INTRODUCTION TO ATYPICAL EXTREMITY INFECTIONS
The management of atypical and severe extremity infections—encompassing fungal, mycobacterial, and aggressive clostridial pathogens—demands a high index of clinical suspicion, precise diagnostic workup, and decisive surgical intervention. Unlike routine pyogenic infections (e.g., Staphylococcus aureus or Streptococcus species), atypical infections often present with an indolent course, mimicking non-infectious inflammatory conditions, or conversely, as fulminant, limb-threatening emergencies.
This comprehensive guide delineates the evidence-based protocols for diagnosing and surgically managing these complex conditions, providing orthopedic surgeons with the critical frameworks required for limb salvage, functional restoration, and the avoidance of catastrophic surgical pitfalls such as operating on pyoderma gangrenosum.
SEVERE OPEN WOUNDS AND CLOSTRIDIAL MYONECROSIS
Before addressing indolent fungal and mycobacterial pathogens, the orthopedic surgeon must be adept at managing acute, life- and limb-threatening infections, particularly clostridial myonecrosis (gas gangrene) arising from contaminated open fractures or traumatic amputations.
Pathophysiology and Clinical Presentation
Clostridial infections, most commonly driven by Clostridium perfringens, thrive in anaerobic environments created by devitalized tissue. The bacteria produce alpha-toxin (lecithinase), which rapidly destroys cell membranes, causing extensive myonecrosis, hemolysis, and profound systemic toxicity. Clinical hallmarks include severe pain out of proportion to physical findings, tense edema, bronze skin discoloration, hemorrhagic bullae, and palpable crepitus.
Surgical Indications and Preoperative Planning
Immediate, aggressive surgical intervention is the cornerstone of survival. Delaying surgery for imaging (such as MRI) is contraindicated if clostridial myonecrosis is clinically suspected.
Surgical Warning: The presence of gas in the soft tissues on plain radiographs is a late finding. Do not wait for radiographic confirmation if the clinical triad of disproportionate pain, systemic toxicity, and foul-smelling "dishwater" exudate is present.
Step-by-Step Surgical Approach: Radical Debridement
- Positioning and Anesthesia: The patient is positioned supine. General anesthesia is required due to the extensive nature of the debridement. A tourniquet may be applied but should not be inflated initially, as assessing tissue perfusion and bleeding is critical for determining muscle viability.
- Incision: Extensile longitudinal incisions are made, fully releasing the involved fascial compartments to decompress the limb and expose the deep musculature.
- Assessment of Muscle Viability (The 4 Cs):
- Color: Healthy muscle is beefy red; necrotic muscle is dark, pale, or bruised.
- Consistency: Healthy muscle is firm; necrotic muscle is friable or mushy.
- Contractility: Healthy muscle contracts when stimulated with electrocautery or forceps.
- Capacity to Bleed: Healthy muscle bleeds briskly when cut.
- Radical Excision: All necrotic skin, subcutaneous tissue, muscle, and bone must be radically excised. Tissue with questionable viability may be left temporarily but mandates a planned second-look debridement within 24 to 48 hours.
- Amputation: In extreme cases where myonecrosis is irreversible and systemic toxicity is advancing, emergent guillotine amputation is life-saving.
- Wound Management: All wounds suspected of harboring clostridial infection, including amputation stumps, must be left open until the infection is definitively controlled. Primary closure is strictly contraindicated.
Antimicrobial and Adjunctive Therapy
The assistance of an infectious disease consultant is paramount. Empirical antibiotic therapy must be tailored to the mechanism of injury:
* Straightforward Open Fractures: Intravenous cephalosporins (e.g., cefazolin).
* Dirt- or Grease-Contaminated Wounds: Cephalosporin combined with an aminoglycoside (e.g., gentamicin) to cover Gram-negative organisms.
* Crush Injuries or Farm Contamination: High risk for clostridial spores. The regimen must include high-dose intravenous Penicillin G, a cephalosporin, and an aminoglycoside.
