

DEFINITION
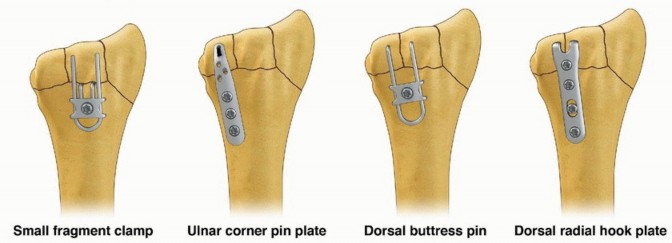
Fragment-specific fixation is a treatment approach for complex articular fracture patterns characterized by independent fixation of each major fracture component with an implant specific for that particular fragment ( FIG 1).Fragment-specific implants are usually low profile and have a certain degree of “spring-like” elasticity; the combination of independent fixation of multiple fragments in different planes can restore articular anatomy without the need for effective thread purchase in small periarticular fragments.Surgical planning is extremely important to determine whether a single approach or a combination of surgical approaches is needed to visualize and fix each of the main fracture components that make up a particular injury. For distal radius fixation, a complete set of implants should be available to address any of the five primary fracture elements: the radial column, ulnar corner, volar rim, dorsal wall, and/or impacted articular fragments. In addition, identification and treatment of distal radioulnar joint (DRUJ) disruption and injuries of the ulnar column should be included.
FIG 1 • FRAGMENT-SPECIFIC IMPLANTS.
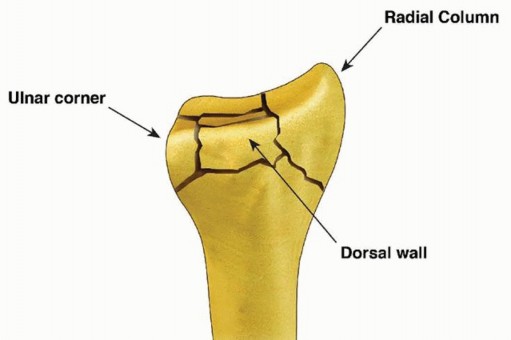
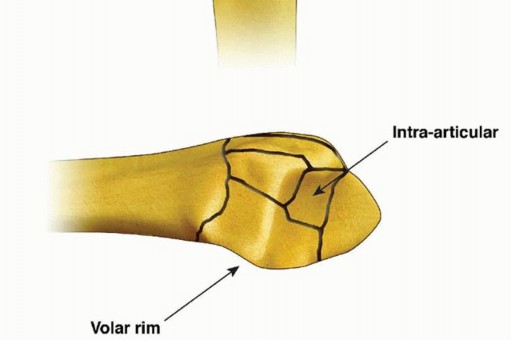
FIG 2 • Articular fracture components.
ANATOMY
ESSENTIAL BASIC ANATOMY
The palmar cutaneous branch of the median nerve typically lies in the subcutaneous tissue between the tendons of the flexor carpi radialis (FCR) and palmaris longus; radial-based incisions shouldnotextend distally into a carpal tunnel approach in order to avoid injury to this nerve.The terminal branches of the lateral antebrachial cutaneous nerve and dorsal sensory branch of the radialnerve run in the subcutaneous tissue radial to the course of the radial artery. Exposure of the radial column by elevating a radial skin and subcutaneous flap using blunt dissection from a proximal to distal direction along the surface of the first dorsal compartment tendons helps avoid injury to these structures.The pronator quadratus inserts along the ridge at the distal flare of the radius; dissection distally should be limited to no more than 1 to 2 mm distal to the ridge to avoid compromise of the important volar carpal ligaments.
ESSENTIAL OSSEOUS ANATOMY
Structurally, the wrist can be thought of in terms of three basic support columns: a radial column that includes the radial border of the distal radius and scaphoid facet, a middle column consisting of the central and ulnar part of the radial shaft and lunate facet, and an ulnar column that includes the DRUJ, the triangular fibrocartilage complex (TFCC), and the ulnar head.The radial column fragment involves the pillar of bone along the radial border of the distal radius ( FIG 2). Restoration of radial length is important to correct the axial position of the carpus, unloading deforming compressive forces that can interfere with reduction of middle column injuries. Typically, the terminal portion of the brachioradialis inserts on the base of the radial column fragment and may be a deforming force that contributes to proximal displacement of the radial column fragment. Metaphyseal comminution along the base of the radial column fragment may also contribute to radial column instability. Although not common, radial column injuries with secondary coronal fracture page or segmental comminution into the shaft proximally can be particularly unstable fracture patterns.The volar rim of the lunate facet is a primary load-bearing structure of the articular surface. Instability of the volar rim occurs in two patterns:In the volar instability pattern, the volar rim migrates in a proximal and volar direction resulting in secondary palmar translation of the carpus.In the axial instability pattern of the volar rim, axial impaction of the carpus drives the volar rim into dorsiflexion, resulting in secondary axial and dorsal subluxation of the carpus.The ulnar corner fragment involves the dorsal half of the sigmoid notch and usually includes a small dorsal ulnar corner of the articular surface of the lunate facet. This fracture component is the result of impaction of the lunate into the articular surface, causing the fragment to migrate dorsally and shorten proximally. Residual displacement of the ulnar corner may result in instability of the DRUJ as well as restriction of forearm rotation.Dorsal wall fragmentation may be a typical finding in either dorsal bending or axial loading injuries. If displaced, this fracture component is often associated with dorsal subluxation of the carpus in addition to the typical dorsal angulation of the articular surface.Free articular fragments may be impacted within the metaphyseal cavity and result in incongruity of the articular surface. Elevation of dorsal wall fragments allows direct access to reduction of free articular fragments.
