FRACTURES OF THE PROXIMAL ULNA
Open Reduction and Internal Fixation of Fractures of the Proximal Ulna
DEFINITION
Fracture of the olecranon process is common, usually displaced, and nearly always treated operatively. Important injury characteristics include displacement, comminution, and subluxation or dislocation of the elbow, and all are accounted for in the Mayo classification ( FIG 1).6Fracture-dislocations of the olecranon can be anterior (transolecranon) or posterior (the most proximal type of posterior Monteggia according to Jupiter and colleagues 3) in direction.2,3,9,10The eponym Monteggia is best applied to metaphyseal or diaphyseal proximal ulnar fracture associated with dislocation of the proximal radioulnar joint.The Bado classification of Monteggia lesions with Jupiter subclassification of type II fractures is shown in Table 1.Equivalent injuries in adultsVariable pathology that is felt to be equivalent to injuries classified by the Bado systemEquivalent injuries do not always fall within the traditional definition of a Monteggia fracture in that they do not always have a concomitant radiocapitellar dislocation. Therefore, it can be argued that these injuries are not necessarily equivalent to Monteggia fractures.Type I and type II injuries are the only ones that have equivalent injury patterns.
ANATOMY
The greater sigmoid notch of the ulna is formed by the coronoid and olecranon processes and forms a nearly 180-degree arc capturing the trochlea.The region between the coronoid and olecranon articular facets is the nonarticular transverse groove of the olecranon, a common location of fracture and a place where precise articular reduction is not critical.The triceps has a broad and thick insertion from just superior to the point of the olecranon and the tip of the olecranon process that can be used to enhance fixation of small, osteoporotic, or fragmented fractures and can be split longitudinally, if needed, when applying a plate.The radioulnar articulation is stabilized by the triangular fibrocartilage complex (TFCC) at the distal radioulnar joint, the interosseous ligament in the midforearm, and the annular ligament at the proximal radioulnar joint (PRUJ). Fracture of the ulna with dislocation of the PRUJ disrupts the annular ligament, but typically, the other structures are spared.In a true Monteggia lesion (fracture-dislocation) of the forearm, the radial head dislocates anterolaterally from the PRUJ.
PATHOGENESIS
Fractures of the olecranon and proximal ulna can result from a direct blow to the point of the elbow or indirect forces during a fall on the outstretched hand.
NATURAL HISTORY
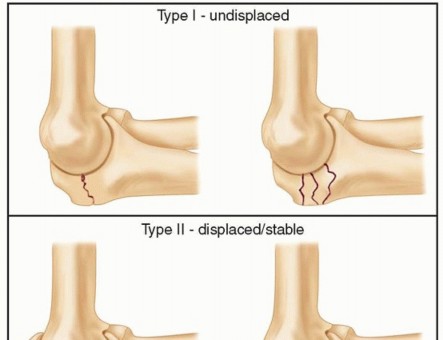
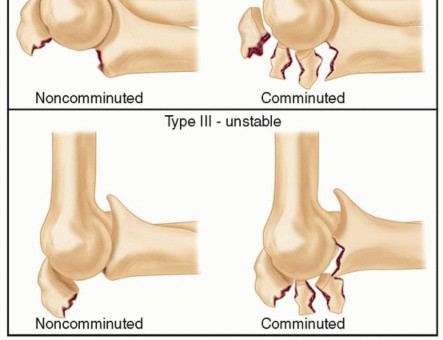
FIG 1 • The Mayo classification of olecranon fractures accounts for the factors that will influence treatment decisions: displacement, comminution, and dislocation or subluxation of the articulations. P.186 P.187 Table 1 Bado Classification of Monteggia Lesions with Jupiter Subclassification of Type II Fractures







In contrast, undertreated or poorly treated fracture-dislocations of the olecranon often lead to severe arthrosis and angulation of the arm under the influence of gravity.Even well-treated complex injuries are at risk for stiffness, heterotopic ossification, arthrosis, and occasionally nonunion.
PATIENT HISTORY AND PHYSICAL FINDINGS
Knowledge of the characteristics of the patient (age, sex, medical health) and the injury (mechanism, energy) will help the surgeon understand the injury and determine optimal treatment.First, the patient is assessed for life-threatening injuries (Advanced Trauma Life Support [ATLS] protocol) and any medical problems that may have contributed to the injury.A secondary survey is performed to identify any other fractures, ipsilateral arm injuries in particular. The skin is inspected for any wounds associated with the fracture.The pulses are palpated, capillary refill inspected, and an Allen test performed if necessary. Peripheral nerve function is assessed.Patients with high-energy injuries, particularly those with ipsilateral wrist or forearm injuries, are at risk for compartment syndrome. If the clinical examination is suggestive or unreliable (owing to problems with mental status), compartment pressure monitoring should be performed.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Anteroposterior (AP) and lateral radiographs are used for initial characterization of the injury. Radiographs after reduction or splinting or oblique views can be useful.Computed tomography (CT) is useful for characterization of fracture-dislocations. In particular, three-dimensional (3-D) CT reconstructions can be useful for assessment of the coronoid and radial head.
