Introduction and Epidemiology
Hand fractures represent a significant proportion of musculoskeletal trauma presenting to emergency departments and orthopedic clinics. Metacarpal and phalangeal fractures are highly prevalent, comprising approximately 10% of all skeletal fractures, with over 50% of these injuries occurring in work-related settings. The 1998 United States National Hospital Ambulatory Medical Care Survey identified phalangeal (23%) and metacarpal (18%) fractures as the second and third most common hand and forearm fractures, secondary only to distal radius fractures. Depending on the specific epidemiological survey methods utilized, hand fractures constitute anywhere from 1.5% to 28% of all emergency department visits.

Border digits are most frequently involved in these injury patterns. The small finger ray is the most commonly injured axis, constituting up to 37% of total hand fractures. While historical studies present conflicting data regarding exact anatomical distribution, a landmark 1996 study published in Injury analyzing a series of 1,358 hand fractures demonstrated the following distribution: 57.4% proximal phalanx, 30.4% middle phalanx, and 12.2% metacarpal fractures.

Demographic analysis reveals a male-to-female ratio ranging from 1.8 to 1 up to 5.4 to 1. Higher male predominance is observed in age cohorts associated with the greatest incidence of specific trauma mechanisms. These include sports-related injuries peaking in the early third decade, workplace and industrial injuries peaking in the fifth decade, and low-energy falls becoming the predominant mechanism in the seventh decade and beyond.
Surgical Anatomy and Biomechanics
A profound understanding of osseous anatomy and the deforming forces exerted by intrinsic and extrinsic musculature is prerequisite for achieving anatomic reduction and stable fixation, whether utilizing closed reduction and internal fixation (CRIF) or open reduction and internal fixation (ORIF).
Metacarpal Osteology and Biomechanics
The metacarpals are anatomically bowed, presenting a concave surface on the palmar aspect. Together with the carpus, they form the critical longitudinal and transverse arches of the hand, which are essential for grip strength and dexterous function. The carpometacarpal (CMC) articulations vary significantly in their mobility. The index and long finger CMC joints are highly rigid, providing a stable central pillar for pinch and grasp. Conversely, the ring and small finger CMC articulations are highly flexible, allowing for the cupping motion of the hand.

Deforming forces in metacarpal fractures are primarily driven by the intrinsic musculature. Three palmar and four dorsal interosseous muscles arise from the metacarpal shafts and insert distally to flex the metacarpophalangeal (MCP) joints. In the setting of a metacarpal shaft fracture, these muscles create a robust deforming force that typically flexes the distal fragment, resulting in characteristic apex dorsal angulation.

Phalangeal Osteology and Biomechanics
Phalangeal fractures exhibit predictable deformity patterns based on their relationship to tendinous insertions. Proximal phalanx fractures classically angulate into extension, creating an apex volar deformity. This occurs because the proximal fragment is flexed by the interossei inserting at the base, while the distal fragment is extended by the central slip of the extensor mechanism inserting at the base of the middle phalanx.

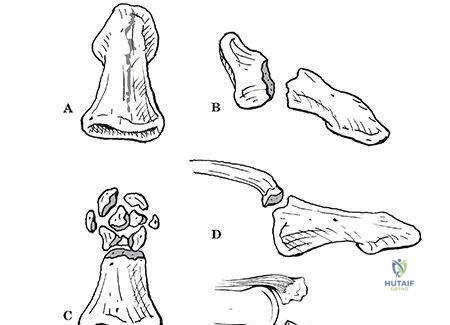
Middle phalanx fractures present with unpredictable angulation depending on the fracture line's relationship to the flexor digitorum superficialis (FDS) insertion. Fractures proximal to the FDS insertion typically exhibit apex dorsal angulation (proximal fragment extended by the central slip, distal fragment flexed by FDS). Fractures distal to the FDS insertion exhibit apex volar angulation (proximal fragment flexed by FDS, distal fragment extended by the terminal extensor tendon). Distal phalanx fractures are frequently the result of crush injuries, presenting as comminuted tuft fractures with associated nail bed lacerations.