PATHOGENESIS


FIG 3 • Pathogenesis of dorsal radius fractures. A. Dorsal bending. B. Volar bending. C. Dorsal shear. D. Volar shear. E. Radial shear. F. Three-part articular. G. Comminuted articular. H. Carpal avulsion. I. High energy.
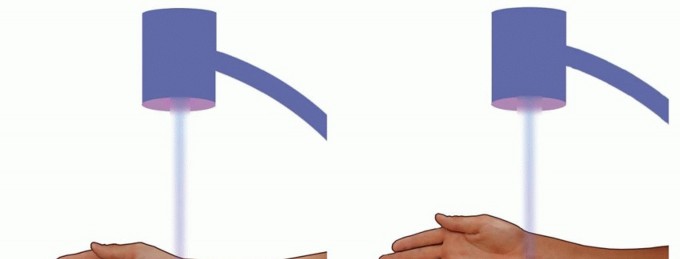
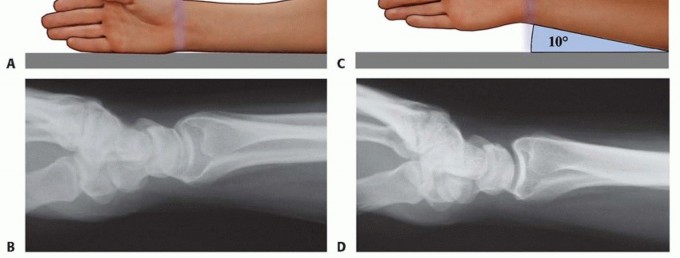
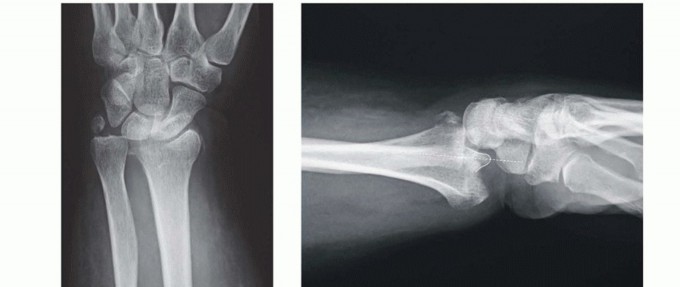
FIG 4 • A. Positioning for standard lateral radiography. B. Standard lateral radiograph. C. Positioning for 10-degree lateral radiography. D. Ten-degree lateral radiograph. Note the improved visualization of the articular surface of the base of the scaphoid facet and the entire lunate facet. Injuries from a high-energy mechanism present as complex comminuted fractures of the articular surface with extension into the radial/ulnar shaft ( FIG 3I).
IMAGING AND OTHER DIAGNOSTIC STUDIES

SURGICAL MANAGEMENT
OPERATIVE INDICATIONS
General parametersShortening of more than 5 mmRadial inclination of less than 15 degrees Dorsal angulation of more than 10 degrees Articular step-off of more than 1 to 2 mmDepression of teardrop angle to less than 45 degrees Volar instabilityDRUJ instabilityDisplaced articular fracturesYoung, active patients are generally less tolerant of residual deformity and malposition.
PREOPERATIVE PLANNING
Extra-articular fractures: multiple optionsVolar plating through a volar approach Dorsal plating through a dorsal approachFragment-specific fixationRadial pin plate (TriMed, Inc., Valencia, CA) and volar buttress pin (TriMed, Inc.) fixation through a limited incision volar or standard volar approachRadial pin plate and either an ulnar pin plate dorsally or a dorsal buttress pin through a dorsal or combined approachFixed-angle radial column plate using either a volar or dorsal radial column exposure Volar hook plates with or without radial column plate using a volar approachIntra-articular fractures: Surgical approach is based on the fragmentation pattern.Unstable volar rim fragments require a standard volar or rarely an ulnar-based volar approach for adequate visualization.Fixation of the radial column can be done either through a limited-incision volar radial approach (Henry), a volar approach with radial extension combined with pronation of the forearm, or a dorsal approach with radial extension combined with supination of the forearm.Fixation of dorsal, ulnar corner, and free intra-articular fragments can be done through a dorsal approach.
