📖
Clinical Article
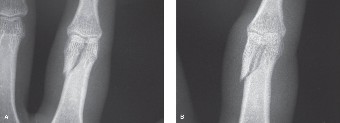
CASE 1 A 28-year-old, right-hand-dominant male caught big air going off a jump while snowboarding for the first time. He landed awkwardly on his non-dominant left hand and immediately developed pain.
Radiographs were obtained at the slope side indicating multiple fractures in the hand (Fig. 4–1A and B).
 🔍 Click to enlarge
🔍 Click to enlarge
Figure 4–1 A–B
He was then splinted and presented to your office on the fourth day after injury.
The most appropriate management at this time for this injury would be:
- Short-arm splint for 6 weeks
- Short-arm cast in intrinsic plus position for 6 weeks
- Long-arm cast in intrinsic plus position for 6 weeks
- Open reduction, internal fixation of all fractures
Discussion
The correct answer is (D). This patient has suffered multiple displaced metacarpal
fractures in contiguous digits. The most appropriate treatment would be an open reduction and internal fixation in order to give the patient an earlier, rehabilitative start.
Identify sequela from this type of injury?** CASE 11 **A 26-year-old female was traveling with her fiancé. At a rest stop, as she got out of the car, he accidentally shut the car door on her left ring finger. There was immediate swelling and bleeding, and after application of first aid, the finger remained swollen and the patient is now here to see you. Radiographs do not show any obvious bony abnormality.
Pinpoint complications of open reduction and internal fixation of these fractures?** CASE 13 **[A 56-year-old homemaker fell down the steps of her basement injuring her left ring finger. She was seen at an outside facility with significant deformity of the ring finger. There were no open wounds. There was severe pain and limited motion. Radiographs are shown in ](file:///C:/Users/DELL/Desktop/hip/board/Chapter%204.%20The%20Hand_Converted.html#bookmark12)[Figures ](file:///C:/Users/DELL/Desktop/hip/board/Chapter%204.%20The%20Hand_Converted.html#bookmark12)4–11A [and ](#bookmark12)B.

_**Figure 4–11 A–B**_
Select surgical approaches for open reduction and internal fixation? Treat these injuries?** CASE 15 **A 54-year-old female comes to your office with a chief complaint of a painful left palm. When further questioned, she mentioned that she has difficulty moving her
finger first thing in the morning and occasionally finds that the finger catches, and she has difficulty opening the palm. Review of systems is negative and the patient reports that she is in otherwise good health. This has been going on the past 6 to 8 weeks.
Perform Nonoperative management in trigger finger? Select invasive treatment options?** CASE 16 **A 61-year-old, diabetic male presents with difficulty moving his dominant right index and middle fingers. He has noticed swelling and difficulty bending both fingers over the last 3 months. Occasionally when he wakes up in the morning, he finds that his fingers are stuck in the bent position. Running warm water over his fingers has helped them to open gradually.
Identify the clinical presentation of trigger finger in diabetics? Pinpoint various treatment options?** CASE 17 **During the course of examination of finger injuries in the emergency room, it is important to be facile with the placement of local anesthetic. This local anesthetic may be administered in the form of flexor sheath block, a web space block, or a digital nerve block which is administered at the level of the metacarpal neck often referred to as the metacarpal block.
Pinpoint postoperative treatment options?** CASE 19 **[A 64-year-old, right-hand-dominant, Caucasian female presents to your office with several months of pain in the right hand. More specifically, she has noticed the pain is worse on doing pinching activities and when trying to do needlepoint and crochet. In gripping these needles, she finds her index finger to be maximally painful as does the rest of the hand. When questioned closely, it appears that the index finger is the most painful. Radiographs are shown in ](file:///C:/Users/DELL/Desktop/hip/board/Chapter%204.%20The%20Hand_Converted.html#bookmark16)[Figure ](file:///C:/Users/DELL/Desktop/hip/board/Chapter%204.%20The%20Hand_Converted.html#bookmark16)4–14A [and ](#bookmark16)B.


