INTRODUCTION TO VASCULARIZED BONE GRAFTING
The reconstruction of massive skeletal defects—whether secondary to trauma, tumor resection, or recalcitrant nonunion—often exceeds the biological capacity of conventional non-vascularized autografts. In these challenging clinical scenarios, the free vascularized bone graft (VBG) remains the gold standard. By transferring living bone with its intrinsic blood supply preserved via microvascular anastomosis, the graft bypasses the protracted process of creeping substitution. This results in accelerated union, resistance to infection, and the ability to undergo primary bone healing even in irradiated or highly compromised recipient beds.
While the free vascularized fibula is the workhorse for long-bone diaphyseal reconstruction, other donor sites offer unique anatomical and biomechanical advantages. The free iliac crest bone graft provides massive corticocancellous volume ideal for metaphyseal defects; the medial femoral condyle (MFC) flap is unparalleled for small, recalcitrant nonunions (e.g., scaphoid); and composite rib grafts offer unique contouring capabilities for specialized reconstructions.
This comprehensive guide details the surgical anatomy, harvesting techniques, fixation strategies, and critical preoperative considerations for these advanced microvascular donor sites.
FREE ILIAC CREST BONE GRAFT
The vascularized iliac crest graft is highly valued for its natural curvature and its dense, rich cancellous bone, which promotes rapid integration at the recipient site. It is particularly indicated for mandibular reconstruction, complex metaphyseal defects, and pelvic ring reconstructions.
Surgical Anatomy and Blood Supply
The vascularized iliac crest flap is based on the Deep Circumflex Iliac Artery (DCIA) and its accompanying venae comitantes (DCIV). The DCIA arises from the lateral aspect of the external iliac artery, just superior to the inguinal ligament. It courses laterally and superiorly toward the anterior superior iliac spine (ASIS), running in the transversalis fascia.
Crucially, the DCIA provides nutrient vessels that penetrate the inner table of the ilium. These vessels arborize extensively within the iliacus muscle before entering the bone.
Surgical Pearl: Preserving the Nutrient Supply
When harvesting the free iliac crest bone graft, it is mandatory to retain the covering of the iliacus muscle on the inner table of the iliac crest. Stripping this muscle will sever the nutrient blood supply to the bone, effectively converting a vascularized graft into a non-vascularized one and leading to catastrophic graft failure.
Harvesting Technique: Step-by-Step
- Positioning: The patient is placed supine with a sandbag under the ipsilateral hip to elevate the pelvis. The entire hemi-pelvis and lower abdomen are prepped and draped.
- Incision: The incision is made parallel to and approximately 2 cm superior to the inguinal ligament, extending from the femoral pulse laterally toward the ASIS, and continuing posteriorly along the iliac crest.
- Pedicle Dissection: The external oblique aponeurosis is incised, and the internal oblique and transversus abdominis muscles are carefully divided to expose the transversalis fascia. The DCIA and DCIV are identified near their origin at the external iliac vessels and traced laterally.
- Muscle Cuff Preservation: As the dissection proceeds toward the ilium, a 2 to 3 cm cuff of the internal oblique, transversus abdominis, and iliacus muscles must be maintained attached to the inner table of the crest to protect the ascending branch and nutrient vessels.
- Osteotomy: Using an oscillating saw and sharp osteotomes, the required length and depth of the iliac crest are harvested. The cuts are made from the outer table inward, ensuring the inner table and its muscular pedicle remain undisturbed.
- Pedicle Ligation: Once the bone is fully mobilized and the recipient site is prepared, the DCIA and DCIV are ligated at their origin, and the composite graft is transferred.
Donor Site Closure and Morbidity Management
Closure of the iliac crest donor site is notoriously challenging due to the resection of the abdominal wall musculature insertions. Failure to achieve a robust closure can result in a devastating incisional hernia.
Surgical Warning: Donor Site Closure
The donor site must be closed in multiple robust layers. To facilitate primary closure and reduce tension on the abdominal wall musculature, the donor site may be closed primarily by flexing the hip. Postoperatively, the patient should be maintained in a slightly flexed "beach chair" position for the first 5 to 7 days.