POSITIONING
The patient is supine.The affected arm is placed on an arm board out to the side. C-armIf the arm board is radiolucent, the C-arm can be brought in from the end of the arm board and images taken directly with the wrist on the arm board.If the arm board is not radiolucent, the C-arm is brought in along the side of the table from the foot, and the arm is brought off the arm board for each image.
OPERATIVE SEQUENCE
Initial restoration of radial column length with traction and provisional trans-styloid pin fixation can be helpful to hold the carpus out to length and unload the lunate facet.The volar rim is reduced and fixed. For complex injuries, this is usually the keystone on which to build stable fixation.The dorsal ulnar corner is reduced and fixed if necessary.Free intra-articular fragments and the dorsal wall fragments are reduced and stabilized as necessary. Bone graft is applied if the metaphyseal defect is large.Fixation is completed with a radial column plate.Depending on the nature of the fracture, fixation may be a subset of these steps.
APPROACH
TECHNIQUES
Limited-Incision Volar Approach
Make a longitudinal incision along the radial side of the radial artery.
Proximally, insert the tip of a tenotomy scissors over the surface of the first dorsal compartment sheath and sweep distally to elevate a radial skin flap.
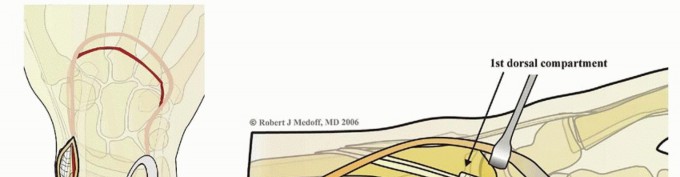
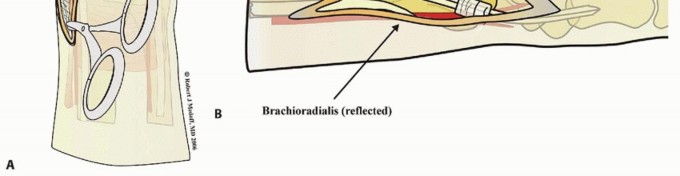
Pronate the forearm and sharply expose the bare area of bone over the radial styloid situated in the interval between the first and second dorsal compartments ( TECH FIG 1A).
Leaving the distal 1 cm of sheath intact, open the first dorsal compartment proximally and mobilize the tendons. Reflect the insertion of brachioradialis to complete exposure of the radial column ( TECH FIG 1B).
LIMITED-INCISION VOLAR APPROACH
TECH FIG 1 • Limited-incision volar approach. A. Sweeping tenotomy scissors to elevate radial skin flap off first dorsal compartment. B. Deep exposure of the radial column.
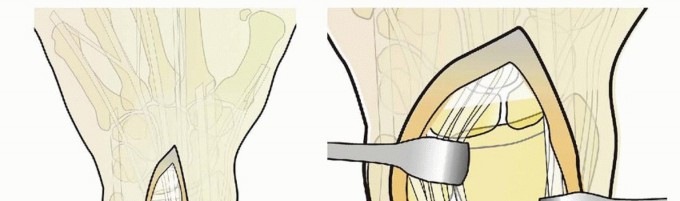
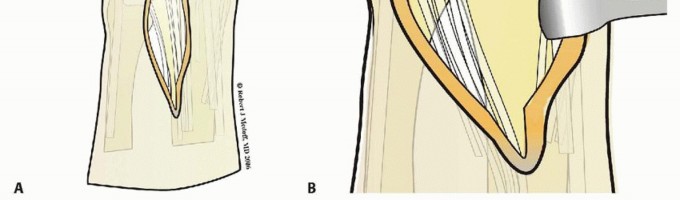
TECH FIG 2 • Dorsal approach. A. Initial incision. B. Deep exposure.
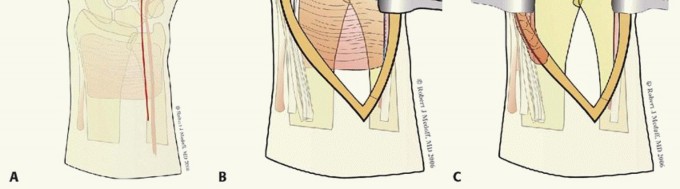
EXTENSILE VOLAR APPROACH



TECH FIG 3 • Extensile volar approach. A. Initial incision. B. Line of incision in pronator quadratus. C.