_**Figure 4–14 A–B**_
Understand the difference in management between dorsal and volar wrist ganglia? Understand the presentation and management of mucous cysts?** CASE 24 **A 34-year-old man presents to the emergency department with pain in his left small finger. He reports that he was cutting meat when his knife slipped and punctured the volar surface of his proximal phalanx. It did not bleed, and he did not seek further medical treatment. He presents with pain in the finger. A diagnosis of flexor tenosynovitis is suspected.
Describe the natural course of untreated flexor tenosynovitis?** CASE 25 **A 42-year-old man presents to the hospital with pain and swelling of the dorsum of his hand. He reports blunt trauma against a metal shelf, but does not remember a break in the skin. There is a blister of the skin. He reports erythema started approximately 6 hours ago of the hand but it now extends to the wrist. He is febrile to 102 degrees, heart rate is 110, and blood pressure is 92/38. He has significant pain to palpation and induration of the dorsum of the hand.
Identity the bacteria that cause necrotizing fasciitis? Select the expected laboratory values?** CASE 26 **A 32-year-old, male patient reports 4 days ago he was fishing in the wilderness when he punctured his long finger with a fishing hook. Over the past 3 days during his trek back, he reports long finger pain with passive extension, fusiform swelling, and pain along the flexor sheath. Flexor tenosynovitis is suspected. He also reports worsening pain in the hand.
Describe the correct management of midpalmar abscesses?** CASE 27 **A 23-year-old man presents to your office with pain of his fingertip over the past day. He does admit to biting his nails and cuticles, particularly because he is stressed over his upcoming dentistry examinations. He has slight swelling and redness over the ulnar eponychial fold of his index finger. He has tenderness to palpation, but no fluctuance is noted.
the region of his eponychial fold. He reports a metal splinter at that site which he removed 2 weeks ago. He reports that the mass grew quickly and often bleeds.
the+region+of+his+eponychial+fold+He+reports+a+metal+splinter+at+that+site+which+he+removed+2+weeks+ago+He+reports+that+the+mass+grew+quickly+and+often+bleeds++
+What+is+the+most+likely+diagnosis" rel="noopener noreferrer" style="color: #1a5276; font-weight: 600; text-decoration: none; font-size: 0.85rem;" target="_blank">[View Source / PubMed]
Pinpoint the contraindication for wrist centralization in radial hypoplasia?** CASE 30 **An 11-month-old patient is brought to you by his parents for “two thumbs on one hand.” Examination of the hand is significant for diverging, converging thumb duplication on the right. He has a duplication of the proximal and distal phalanges. On palpation, there is a singular thumb metacarpal.
Pinpoint the most common types of thumb duplication? Surgically manage thumb duplication?** CASE 31 **A 17-year-old patient presents for evaluation. He reports that after racing his motocross bike for approximately 20 minutes, he reports pain, weakness of grip, forearm swelling and numbness and tingling of all five digits. On physical examination, he has normal sensation, normal strength of all major muscle groups. It resolves with rest.
Pinpoint+the+most+common+types+of+thumb+duplication+Surgically+manage+thumb+duplication+CASE+31+A+17yearold+patient+presents+for+evaluation+He+reports+that+after+racing+his+motocross+bike+for+approximately+20+minutes+he+reports+pain+weakness+of+grip+forearm+swelling+and+numbness+and+tingling+of+all+five+digits+On+physical+examination+he+has+normal+sensation+normal+strength+of+all+major+muscle+groups+It+resolves+with+rest++
+What+is+the+most+likely+diagnosis" rel="noopener noreferrer" style="color: #1a5276; font-weight: 600; text-decoration: none; font-size: 0.85rem;" target="_blank">[View Source / PubMed]
Describe the anatomy of the hand compartments and how to release each of them? Manage compartment syndrome after release?** CASE 32 **A 34-year-old, right-hand-dominant man presents with a pinpoint injury to his left index finger. He reports that he was cleaning the nozzle of his paint gun when he accidentally pulled the trigger of the gun. Inspection of the digit reveals a pinpoint skin break at the distal phalanx. He receives tetanus prophylaxis and IV antibiotics in the emergency department.