Recipient Site Fixation Challenges
Placing and securing the iliac crest bone graft in the recipient site presents unique biomechanical challenges compared to the fibula.
- Length Constraints: Because the iliac graft is relatively short, fixation techniques that consume bone length—such as insetting or doweling the graft into the medullary canal of the host bone—may severely compromise the overall length of the reconstruction.
- Hardware Limitations: Difficulty may be encountered in attaching a standard dynamic compression plate to an iliac crest graft. The natural curvature of the ilium and the varying thickness of its cortices make plate contouring and screw purchase unpredictable.
- Preferred Fixation Methods: Fixation of the iliac crest graft into the recipient site may be more difficult than fixation of the fibula. Fixation is often best achieved using an external fixation device, which spans the defect and neutralizes forces without requiring direct hardware application to the graft. Alternatively, a combination of limited internal fixation devices with independent lag screws can be utilized to secure the graft at the host-graft junctions while preserving the delicate periosteal and muscular blood supply.
MEDIAL FEMORAL CONDYLE (MFC) CORTICOCANCELLOUS FLAP
While the iliac crest provides massive structural volume, the Medial Femoral Condyle (MFC) flap has revolutionized the treatment of small, recalcitrant nonunions, particularly in the upper extremity (e.g., scaphoid nonunions, clavicle defects, and limited segmental defects of the forearm).
Anatomy and Indications
The MFC flap is a periosteal or corticocancellous flap based on the Descending Genicular Artery (DGA) or, less commonly, the Superomedial Genicular Artery (SMGA). The DGA arises from the superficial femoral artery just proximal to the adductor hiatus. It provides a robust, consistent vascular arborization to the periosteum and underlying cancellous bone of the medial femoral condyle.
The primary advantage of the MFC flap is its ability to provide highly vascularized, structurally sound cancellous bone that can be precisely contoured to fit complex three-dimensional defects, such as the proximal pole of the scaphoid.
Surgical Approach to the MFC
- Incision: A longitudinal incision is made over the medial aspect of the distal thigh, centered over the vastus medialis.
- Dissection: The vastus medialis is elevated anteriorly, exposing the medial intermuscular septum.
- Pedicle Identification: The DGA is identified as it emerges from the superficial femoral artery and courses over the medial femoral condyle.
- Harvest: A corticocancellous block is outlined with a surgical marker. Using a thin oscillating saw and sharp osteotomes, the bone block is harvested, ensuring the periosteal blood supply remains meticulously attached to the underlying cortex.
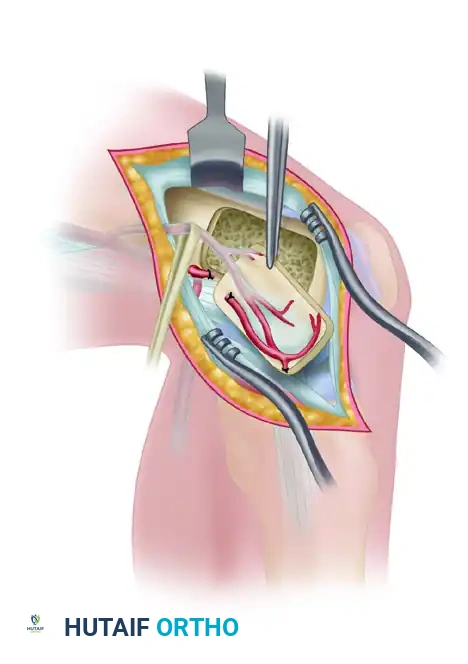
FIGURE 63-47: Flap elevated from the medial femoral condyle, demonstrating the vascular pedicle and the harvested corticocancellous block prior to microvascular transfer.
HARVESTING COMPOSITE RIB GRAFTS
Vascularized rib grafts offer a unique combination of bone and, if necessary, overlying soft tissue or cartilage. They are historically significant in mandibular reconstruction, spinal fusion (particularly in irradiated beds), and complex facial reconstructions.
Types of Vascularized Rib Grafts
Two distinct types of vascularized rib grafts are used clinically, differentiated by their vascular supply:
- The Posterior Rib Graft: This graft is harvested with its nutrient vessels intact, providing both medullary and periosteal circulation. It relies on the proximal intercostal artery.