TECH FIG 4 • Volar ulnar approach. A. Incision. B. Initial exposure. C. Completed exposure. Retract the contents of the carpal tunnel to the radial side ( TECH FIG 4C).Reflect the pronator quadratus from its ulnar and distal attachment. Do not dissect more than 1 to 2 mm beyond the distal radial ridge to avoid detachment of the volar wrist capsule.5. Volar Rim Fragment
SMALL FRAGMENT PLATE FIXATION
Small fragment volar plate fixation may be indicated for treatment of a volar instability pattern of the volar rim. The fragment must be of adequate size to allow buttressing on the volar surface by the plate ( TECH FIG 5A,B).If volar rim fragmentation is associated with an axial instability pattern, the fragment must be of adequate size and strength to allow angular correction of the dorsiflexion deformity with distal locked screw purchase.An appropriate volar approach is used to expose the volar rim fragment. If a shortened radial column fragment is present, restoring radial length and provisionally holding with a trans-styloid Kirschner wire may simplify reduction by unloading the lunate facet.Reduce the volar rim fragment; this should restore normal carpal alignment.Apply a small fragment volar plate and fix it proximally with cortical bone screws. If needed, secure the distal fragment with standard or locking bone screws ( TECH FIG 5C,D).
VOLAR BUTTRESS PIN FIXATION
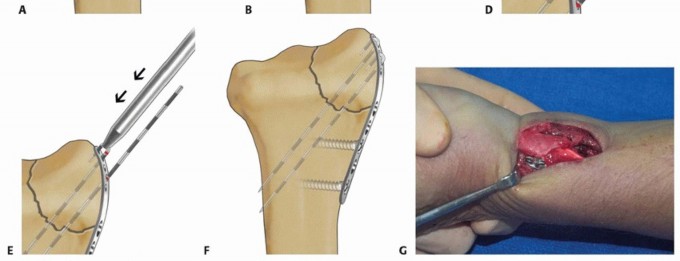
TECH FIG 5 • Volar rim fixation with small fragment plate. A,B. Shear fracture of volar rim with volar instability pattern. C,D. Fixation with small fragment plate.
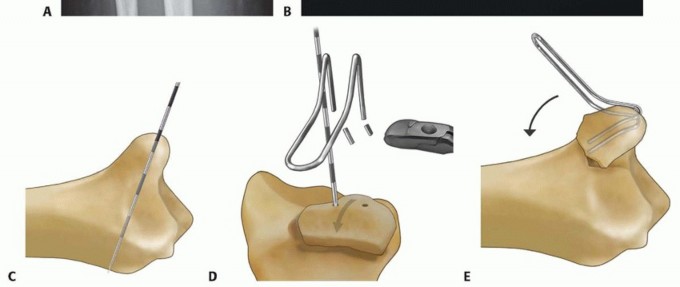
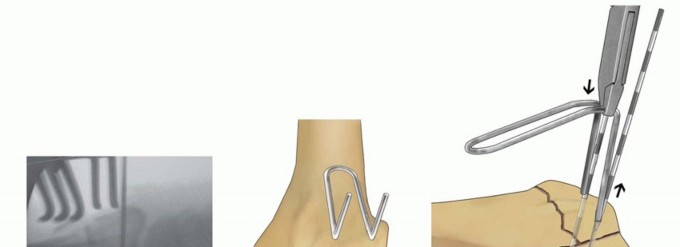
TECH FIG 6 • Volar rim fixation with a volar buttress pin. A,B. Articular fracture with axial instability pattern of volar rim. C. Insertion of Kirschner wires. D. Cutting and inserting legs. E. Reduction of teardrop.(continued)

TECH FIG 6 •(continued)F. Completed fixation. G,H. Volar buttress pin fixation to control rotational alignment of volar rim fragment. Fine-tune the reduction and fix it proximally with a minimum of two screws and washers ( TECH FIG 6F-H). If needed, a blocking screw can be placed just proximal to the end of the buttress pin to prevent shortening of the fragment. Alternatively, a wire plate can be used to secure the implant proximally.