DIFFERENTIAL DIAGNOSIS
Elbow dislocationEssex-Lopresti fracture-dislocation of the forearm (disruption of the interosseous ligament and or TFCC usually with fracture of the radial head)Fracture-dislocations of the elbow (“terrible triad” injury) Distal humerus fracture
NONOPERATIVE MANAGEMENT
Nonoperative management is appropriate for the rare fracture of the olecranon that is less than 2 mm displaced with the elbow flexed 90 degrees.Four weeks of splint immobilization followed by active-assisted mobilization of the elbow will usually result in a healed fracture and good elbow function.
SURGICAL MANAGEMENT
The vast majority of olecranon fractures are displaced and merit operative treatment.Transverse, noncomminuted fractures not associated with fracture-dislocation are treated with tension band wiring. 4,8Comminuted fractures and fracture-dislocations are treated with dorsal contoured plate and screw fixation. 1,2,3The treatment of fracture-dislocations requires attention to the coronoid, radial head, and lateral collateral ligament. 2,9,10,11Fracture-dislocations of the forearm (anterolateral Monteggia injuries) is treated with anatomic realignment ofthe ulna and plate and screw fixation. 10 Inadequate radiocapitellar alignment suggests residual ulnar angulation.
PREOPERATIVE PLANNING
The fracture characteristics that determine treatment are defined on radiographs and CT.Templating the surgery with tracings of the radiographs is a useful way of running through the surgery in detail beforeP.188performing it, familiarizing oneself with the anatomy, anticipating problems, and ensuring that all of the implants and equipment that might be necessary are available.
POSITIONING
In most patients, a lateral decubitus position with the arm over a bolster or support is best.Some patients with fracture-dislocations that require both medial and lateral access may be positioned supine with the arm supported on a hand table.A sterile pneumatic tourniquet is used.
APPROACH
A dorsal longitudinal skin incision is used.
TECHNIQUES
Tension Band Wiring
TENSION BAND WIRING
REDUCTION AND KIRSCHNER WIRE FIXATION
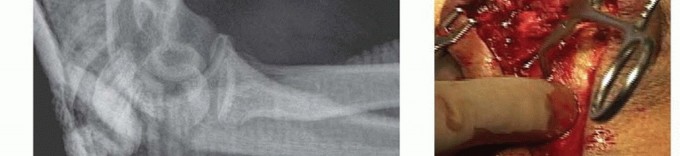
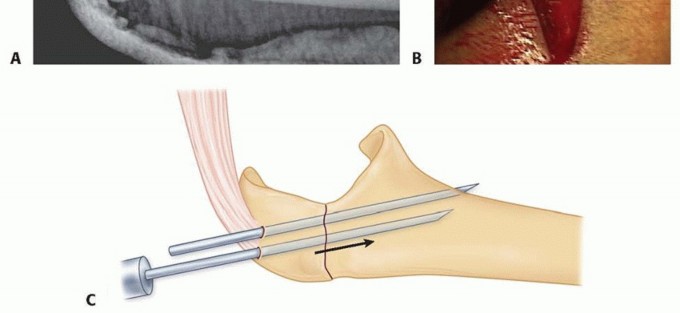
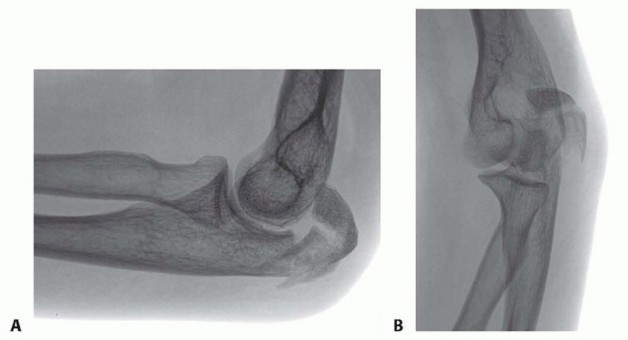
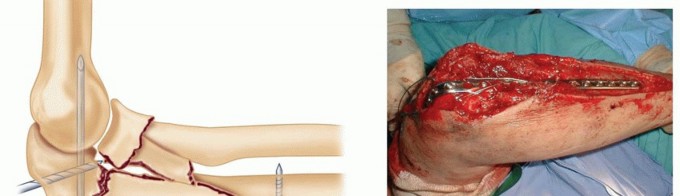
TECH FIG 1 • A. A lateral radiograph with the arm in plaster shows a transverse, noncomminuted fracture of the olecranon. B. An open reduction is held with a fracture reduction forceps. C. Two 1-mm Kirschner wires are drilled obliquely across the fracture site so that they exit the anterior ulnar cortex distal to the coronoid process. (A,B: Copyright , MD.)
