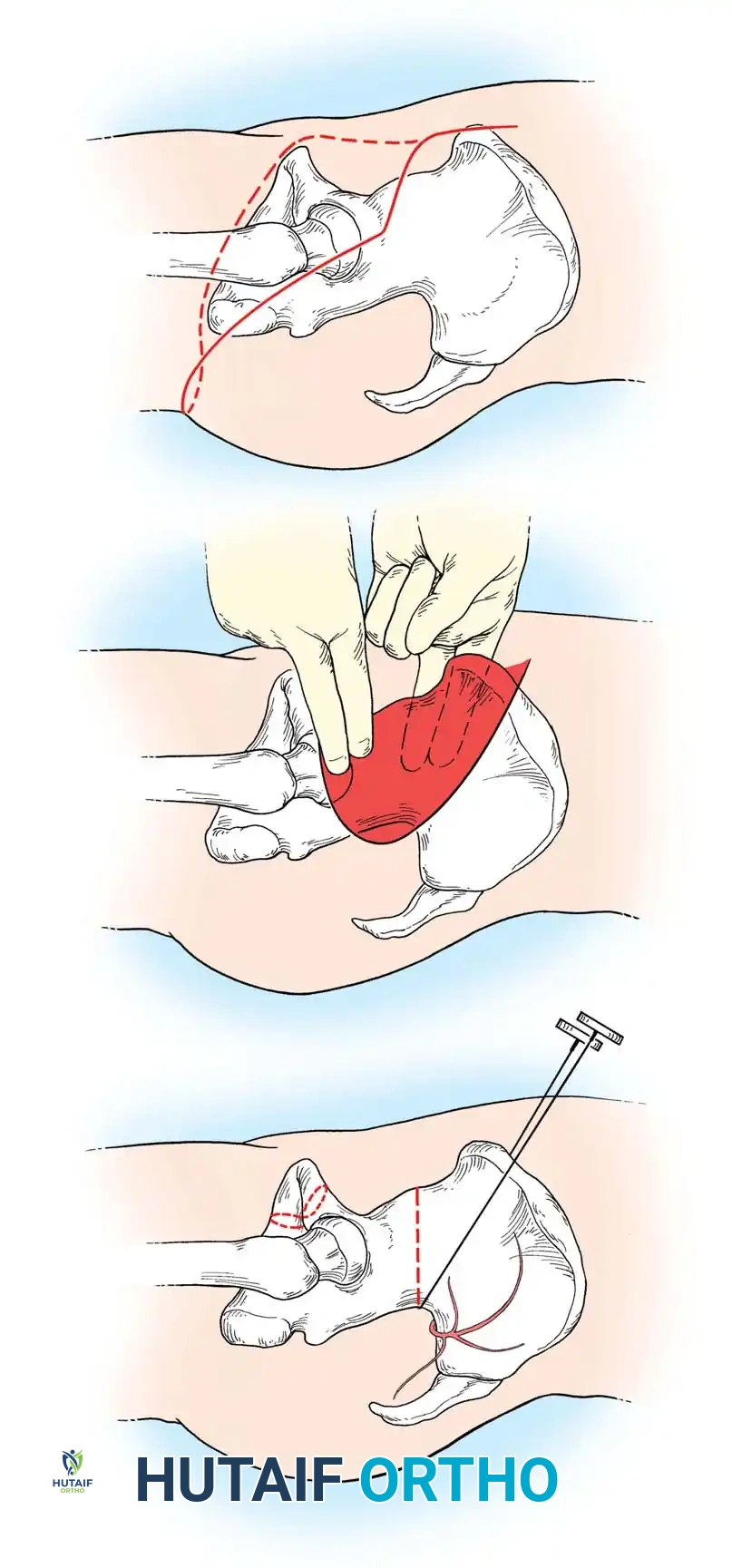
Technique 12-5: Conservative Hemipelvectomy
Conservative hemipelvectomy is a supraacetabular amputation indicated for tumors localized to the proximal thigh and hip joint that cannot be resected via limb-sparing techniques, but importantly, do not require sacroiliac disarticulation to achieve satisfactory proximal oncologic margins. By preserving the iliac wing, abdominal wall contour and core stability are significantly improved.
Incision and Exposure
- Positioning: Place the patient in a lateral decubitus position, secured to allow tilting to either side.
- Racquet Incision: Begin the incision 1 to 2 cm superior to the ASIS. Continue it posteriorly and laterally across the greater trochanter to the gluteal crease, following the crease to the medial thigh. Begin a second incision 5 cm below the starting point of the first, coursing parallel and just superior to the inguinal ligament down to the pubic tubercle. Carry this incision posteriorly across the medial thigh to complete the racquet shape.
Anterior Dissection and Osteotomy
- Retroperitoneal Exposure: Perform the anterior dissection first. Divide the abdominal wall muscles in line with the incision to expose the retroperitoneal space.
- Vascular Control: Bluntly dissect the retroperitoneal space to expose the iliac vessels. Ligate and divide the external iliac artery and vein just distal to the bifurcation of the internal iliacs, preserving pelvic visceral blood flow.
- Symphyseal Division: Divide the symphysis pubis, meticulously protecting the underlying bladder and urethra with a retractor.
- Iliac Osteotomy: The defining step of the conservative hemipelvectomy is the division of the ilium through the greater sciatic notch.
- Bluntly dissect the iliopsoas muscle from the medial wall of the ilium by passing a finger from the ASIS down to the greater sciatic notch.
- Similarly, elevate the gluteal muscles from the lateral aspect of the ilium.
- Pass a Gigli saw through the greater sciatic notch, positioning it just inferior to the origin of the gluteus minimus, and perform a smooth, transverse osteotomy of the ilium.
Specimen Extirpation and Closure
- Soft Tissue Release: With the bone divided, the extremity becomes highly mobile. Position the leg to place the remaining muscle groups under tension. Divide the muscles at appropriate oncologic levels.
- Neurovascular Division: Sharply transect the femoral, obturator, and sciatic nerves. Allow the nerves to retract deep into the soft tissues to minimize symptomatic neuroma formation.
- Pelvic Floor Preservation: Carefully divide the urogenital and pelvic diaphragms at their distal attachments, ensuring the bladder and rectum are protected. Remove the specimen.
- Closure: Achieve meticulous hemostasis. Close the myocutaneous flaps over large-bore suction drains.
Postoperative Protocol
The drains and Foley catheter must remain in place for several days to manage the high volume of serosanguinous exudate typical of large dead-space resections. Strict offloading of the posterior flap is mandatory for the first 5 to 7 days to prevent pressure necrosis. Early mobilization to a chair is encouraged once hemodynamic stability is achieved and flap viability is confirmed. Rehabilitation focuses on core strengthening, wheelchair mobility, and single-leg transfers.