Indications and Contraindications
The decision to proceed with operative intervention—and specifically the choice between CRIF and ORIF—relies on fracture geometry, inherent stability, soft tissue envelope integrity, and patient-specific functional demands.

While many hand fractures can be managed non-operatively with closed reduction and immobilization in an intrinsic-plus position, fractures that are irreducible, inherently unstable, or involve significant articular displacement necessitate surgical fixation. CRIF is generally preferred for extra-articular fractures where closed reduction can be achieved and maintained with percutaneous Kirschner wires (K-wires), thereby preserving the soft tissue envelope and periosteal blood supply. ORIF is indicated when closed reduction is unattainable, in complex intra-articular fractures requiring absolute stability, or when early active motion is critical to prevent tendon adhesions.

| Clinical Scenario | Operative Indications | Non Operative Indications |
|---|---|---|
| Metacarpal Shaft Fractures | Rotational malalignment (any degree); Shortening > 5mm; Apex dorsal angulation > 10° (index/long) or > 30-40° (ring/small); Multiple adjacent fractures. | Stable, non-displaced fractures; Acceptable angulation without rotational deformity; Patient non-compliance or high surgical risk. |
| Metacarpal Neck Fractures | Rotational malalignment; Pseudoclawing; Angulation > 15° (index/long) or > 50-70° (small finger "Boxer's"). | Angulation within acceptable limits based on digit (e.g., up to 70° in small finger if no rotation/pseudoclawing). |
| Proximal Phalanx Fractures | Any rotational deformity; Angulation > 10° apex volar; Shortening > 2mm; Intra-articular displacement > 1mm. | Non-displaced fractures; Stable transverse fractures reducible and maintainable in intrinsic-plus splint. |
| Middle Phalanx Fractures | Intra-articular displacement > 1mm (e.g., pilon fractures); Unstable oblique/spiral fractures; Rotational malalignment. | Extra-articular, non-displaced fractures; Stable transverse fractures. |
| Open Fractures | All requiring irrigation, debridement, and skeletal stabilization. | N/A (Operative management required). |
Pre Operative Planning and Patient Positioning
Clinical Evaluation and Mechanism of Injury
A high degree of variation in the mechanism of injury accounts for the broad spectrum of skeletal trauma sustained by the hand. A meticulous history is essential as it directly influences treatment algorithms. Key historical elements include the patient’s age, hand dominance, occupation, systemic illnesses, and financial or workers’ compensation considerations.

The exact mechanism of injury dictates the expected fracture pattern and associated soft tissue trauma:
* Axial Load: Frequently sustained during ball sports or sudden reaches. Patterns include shearing articular fractures or metaphyseal compression fractures. Axial loading along the upper extremity mandates a high index of suspicion for associated injuries to the carpus, forearm, elbow, and shoulder girdle.
* Crush: Industrial settings or environments with heavy objects lead to crushing mechanisms that combine bending, shearing, and torsion. Distal phalanx fractures usually result from crush injuries and present as comminuted tuft fractures.
* Bending: Diaphyseal fractures and joint dislocations usually require a bending component, occurring during sports or when the hand is trapped.
* Torsion: Individual digits caught in clothing or machinery sustain torsional forces, resulting in spiral fractures or complex dislocation patterns.
* Avulsion: Ring avulsion injuries result in severe soft tissue compromise ranging from circumferential laceration to complete amputation.
For open fractures, the time of injury, exposure to specific contamination (e.g., barnyard, brackish water, human/animal bite), and pre-hospital treatment provided (cleansing, tourniquet application) must be documented.

Physical Examination and Imaging
Physical examination must assess the digital cascade. Any overlap or scissoring of the digits during active flexion indicates a rotational deformity, which is poorly tolerated and constitutes an absolute indication for intervention. True posteroanterior (PA), true lateral, and oblique radiographs of the individual digit or hand are mandatory. The lateral view must isolate the injured digit to accurately assess apex volar or dorsal angulation without superimposition of adjacent rays.