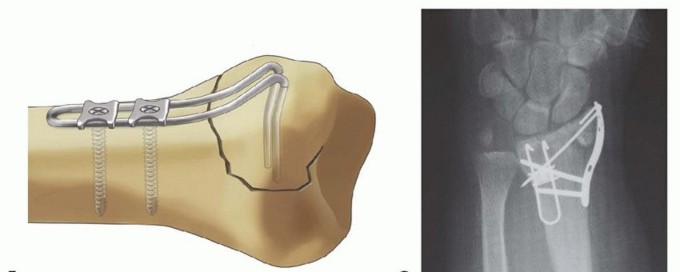
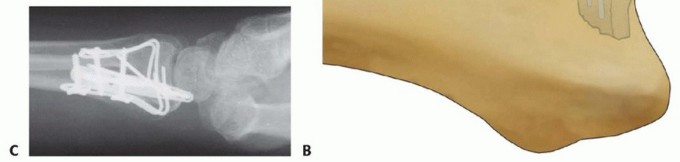
VOLAR HOOK PLATE FIXATION
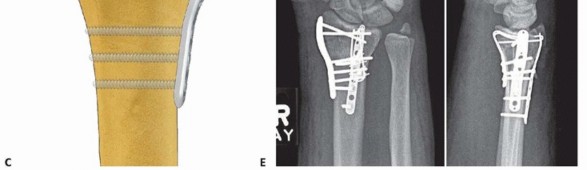
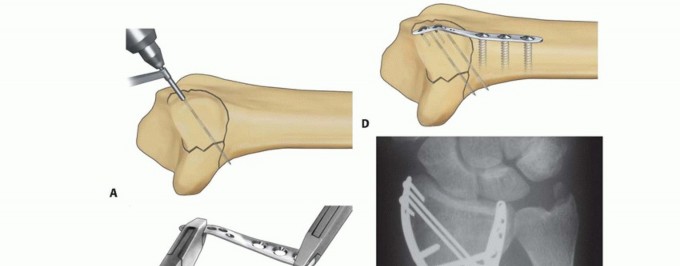
TECH FIG 7 • Volar rim fixation with a volar hook plate. A. Insertion of volar hook plate over guide pin through predrilled holes. B. Completed fixation. C. Final intraoperative x-ray showing placement of two volar hook plates into separate distal rim fragments.
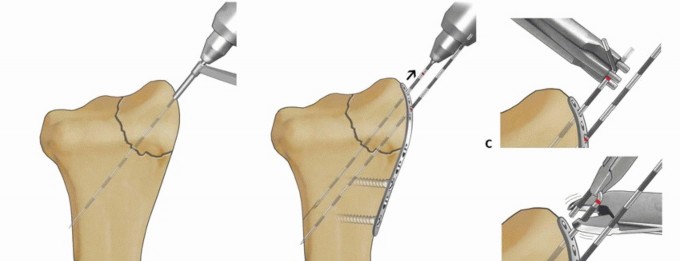
TECH FIG 8 • Radial column fixation with radial pin plate. A. Insertion of trans-styloid Kirschner wire. B,C.


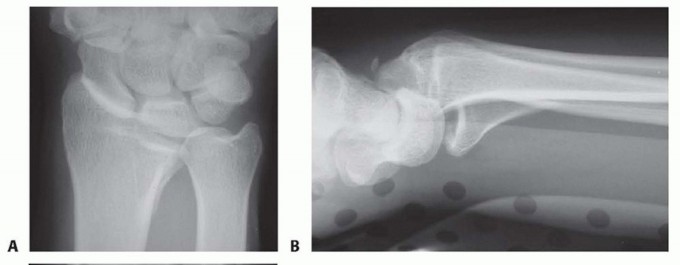
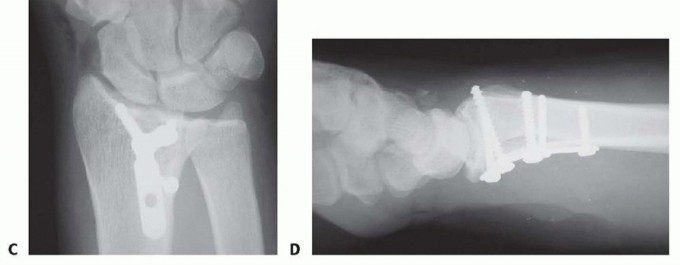
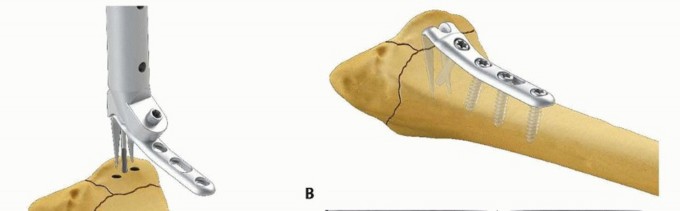
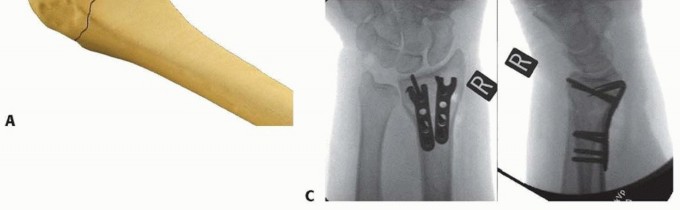
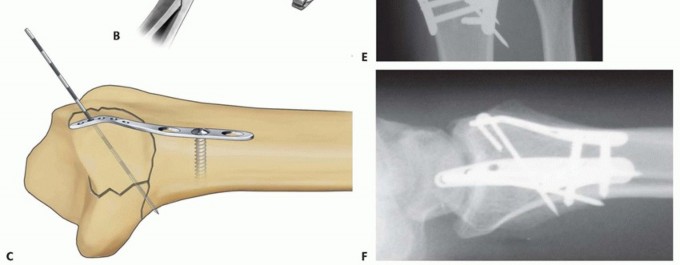
TECH FIG 9 • Radial column fixation with fixed-angle radial column plate. A. Provisional placement of fixed-angle radial column plate. B. Drilling holes for distal fixed-angled pegs. C. Completed fixation. D. Unstable fracture injury films with segmental radial column comminution. E. Films 2 months postoperatively. Fixed-angle radial column support is used to avoid radial column shortening. Using fixed-angle drill guides, drill, measure, and insert locking fixation pegs of appropriate length into the distal fixed-angle holes in the plate and standard bone screws proximally into the shaft ( TECH FIG 9B-E).P.2873. Ulnar Corner and Dorsal Wall Fixation
ULNAR PIN PLATE
TECH FIG 10 • Ulnar corner fixation with an ulnar pin plate. A. Insertion of the interfragmentary Kirschner wire. B. Contouring the plate. C. Application of the plate and insertion of the initial fixation screw. D. Fixation completed. E,F. Radial and ulnar pin plate fixation of a three-part articular pattern (radial column and ulnar corner fragment). Slide the plate over the Kirschner wire and fix it proximally with a 2.3-mm bone screw ( TECH FIG 10C).Insert a second Kirschner wire if the fragment is large enough. Create and impact hooks as described for the radial pin plate ( TECH FIG 10D-F).If the Kirschner wire tips protrude beyond the volar cortex, they can be cut flush to the bone surface through a volar incision.