- The Posterolateral (Segmental) Rib Graft: This graft is supplied solely by periosteal vessels derived from the intercostal muscle cuff harvested with the rib.
Despite the anatomical differences in blood supply, clinical and experimental data demonstrate that the viability of these two types of grafts is similar, provided the microvascular anastomosis is successful.
Preoperative Planning: The Artery of Adamkiewicz
Harvesting a rib graft carries a unique and potentially devastating neurological risk: spinal cord ischemia. The blood supply to the lower thoracic and upper lumbar spinal cord is highly dependent on a dominant radicular artery.
🚨 CRITICAL SURGICAL WARNING: SPINAL CORD ISCHEMIA
Selective arteriography is absolutely necessary prior to rib harvest to assess the location of the arteria radiculomedullaris magna (Artery of Adamkiewicz). This critical vessel usually arises from the dorsal branch of the lower intercostal or upper lumbar arteries, predominantly on the left side (in approximately 75% of patients).
It is paramount to establish the exact anatomical location of this artery to determine that it does not originate from the chosen intercostal artery. Ligation of the intercostal artery that gives rise to the artery of Adamkiewicz will result in anterior spinal artery syndrome, leading to irreversible paraplegia.
Surgical Technique and Donor Site Selection
Because of the anatomical variability and the risks associated with the lower thoracic vessels, donor site selection must be meticulous.
- Preferred Donor Site: Ostrup and other pioneers in microvascular surgery recommended the use of the ninth rib (left or right) as the primary donor site for microvascular free rib grafts. The 9th rib provides adequate length, a reliable intercostal pedicle, and generally avoids the most common origins of the artery of Adamkiewicz (though angiography remains mandatory).
- Harvesting Technique: The patient is placed in the lateral decubitus position. An incision is made directly over the chosen rib. The latissimus dorsi and serratus anterior muscles are divided. The periosteum of the superior rib and the inferior rib is preserved, but the intercostal muscles attached to the harvested rib are kept intact to preserve the vascular pedicle. The rib is osteotomized anteriorly and posteriorly, and the intercostal artery and vein are dissected proximally to obtain adequate pedicle length before ligation and transfer.
- Pleural Management: Extreme care must be taken to avoid breaching the parietal pleura. If a pleural tear occurs, it must be meticulously repaired, and a chest tube may be required to prevent pneumothorax.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative management of patients undergoing free vascularized bone grafting—whether iliac crest, MFC, or rib—requires a multidisciplinary approach focused on flap survival and optimal bone healing.
Postoperative care is broadly similar to that described for the free vascularized fibular graft. Key principles include:
- Hemodynamic Stability: Maintaining adequate systemic blood pressure and hydration to ensure optimal perfusion across the microvascular anastomosis. Vasopressors are generally avoided if possible, as they can induce vasospasm in the pedicle.
- Flap Monitoring: If a chimeric flap was harvested (e.g., an iliac crest graft with an overlying skin paddle), the skin paddle serves as a reliable clinical monitor for the buried bone graft. In purely osseous grafts, an implantable venous Doppler is often utilized for the first 5 to 7 days to continuously monitor anastomotic patency.
- Immobilization: The recipient site must be rigidly immobilized. Because vascularized grafts bypass creeping substitution, they heal via primary bone healing. However, the graft is initially mechanically weak. External fixators or customized orthoses are maintained until radiographic evidence of bridging callus is observed at the host-graft junctions.
- Donor Site Care:
- Iliac Crest: Hip flexion is maintained to protect the abdominal closure. Early mobilization is encouraged, but core-straining activities are strictly prohibited for 6 to 8 weeks.
- Rib: Aggressive pulmonary toilet, incentive spirometry, and adequate analgesia are critical to prevent atelectasis and pneumonia following rib harvest.
- Weight-Bearing: For lower extremity reconstructions, patients remain strictly non-weight-bearing until radiographic union is confirmed, followed by a protracted period of progressive, protected weight-bearing to allow the graft to hypertrophy in response to mechanical stress (Wolff's Law).