Hyperbaric Oxygen Therapy (HBO):
Although considered a controversial adjunct by some, substantial evidence suggests HBO is highly effective in halting alpha-toxin production. Administered at 2 to 2.5 atmospheres (atm) three times daily for acute infections, HBO has been shown to help stabilize limb amputations secondary to clostridial infections and demarcate viable from non-viable tissue.
FUNGAL INFECTIONS OF THE EXTREMITIES
Fungal infections of the musculoskeletal system are rare but highly destructive. They are broadly categorized into three manifestations based on the depth of tissue invasion:
- Cutaneous Infections: Primarily caused by dermatophytes (e.g., Tinea species). These are generally managed medically with topical or systemic antifungals and rarely require surgical intervention.
- Subcutaneous Infections: Often resulting from direct inoculation (e.g., Sporotrichosis, known as "rose gardener's disease"). These present as nodular lymphangitis spreading proximally from the inoculation site.
- Deep or Systemic Infections: These involve deep fascial planes, tendons, joints, and bone. Usual causative organisms include Sporothrix schenckii, Madurella mycetomatis (maduromycosis), Histoplasma capsulatum, Coccidioides immitis, and Blastomyces dermatitidis.
Surgical Indications
While systemic antifungal therapy (e.g., Amphotericin B, Itraconazole, or Voriconazole) is the first line of defense, surgical therapy is absolutely indicated for:
* Fungal flexor or extensor tenosynovitis (to prevent tendon rupture).
* Fungal septic arthritis (to prevent cartilage destruction).
* Fungal osteomyelitis (to remove sequestrum and eradicate the nidus of infection).
Surgical Approach: Fungal Flexor Tenosynovectomy
Fungal tenosynovitis often presents indolently, mimicking rheumatoid tenosynovitis.
- Positioning: Supine with a hand table. A pneumatic tourniquet is applied. Exsanguination should be performed by elevation rather than Esmarch bandage to prevent proximal seeding of the fungus.
- Incision: Brunner zigzag incisions or mid-axial incisions are utilized over the volar aspect of the affected digit, extending into the palm if the infection tracks along the flexor tendon sheath (especially the radial or ulnar bursae).
- Exposure and Protection: The neurovascular bundles are identified and protected using vessel loops.
- Tenosynovectomy: The flexor tendon sheath is opened. Fungal infections often produce a thick, hypertrophic, granulomatous synovium. A meticulous tenosynovectomy is performed, excising all diseased synovium while strictly preserving the critical A2 and A4 pulleys to prevent tendon bowstringing.
- Tissue Sampling: Multiple tissue samples must be sent for aerobic, anaerobic, mycobacterial, and fungal cultures, as well as histopathology (requesting Gomori methenamine silver [GMS] and Periodic acid-Schiff [PAS] stains).
- Irrigation and Closure: The wound is copiously irrigated. Depending on the severity, the wound may be closed loosely over a drain, or left open for delayed primary closure.
MYCOBACTERIAL INFECTIONS
Atypical mycobacteria and Mycobacterium tuberculosis are notorious for causing chronic, progressive infections in the hand and wrist. Because routine bacterial cultures are negative, diagnosis is frequently delayed.
Mycobacterium tuberculosis
The most common presentation of Mycobacterium tuberculosis in the hand is chronic flexor tenosynovitis.
Clinical Presentation:
It classically appears as an extensive palmar "ganglion" or swelling (the compound palmar ganglion). Because the hypertrophic synovium proliferates within the confined space of the carpal tunnel, it frequently causes secondary compression of the median nerve, presenting as acute or subacute carpal tunnel syndrome.
Surgical Management:
Surgical decompression and radical tenosynovectomy are required. The transverse carpal ligament is completely divided to relieve median nerve compression. The surgeon will often encounter "rice bodies"—fibrinous, cartilaginous-appearing nodules within the synovial fluid that are pathognomonic for tuberculous or rheumatoid tenosynovitis. Complete excision of the infected bursae is necessary, followed by a prolonged course (6–12 months) of multi-drug antituberculous chemotherapy (Rifampin, Isoniazid, Pyrazinamide, Ethambutol).