DORSAL BUTTRESS PIN
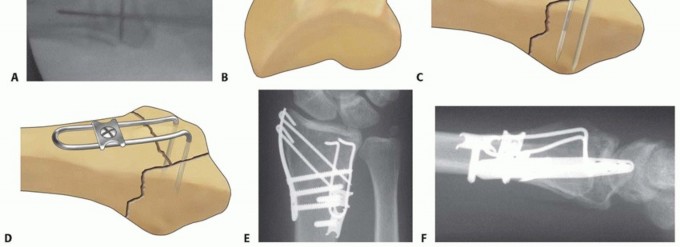
TECH FIG 11 • Dorsal buttress pin fixation. A. The position of the Kirschner wires is checked with a Carm before inserting the implant. B. Placing an implant upside-down on bone to template the trajectory of the Kirschner wires. C. Inserting the dorsal buttress pin. D. Buttress pin fixation completed. E,F. Fixation of a three-part articular fracture with radial column and ulnar corner fragment with radial column plate and dorsal buttress pin. Ensure that the leading tips of the legs of the dorsal buttress pin are straight and cut to the required length. Leave the ulnar leg 2 to 3 mm longer than the radial leg so one leg can be engaged at a time. Direct the legs proximally if needed to match the insertion angle of the Kirschner wires.Place the ulnar leg of the buttress pin adjacent to the insertion site of the ulnar Kirschner wire, and then withdraw the Kirschner wire and immediately engage the leg in the hole ( TECH FIG 11C). Repeat with the radial Kirschner wire to engage the radial leg of the buttress pin. Impact and seat the buttress pin (TECH FIG 11D).Fine-tune the reduction and complete the fixation proximally with one or two 2.3-mm cortical bone screws and washers ( TECH FIG 11E,F). If needed, a blocking screw can be placed just proximal to the end of the buttress pin to prevent shortening of the fragment.
DORSAL HOOK PLATE FIXATION

TECH FIG 12 • Dorsal hook plate fixation. A. Placement of dorsal hook plate. B. Completed fixation.
Free Articular Fragment Support with a Buttress Pin
Free articular fragments impacted into the metaphyseal cavity can be reduced and stabilized by providing support to the subchondral surface of the fragment, in combination with peripheral cortical stabilization circumferentially around the articular fragment.
In some cases, impacted free articular fragments may be adequately supported by a properly applied locking plate to provide subchondral support.