Patient Positioning
The patient is typically positioned supine with the operative extremity extended on a radiolucent hand table. A well-padded upper arm tourniquet is applied. Regional anesthesia (axillary or supraclavicular brachial plexus block) is highly efficacious, providing excellent intraoperative anesthesia and postoperative analgesia. Wide-awake local anesthesia no tourniquet (WALANT) is increasingly utilized for both CRIF and ORIF, allowing for intraoperative assessment of active tendon gliding and fracture stability. Fluoroscopy is positioned either parallel or perpendicular to the hand table, ensuring unimpeded access for orthogonal imaging.
Detailed Surgical Approach and Technique
Closed Reduction and Internal Fixation Techniques
CRIF is advantageous for minimizing soft tissue stripping, thereby reducing postoperative adhesions and stiffness. It is primarily indicated for extra-articular transverse, short oblique, or spiral fractures that can be anatomically reduced closed.

Metacarpal Intramedullary Pinning (Bouquet Technique):
For metacarpal neck and shaft fractures, antegrade intramedullary pinning provides excellent stability. A small incision is made at the metacarpal base. The cortex is breached with an awl or drill. Pre-bent, blunt-tipped K-wires (typically 0.8mm or 1.0mm) are advanced antegrade through the medullary canal. The fracture is reduced via the Jahss maneuver (flexing the MCP and PIP joints to 90 degrees and applying dorsal directed pressure through the proximal phalanx). The wires are then advanced across the fracture site into the metacarpal head, diverging to provide subchondral support.

Phalangeal Crossed Pinning:
For proximal and middle phalanx fractures, crossed K-wire fixation is standard. Following closed reduction, a 0.035-inch or 0.045-inch K-wire is driven retrograde from the condyle across the fracture site into the contralateral proximal cortex. A second wire is placed from the opposite condyle, ensuring the wires cross proximal to the fracture line to avoid distraction. Care must be taken to avoid tethering the lateral bands of the extensor mechanism.


Open Reduction and Internal Fixation Techniques
ORIF is mandatory when closed reduction fails, for multi-fragmentary diaphyseal fractures, or for displaced intra-articular fractures requiring absolute stability to permit early range of motion.

Dorsal Approach to the Metacarpals:
A longitudinal dorsal incision is made over the affected metacarpal or between adjacent metacarpals if multiple are involved. The extensor tendons are retracted laterally. The dorsal periosteum is incised and elevated minimally to expose the fracture.

For long oblique or spiral fractures, lag screw fixation alone may be sufficient if the fracture length is at least twice the bone diameter. The glide hole is drilled in the near cortex, the thread hole in the far cortex, and the screw is inserted to provide interfragmentary compression.

For transverse or comminuted fractures, a low-profile dorsal plate is utilized. The plate functions in a neutralization or compression mode. At least two (preferably three) bicortical screws are required proximal and distal to the fracture. Meticulous hemostasis and low-profile hardware are critical to prevent postoperative extensor tendon irritation.

Midaxial Approach to the Phalanges:
To avoid the dorsal extensor apparatus, a midaxial approach is frequently employed for phalangeal ORIF. The incision connects the apices of the flexion creases on the non-working border of the digit (ulnar border for index/long, radial border for ring/small). The neurovascular bundle is identified and retracted volarly. The transverse retinacular ligament is incised, exposing the periosteum.
Fixation options include mini-fragment plates (1.2mm to 1.5mm systems) placed laterally, which interfere less with extensor tendon gliding compared to dorsal plates. Alternatively, intra-articular fractures (e.g., unicondylar or bicondylar fractures) are anatomically reduced with reduction forceps and stabilized with miniature lag screws or headless compression screws buried beneath the articular cartilage.
Complications and Management
Complications following surgical management of hand fractures can severely compromise digital function. The delicate interplay between the osseous structures and the surrounding soft tissue envelope means that even minor technical errors can lead to profound morbidity.

Stiffness is the most ubiquitous complication, often resulting from prolonged immobilization, excessive soft tissue dissection during ORIF, or tethering of the extensor mechanism by prominent hardware. Nonunion is relatively rare in the hand due to excellent vascularity, but malunion—particularly rotational malunion—is a frequent consequence of inadequate intraoperative assessment.