Mycobacterium marinum
Mycobacterium marinum is an atypical, non-tuberculous mycobacterium found in fresh and salt water. Infection typically occurs following minor trauma while handling fish, cleaning aquariums ("fish tank granuloma"), or swimming.
Clinical Presentation:
The infection initially presents as a solitary, violaceous, erythematous nodule at the site of inoculation, most commonly on the dorsum of the hand or fingers. It can progress to superficial ulceration or deep tenosynovitis.
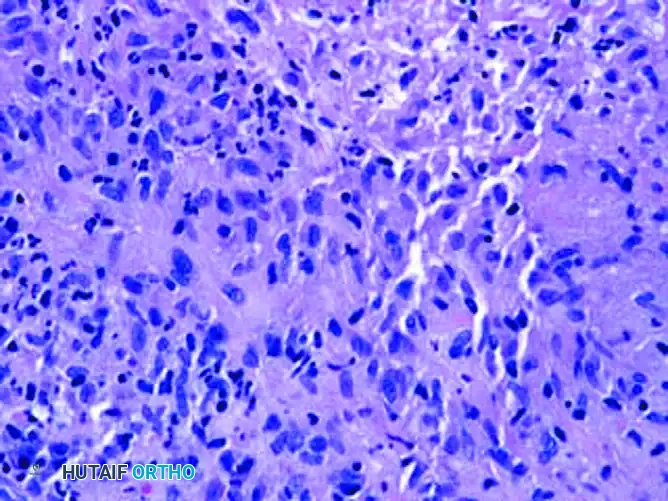
FIGURE 1: A, Three erythematous, tender, exophytic nodules on the dorsum of the hand caused by Mycobacterium marinum infection.
Histopathology:
Diagnosis requires a high index of suspicion. Tissue cultures must be incubated at a cooler temperature (30°C to 32°C) than standard cultures (37°C), as M. marinum is a photochromogen that thrives in cooler extremity temperatures.

FIGURE 2: B, Histopathology shows suppurative and granulomatous inflammation with central necrosis, characteristic of mycobacterial infection.
Surgical and Medical Management:
Superficial cutaneous infections may resolve with targeted antibiotics alone (e.g., Clarithromycin, Ethambutol, or Doxycycline). However, if the infection penetrates the deep fascial layers causing tenosynovitis or septic arthritis, surgical debridement is mandatory. The surgical principles mirror those of fungal tenosynovectomy: meticulous excision of granulomatous tissue, preservation of vital structures, and extensive irrigation.
Clinical Pearl: Always ask patients presenting with chronic, culture-negative hand swelling or nodules about their hobbies, specifically focusing on aquatic activities, fishing, or aquarium maintenance.
PYODERMA GANGRENOSUM: THE SURGICAL MIMIC
Pyoderma gangrenosum (PG) is a rare, non-infectious neutrophilic dermatosis that presents as a rapidly enlarging, painful cutaneous ulcer. It is one of the most dangerous mimics in orthopedic surgery because it is frequently misdiagnosed as a necrotizing soft tissue infection (e.g., necrotizing fasciitis or severe fungal/bacterial ulceration).
Pathogenesis and Clinical Presentation
PG is characterized by a primary sterile inflammatory process. It begins as a painful erythematous papule or pustule that rapidly breaks down into an ulcer with classic violaceous, undermined, and necrotic borders. The wound bed is often purulent and cribriform.
Crucially, PG is associated with underlying systemic autoimmune or inflammatory conditions in up to 50% of cases, most notably:
* Inflammatory Bowel Disease (Ulcerative Colitis, Crohn's disease)
* Rheumatoid Arthritis
* Hematologic malignancies (Myeloproliferative disorders)
The Danger of Pathergy
The hallmark of Pyoderma Gangrenosum is pathergy—an exaggerated inflammatory response to minor trauma or surgical intervention.