[He has an abnormal cascade and undergoes wound exploration. He is noted to have a laceration of the FDP tendon in zone 2. He undergoes repair of both tendons with a four-strand repair and epitendinous suture. He presents 3 days after injury for wound check (](file:///C:/Users/DELL/Desktop/hip/board/Chapter%204.%20The%20Hand_Converted.html#bookmark20)[Fig. ](#bookmark20)4–18).

_**Figure 4–18**_
He+has+an+abnormal+cascade+and+undergoes+wound+exploration+He+is+noted+to+have+a+laceration+of+the+FDP+tendon+in+zone+2+He+undergoes+repair+of+both+tendons+with+a+fourstrand+repair+and+epitendinous+suture+He+presents+3+days+after+injury+for+wound+check+fileCUsersDELLDesktophipboardChapter20420The20Hand_Convertedhtmlbookmark20Fig+bookmark20418++
Illustration+29+for+Orthopedic+Hand+Cases+A+Patients+Journey+Is+a+Year+Old+a+Factormediaupload6925db2c3a184cfb8cb47762a4842ab0jpg++
++
_Figure+418_++
+What+is+the+most+appropriate+splint+for+him+postoperatively" rel="noopener noreferrer" style="color: #1a5276; font-weight: 600; text-decoration: none; font-size: 0.85rem;" target="_blank">[View Source / PubMed]
Identify tendon rupture and its treatment?** CASE 35 **A 28-year-old woman presents after flexor tendon repair in zone 2. Despite an aggressive therapy protocol, she has not achieved sufficient active motion. The tendon is intact on palpation.
Pinpoint th challenges that affect outcome in replant failure? Identify the signs of venous congestion?
Describe the complications of leeching?** CASE 38 **The patient is a 5-year-old boy who is referred into the emergency department with an amputation of his dominant right thumb at the level of the MP joint, sustained during a motor vehicle collision in which a sharp piece of metal lacerated and amputated his thumb. He has no other injuries and is hemodynamically stable. On examination, the patient has a sharp amputation of his thumb through the MP joint, and plain films demonstrate no fractures with preservation of the metacarpal head and proximal phalangeal base.
Describe the various treatment options after failed implantation?** CASE 39 **[The patient is a 68-year-old, right-handed male who presents to the emergency department following a tablesaw injury to his nondominant left index finger (](file:///C:/Users/DELL/Desktop/hip/board/Chapter%204.%20The%20Hand_Converted.html#bookmark23)[Fig. 4–21A ](file:///C:/Users/DELL/Desktop/hip/board/Chapter%204.%20The%20Hand_Converted.html#bookmark23)[and ](file:///C:/Users/DELL/Desktop/hip/board/Chapter%204.%20The%20Hand_Converted.html#bookmark23)[B](file:///C:/Users/DELL/Desktop/hip/board/Chapter%204.%20The%20Hand_Converted.html#bookmark23)[). The patient states that he was working at home after having “a few](#bookmark23)” beers, when his hand slipped and his nondominant index finger was drawn into the blade of the saw. On examination, he has sustained an amputation to the index finger at the mid-shaft of the proximal phalanx, with a stellate, multilevel soft tissue injury to the index finger base. Radiographs demonstrate a comminuted fracture of the proximal phalanx with intra-articular involvement and a fracture of the metacarpal head. The amputated index finger was irretrievable and not brought to the hospital.

_**Figure 4–21 A–B**_
Identify the functional outcomes of replantation?** CASE 40 **The patient is a 48-year-old, diabetic woman who presents with a 4 months history of numbness and paresthesias of bilateral thumbs, index, and middle fingers. She has had no prior workup for this problem. She reports that her symptoms have been progressive, and that they wake her up from sleep two or three times per week. On physical examination, the patient has grossly normal sensibility in all fingers, and has 5/5 strength to palmar abduction in bilateral thumbs.