Infection rates are elevated in open fractures, crush injuries, and when percutaneous K-wires are left protruding through the skin. Pin tract infections typically resolve with oral antibiotics and pin removal, whereas deep infections involving internal hardware necessitate formal irrigation, debridement, and potential hardware explantation.

| Complication | Estimated Incidence | Etiology and Risk Factors | Salvage and Management Strategies |
|---|---|---|---|
| Joint Stiffness | 15% - 50% | Prolonged immobilization (>3 weeks); Extensive periosteal stripping; Extensor tendon adhesions over dorsal plates. | Aggressive hand therapy; Dynamic splinting; Surgical tenolysis and capsulotomy if refractory after 6 months. |
| Rotational Malunion | 5% - 10% | Failure to assess digital cascade intraoperatively; Inadequate reduction prior to fixation. | Corrective osteotomy (metacarpal base or phalangeal shaft) depending on the apex of deformity. |
| Pin Tract Infection | 10% - 15% | Exposed K-wires; Poor local hygiene; Prolonged retention (>4-6 weeks). | Oral antibiotics (first-generation cephalosporin); Early pin removal if clinical union is achieved. |
| Hardware Failure | < 5% | Premature load bearing; Inadequate construct rigidity (e.g., single K-wire for rotational stability). | Revision internal fixation with robust plating; Bone grafting if associated with delayed union. |
| Nonunion | 1% - 2% | Severe bone loss (crush injuries); Infection; Inadequate stabilization. | Debridement of non-viable bone; Rigid ORIF with autologous cancellous bone grafting. |
Post Operative Rehabilitation Protocols
The ultimate success of both CRIF and ORIF relies heavily on the postoperative rehabilitation protocol. The primary goal is to achieve stable osseous union while preventing tendon adhesions and joint contractures.

Immediately postoperatively, the hand is immobilized in a bulky dressing with a plaster splint. The wrist is positioned in 20-30 degrees of extension, the MCP joints in 70-90 degrees of flexion, and the interphalangeal (IP) joints in full extension. This "intrinsic-plus" or "safe" position maintains the collateral ligaments of the MCP joints at their maximal length, preventing extension contractures, while preventing flexion contractures at the IP joints.
For fractures treated with rigid ORIF, early active motion (EAM) protocols are initiated within 3 to 5 days postoperatively. Hand therapists guide patients through differential tendon gliding exercises to prevent adherence of the FDS and FDP tendons.
For fractures treated with CRIF, the timing of motion depends on construct stability. If percutaneous pins cross the joint (e.g., trans-articular pinning for severe intra-articular fractures), the joint must remain immobilized until pin removal at 3 to 4 weeks. If the pins are extra-articular and the construct is stable, gentle active range of motion can be initiated, though care must be taken to avoid pin migration or breakage. Edema control through compressive wrapping and elevation is critical in all postoperative phases to facilitate venous return and minimize fibrotic induration.
Summary of Key Literature and Guidelines
The academic debate between CRIF and ORIF for hand fractures centers on balancing anatomic restoration against soft tissue morbidity. Evidence-based guidelines suggest that while ORIF provides superior radiographic alignment and allows for earlier mobilization, it carries a higher risk of tenosynovitis, hardware irritation, and delayed stiffness requiring tenolysis.

Recent comparative studies demonstrate that functional outcomes (measured by Total Active Motion and grip strength) at one year are largely equivalent between CRIF and ORIF for closed, extra-articular metacarpal and proximal phalanx fractures, provided that acceptable reduction parameters are maintained. However, for unstable intra-articular fractures, multiple contiguous fractures, and fractures with significant soft tissue compromise, the literature strongly supports rigid ORIF to restore joint congruity and permit the early active motion necessary for optimal functional recovery. Surgeon familiarity, fracture morphometry, and patient compliance remain the ultimate determinants in selecting the most appropriate surgical intervention.
Clinical & Radiographic Imaging