Surgical Warning: If a surgeon mistakes Pyoderma Gangrenosum for an infection and performs a surgical debridement, the surgical trauma will trigger a massive pathergic response. The ulcer will rapidly expand, leading to catastrophic tissue loss, exposed tendons/bone, and potentially unnecessary amputation.
Management Strategy
- Recognition: Suspect PG in patients with rapidly expanding, painful ulcers with violaceous borders, especially if routine cultures are repeatedly negative and the patient fails to respond to broad-spectrum antibiotics.
- Consultation: Immediate dermatological and rheumatological consultation is required to avoid inappropriate surgical treatments.
- Medical Therapy: The treatment for PG is strictly medical, focusing on profound immunosuppression. High-dose systemic corticosteroids (e.g., Prednisone) are the first-line therapy. Steroid-sparing agents such as Cyclosporine, Infliximab, or Tacrolimus may be required for refractory cases.
- Wound Care: Gentle, non-traumatic local wound care is utilized. Aggressive sharp debridement is absolutely contraindicated.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
For patients who have undergone surgical debridement for fungal, mycobacterial, or clostridial infections, postoperative management is as critical as the surgery itself.
- Immobilization: Immediately postoperatively, the extremity should be splinted in the "safe position" (intrinsic plus position: wrist extended 20-30 degrees, MCP joints flexed 70-90 degrees, IP joints fully extended) to prevent collateral ligament contracture.
- Elevation: Strict elevation of the limb above the level of the heart is maintained to reduce edema and improve microvascular perfusion.
- Infectious Disease Integration: Antimicrobial therapy must be guided by definitive culture and sensitivity results. Fungal and mycobacterial infections often require months of systemic therapy. Regular monitoring of hepatic and renal function is necessary due to the toxicity of agents like Amphotericin B and Isoniazid.
- Rehabilitation: Once the acute infectious process is controlled and wound healing is progressing, early active and passive range of motion (ROM) exercises are initiated under the guidance of a specialized hand therapist. Tendon gliding exercises are crucial to prevent the severe adhesive tenosynovitis and stiffness that commonly follow deep space infections of the hand.
CONCLUSION
The management of atypical extremity infections requires a sophisticated understanding of microbiology, pathology, and surgical anatomy. Orthopedic surgeons must be prepared to perform radical, life-saving debridements for clostridial myonecrosis, execute meticulous, structure-preserving tenosynovectomies for fungal and mycobacterial pathogens, and exercise profound clinical restraint when faced with inflammatory mimics like pyoderma gangrenosum. Through a combination of aggressive surgical intervention when indicated, targeted antimicrobial therapy, and multidisciplinary collaboration, optimal functional outcomes and limb salvage can be achieved.
📚 Medical References
- Atypical hand infections, Hand Clin 14:613, 1998.
- Huang HW, Strauch RJ: Extensor pollicis longus tenosynovitis: a case report and review of the literature, J Hand Surg 25A:577, 2000.
- Huang JI, Seeger LL, Jones NF: Coccidioidomycosis fungal infection in the hand mimicking a metacarpal enchondroma, J Hand Surg 25B:475, 2000.
- Huish SB, de La Paz EM, Ellis PR III, Stern PJ: Pyoderma gangrenosum of the hand: a case series and review of the literature, J Hand Surg 26A:679, 2001.
- Hurst LC, Amadio PC, Badalamente MA, et al: Mycobacterium marinum infections of the hand, J Hand Surg 12A:428, 1987.
- Hurst LC, Gluck R, Sampson SP, et al: Herpetic whitlow with bacterial abscess, J Hand Surg 16A:311, 1991.
- Janes PC, Mann RJ: Extracutaneous sporotrichosis, J Hand Surg 12A:441, 1987.