Initially manage carpal tunnel syndrome?** CASE 41 **The patient is a 29-year-old, right-hand-dominant G1 P0 woman, currently 7 months pregnant, who presents with edematous hands and numbness in her thumbs bilaterally. She reports that her symptoms are worst at night and wake her up from sleep. The patient states that she did not have similar symptoms prior to pregnancy. On examination, she has a positive Durkan test but no weakness or thenar atrophy. She is diagnosed with carpal tunnel syndrome of pregnancy.
Describe the incidence of pregnancy-induced carpal tunnel syndrome?** CASE 42 **The patient is a 65-year-old, diabetic, male carpenter who presents with bilateral carpal tunnel syndrome. His primary symptoms are paresthesias in the median nerve distribution, although he also complains of clumsiness of his hands. On examination, he has weakness to palmar abduction in his thumbs bilaterally with a positive Durkan test. EMG demonstrates moderate bilateral carpal tunnel syndrome. After patient education and counseling, the patient is prepared to undergo carpal tunnel release.
Describe+the+incidence+of+pregnancyinduced+carpal+tunnel+syndrome+CASE+42+The+patient+is+a+65yearold+diabetic+male+carpenter+who+presents+with+bilateral+carpal+tunnel+syndrome+His+primary+symptoms+are+paresthesias+in+the+median+nerve+distribution+although+he+also+complains+of+clumsiness+of+his+hands+On+examination+he+has+weakness+to+palmar+abduction+in+his+thumbs+bilaterally+with+a+positive+Durkan+test+EMG+demonstrates+moderate+bilateral+carpal+tunnel+syndrome+After+patient+education+and+counseling+the+patient+is+prepared+to+undergo+carpal+tunnel+release++
+Which+of+the+following+is+a+benefit+of+endoscopic+carpal+tunnel+release+compared+to+open+release" rel="noopener noreferrer" style="color: #1a5276; font-weight: 600; text-decoration: none; font-size: 0.85rem;" target="_blank">[View Source / PubMed]
Identify the structures at risk during the release of the transverse carpal ligament? Identify the risk factors for carpal tunnel syndrome?** CASE 43 **The patient is a 52-year-old, right-hand-dominant male with a history of a nondisplaced right distal radius fracture treated with a short-arm cast for 6 weeks who presents with wrist pain and weakness. His fracture occurred 2 months prior to this presentation, and he initially did well and fully regained range of motion in his wrist and hand. Over the past 3 to 4 weeks, the patient has developed thumb and radial-sided wrist pain. On examination, the patient has crepitation with wrist flexion and wrist extension and has weakness with thumb extension at the MP joint and no appreciable extension at the IP joint.
Treat EPL rupture?** CASE 44 **The patient is a 31-year-old woman who sustained a laceration to the radial side of her index finger while cutting vegetables at home. She presented to an outside emergency room where her laceration was repaired. Four days later, she presents to the office complaining of numbness along the radial side of her index finger. On examination, the patient has a 1.5 cm oblique laceration along the volar radial aspect of her index finger distal to the MP joint overlying the proximal phalanx, but is able to flex at the PIP and DIP joints without discomfort. You diagnose her with a radial digital nerve laceration and plan for operative repair.
Treat+EPL+rupture+CASE+44+The+patient+is+a+31yearold+woman+who+sustained+a+laceration+to+the+radial+side+of+her+index+finger+while+cutting+vegetables+at+home+She+presented+to+an+outside+emergency+room+where+her+laceration+was+repaired+Four+days+later+she+presents+to+the+office+complaining+of+numbness+along+the+radial+side+of+her+index+finger+On+examination+the+patient+has+a+15+cm+oblique+laceration+along+the+volar+radial+aspect+of+her+index+finger+distal+to+the+MP+joint+overlying+the+proximal+phalanx+but+is+able+to+flex+at+the+PIP+and+DIP+joints+without+discomfort+You+diagnose+her+with+a+radial+digital+nerve+laceration+and+plan+for+operative+repair++
+What+is+a+normal+twopoint+discrimination+in+the+tip+of+the+index+finger" rel="noopener noreferrer" style="color: #1a5276; font-weight: 600; text-decoration: none; font-size: 0.85rem;" target="_blank">[View Source / PubMed]
Identify the structure that is repaired during digital nerve coaptation?** CASE 45 **[The patient is a 48-year-old, diabetic, male smoker who presents to the emergency room after sustaining a laceration to the volar aspect of his palm with a tablesaw (](file:///C:/Users/DELL/Desktop/hip/board/Chapter%204.%20The%20Hand_Converted.html#bookmark24)[Fig. ](#bookmark24)4–22). In addition to injuring multiple tendons, the patient has injuries to multiple digital nerves and digital arteries. He is brought to the operating room urgently for exploration and repair; his fingers are revascularized and his digital nerves and tendons are repaired. Postoperatively, the patient inquires about his expected neural recovery.