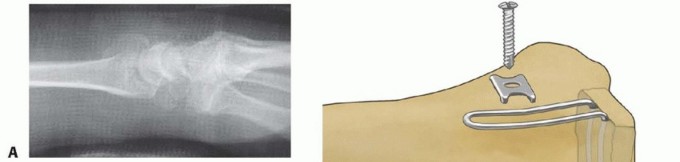
Free Articular Fragment Support with a Buttress Pin TECH FIG 13 • A. Depressed articular fragment. B. Support of free articular fragment with a buttress pin. C. Dorsal buttress pin to support fragment from endosteal surface. An alternative method is to use structural bone graft to support the free articular fragment in combination with fragment-specific fixation of the surrounding cortical shell, resulting in containment of the graft within the metaphysis.A dorsal buttress pin can also be used for direct subchondral support of impacted articular fragments. The legs of the implant are cut to length and inserted through the dorsal defect, slid distally directly behind the articular fragment, and then fixed proximally with a screw and washer. The articular fragment is sandwiched between the base of the lunate and the legs of the implant ( TECH FIG 13A-C).P.290PEARLS AND PITFALLS
COMPLICATIONS
Missed fragment: fracture displacement after surgery9.Careful analysis of radiographic features both before and during reduction; CT scan when needed.10.Preoperative planning to select approaches that allow complete visualization of all major fragments.11.Complete set of implants and instruments available before surgery.12.Evaluate stability of fixation with range of motion under observation before closing operative incision.Loss of radial length: proximal migration of articular surface13.Graft the metaphyseal defect when needed with structural bone graft.14.Use implants that buttress the subchondral bone.DRUJdysfunction: pain,1.Assess clinical stability of DRUJ at the end of procedure.2.Use radial column plate to push distal fragment against ulna to seat sigmoid notch against ulnar head.|instability, or ▪ Evaluate and repair TFCC and capsular tears when necessary.limitation of ▪ Reduce and fix ulnar corner and volar rim fragments to restore congruity of forearm sigmoid notch.rotation ▪ Ensure that radial length is restored.1.Mild, uncomplicated postoperative ulnar-sided wrist pain often spontaneously resolves over 6-12 months.Stiffness: ▪ Early range of motion and mobilization of soft tissuesslow, ▪ Avoidance of constricting bandages and postoperative swelling restricted ▪ Consider occupational therapy when needed.return of movement of wrist, forearm, and fingers; associated with painTendinitis or ▪ Use implants that have a low distal profile.rupture: pain ▪ Avoid placing sharp, bulky edges of hardware in proximity to tendons. with resisted ▪ Cover plates distally with retinacular flap when needed.motion, loss ▪ Consider use of buttress pins (which have a very low profile) when possible. of tendon ▪ Remove any pins or hardware that back out or become prominentfunction, postoperatively.clicking and ▪ Ensure that volar plates do not extend up beyond distal volar ridge into soft pain tissues.2.Avoid long screws or pins, particularly when placed from volar to dorsal. Distal screws should normally be 2-4 mm shy of the dorsal cortical margin.|------P.291
POSTOPERATIVE CARE
At the end of the surgical procedure, confirm the stability of fixation as well as the stability of the DRUJ.If stable, apply a removable wrist brace and instruct the patient to initiate gentle range-of-motion exercises of the fingers, wrist, and forearm twice or more daily as tolerated. For noncompliant patients or injuries with tenuous fixation, use a cast for 2 to 3 weeks postoperatively or until radiographic evidence of healing is identified.Avoid resistive loading across the wrist until signs of radiographic healing are present; typically, this occurs by 4 weeks postoperatively. Specifically instruct older patients not to push up out of a chair or lift heavy objects after surgery.If there is persistent stiffness after 4 weeks, initiate physical and occupational therapy.