_**Figure 4–22**_
Explain the causes of nerve pain in a damaged nerve? Describe the causes of neuroma?** CASE 46 **The patient is an 18-year-old woman who sustained a laceration to the radial side of her index finger at the level of the PIP joint two and a half weeks prior to her office visit. The injury was sustained when a kitchen knife slipped and accidentally caused a 2 cm laceration to this area. On examination, the patient has anesthesia of the radial side of her index finger distal to the injury, but is able to flex at the PIP and DIP joints without difficulty. Surgery is planned for digital nerve exploration and repair.
Identify nerves used for autologous nerve grafting?** CASE 47 **[The patient is a 74-year-old man involved in a motor vehicle collision who sustained a soft tissue injury to the dorsum of his left hand when it was caught out the window (](file:///C:/Users/DELL/Desktop/hip/board/Chapter%204.%20The%20Hand_Converted.html#bookmark25)[Fig. ](#bookmark25)4–23). He has no other injuries and is otherwise healthy. He
underwent initial debridement followed by extensor tendon repair (extensor digitorum communis to the index and middle fingers as well as the extensor indicis proprius) and is left with an 8 × 8 cm wound over the dorsum of the hand, with exposed extensor tendons.

_**Figure 4–23**_
Describe the indications for a Moberg advancement flap? Identify the anatomy of the thumb?** CASE 49 **[The patient is a 36-year-old otherwise healthy male who presents with a volar soft tissue defect overlying the distal phalanx of the index finger (](file:///C:/Users/DELL/Desktop/hip/board/Chapter%204.%20The%20Hand_Converted.html#bookmark27)[Fig. ](#bookmark27)4–25). The patient reports that this is the result of a locally aggressive infection which required surgical debridement. The infection has been clinically eradicated with local wound care and a course of antibiotics. On examination, the patient has a 2 × 2 cm soft tissue defect of the volar distal phalanx of the index finger extending proximal to the DIP joint, with exposed flexor tendon sheath. The finger is stiff but is sensate and perfused.

_**Figure 4–25**_
Access timing of division for cross finger flaps?** CASE 50 **The patient is a 51-year-old male construction worker who presents with pain in his proximal left palm and a superficial 1 × 1 cm ulcer along the radial aspect of his small finger tip. He reports that he has had pain in his hand for approximately 4 months, but has had the ulcer for only 3 weeks. He operates heavy machinery at work and often uses a jackhammer. On examination, the patient has a normal appearing, sensate hand with an ulcer of his small fingertip. There is no muscular wasting. He has normal range of motion in all fingers and his grip and pinch strength are normal.
+_Discussion_
The+correct+answer+is+E+All+of+the+listed+treatment+options+may+be+helpful+for+this+patient+Smoking+cessation+independent+of+surgical+intervention+may+be+helpful+for+this+patient+to+prevent+disease+progression+The+choice+of+ulnar+artery+ligation+vs+reconstruction+with+a+vein+graft+is+surgeon+and+patientdependent+either+option+might+be+indicated+in+this+scenario+as+described+above+Adjunctive+medications+such+as+antiplatelet+therapy+Aspirin+anticoagulation+and+vasodilators+such+as+calcium+channel+blockers+may+be+helpful+in+cases+of+distal+finger+ischemia+Objectives+Did+you+learn++
Identify+the+indications+for+the+use+of+the+Allens+test+Identify+the+indications+for+Digital+Brachial+Index++
**