OUTCOMES
Konrath and Bahler 5 reported 27 patients with at least 2 years of follow-up:One fracture lost reduction.Patient satisfaction was high (average Disabilities of the Arm, Shoulder, and Hand [DASH] scores 17 and Patient-Rated Wrist Evaluation [PRWE] scores 19 at follow-up).In only three cases was hardware removed; no tendon ruptures occurred.Schnall et al 10 reported on two groups of patients: group I had sustained high-energy trauma and group II had lower energy injuries.Group I patients averaged return to work in 6 weeks, with all fractures uniting without loss of position or deformity.Two patients in group I required removal of painful hardware.Group II patients averaged 2 degrees of loss of volar tilt, a 0.3-mm change in ulnar variance, and no loss of joint congruity at follow-up.Grip strength in group II patients was 67% of the contralateral side.Benson et al 3 reported on 85 intra-articular fractures in 81 patients with a mean follow-up of 32 months.There were 64 excellent and 24 good results, with an average DASH score of 9 at final follow-up. Flexion and extension motion was 85% and 91% of the opposite side at final follow-up.Grip strength was 92% of the opposite side at final follow-up.Sixty-two percent of patients had a 100-degree arc of flexion-extension and normal forearm rotation by 6 weeks postoperatively.Postoperative radiographic alignment was maintained at follow-up. There were no cases of symptomatic arthritis.Abramo et al 1 reported a randomized, prospective study on 50 unstable fractures too unstable for closed methods of management, with fractures randomized to either external fixation or fragment-specific fixation and with follow-up at 1 year1 and 5 years.6At 1 year, internal fixation resulted in better grip strength and range of motion. No difference in subjective outcome was observed at 5 years.There were five malunions in the external fixation group, compared to only one malunion in the fragment-specific group.Differences in grip strength tended to equalize at 5-year follow-up.Saw et al 9 reported on 22 unstable C2 and C3 fractures of the distal radius treated with fragment-specific fixation with a minimum of 6 months follow-up.At follow-up, radial inclination was restored to an average of 25 degrees and volar tilt to 8 degrees. Twenty of 22 fractures had restoration of articular congruity to less than 2 mm.Mean flexion/extension was 50 to 63 degrees, and mean pronation/supination arc of 149 degrees. Mean subjective PRWE score at follow-up was 20.Treatment approach was felt to be a powerful tool for difficult fractures, but acknowledge a significant learning curve.
COMPLICATIONS
Stiffness: common early, uncommon at follow-upRecovery can be accelerated by anatomic fixation that is stable enough to start motion immediately after surgery. The relative degree of trauma to the bone and soft tissues, combined with underlying physiologic factors, is also a critical factor that can lead to slow recovery of motion or residual stiffness.Malunion or nonunion: rareLoss of reduction may occur, particularly if a major fracture component is missed and left untreated. In addition, osteoporosis, failure to graft the metaphyseal defect, and associated DRUJ injuries may contribute to loss of reduction or malunion.Pin plates are able to resist translational displacements but are less effective for preventing loss of length; they require osseous contact between the proximal and distal fragments or additional support by bone graft or a secondary implant that will buttress the subchondral surface.Nonunions are extremely rare.Tendinitis or tendon rupture: uncommonIf pins are noted postoperatively to back out, they should be removed. Leaving the distal 1 cm of tendon sheath of the first dorsal compartment intact helps avoid tendon contact with hardware.Using low-profile implants dorsally, covering the distal ends with a strip of retinacular sheath or both is also helpful.The surgeon should avoid leaving screws or pins protruding from the dorsal or volar surfaces of the bone.Painful hardware: rarePainful hardware can be related to migration of a pin or settling of the fracture proximally. Overbending pin hooks and using bone graft or buttressing implants can help avoid this problem.Remove hardware when painful.Late arthritis is uncommon and related to the articular damage at the time of injury as well as the quality of the articular restoration.Infections, bleeding, carpal tunnel syndrome, and other nerve injuries are uncommon and often related to the primary injury.Complex regional pain syndrome is uncommon.
REFERENCES
P.2921.Abramo A, Kopylov P, Geijer M, et al. Open reduction and internal fixation compared to closed reduction and external fixation in distal radial fractures. Acta Orthop 2009;80(4):478-485.2.Barrie K, Wolfe S. Internal fixation for intraarticular distal radius fractures. Tech Hand Up Extrem Surg 2002;6:10-20.3.Benson LS, Minihane KP, Stern LD, et al. The outcome of intraarticular distal radius fractures treated with fragment-specific fixation. J Hand Surg Am 2006;31(8):1333-1339.4.Fernandez DL, Jupiter JB. Fractures of the Distal Radius, ed 2. New York: Springer, 2002:42-50.5.Konrath G, Bahler S. Open reduction and internal fixation of unstable distal radius fractures: results using the trimed fixation system. J Orthop Trauma 2002;16:578-585.6.Landgren M, Jerrhag D, Tägil M, et al. External or internal fixation in the treatment of non-reducible distal radial fractures? Acta Orthop 2011;82(5):610-613.7.Leslie BM, Medoff RJ. Fracture-specific fixation of distal radius fractures. Tech Orthop 2000;15:336-352.8.Medoff R. Essential radiographic evaluation for distal radius fractures. Hand Clin 2005;21:279-288.9.Saw N, Roberts C, Cutbush K, et al. Early experience with the TriMed fragment-specific fracture fixation system in intraarticular distal radius fractures. J Hand Surg Eur Vol 2008;33(1):53-58.10.Schnall SB, Kim BJ, Abramo A, et al. Fixation of distal radius fractures using a fragment specific system. Clin Orthop Relat Res 2006;445:51-57.11.Swigart C, Wolfe S. Limited incision open techniques for distal radius fracture management. Orthop Clin North Am 2001;32:317-327.