WIRING
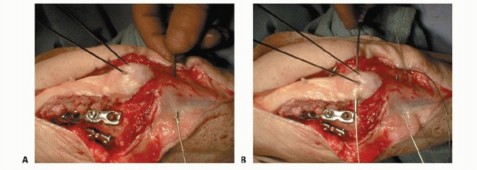
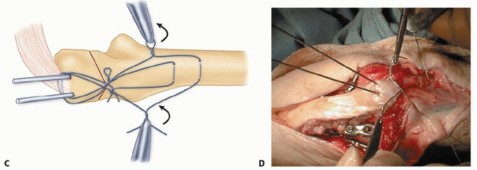
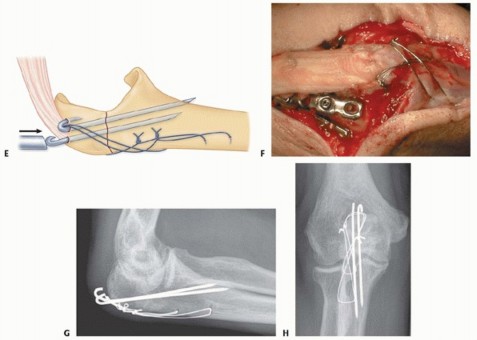
TECH FIG 2 • A. Two 22-gauge stainless steel tension wires are passed in a figure-of-eight fashion through drill holes in the ulnar shaft. B. They engage the triceps insertion proximally. C,D. The wires are
TECH FIG 3 • A. A lateral radiograph illustrates a comminuted olecranon fracture with a small proximal olecranon fragment. B. An oblique view shows the fragmentation. C. A 3.5-mm limited-contact dynamic compression plate and screws contoured to wrap around the dorsal surface of the olecranon is used for fixation. D. A 22-gauge stainless steel wire engages the triceps insertion— this is useful when the olecranon fragment is small, fragmented, or osteopenic. (Copyright , MD.) Distally, a dorsal plate will lie directly on the apex of the ulnar diaphysis. The muscle need only be split sufficiently to gain access to this apex—there is no need to elevate the muscle or periosteum off either the medial or lateral flat aspect of the ulna.No attempt is made to precisely realign intervening fragmentation— once the relationship of the coronoid and olecranon facets is restored and the overall alignment is restored, the remaining fragments are bridged, leaving their soft tissue attachments intact.Bone grafts are rarely necessary if the soft tissue attachments are preserved.If the olecranon fragment is small, osteoporotic, or fragmented, a wire engaging the triceps insertion should be used to reinforce the fixation ( TECH FIG 3D).The plate and screws will serve to hold the coronoid and olecranon facets in proper alignment and bridge fragmentation, and the wire will help ensure fixation even if screw purchase is lost.P.1913. Plate and Screw Fixation of the Fracture-Dislocations of the Olecranon
EXPOSURE
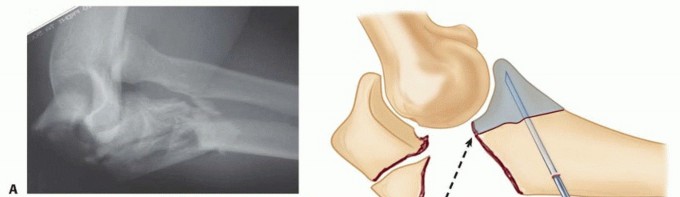
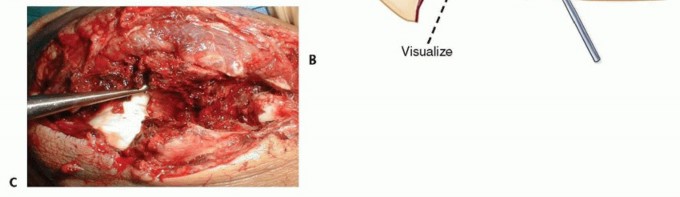
TECH FIG 4 • A. A complex anterior fracture-dislocation of the elbow. A lateral radiograph shows extensive comminution of the trochlear notch of the ulna, including the coronoid, and anterior displacement of the forearm. B,C. The coronoid fragments are connected to the dorsal metaphyseal fragments in this patient, which facilitates reduction and fixation. (A,C: Copyright , MD.)
FIXATION
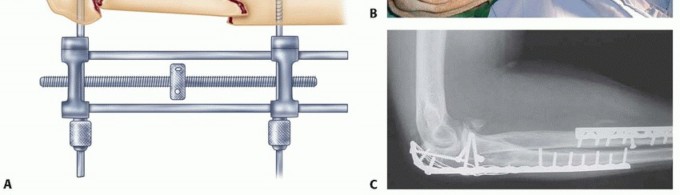
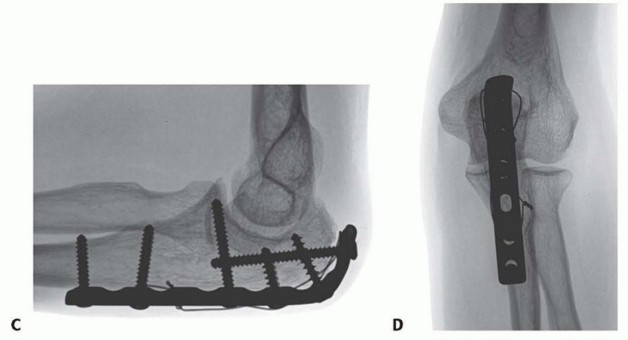
TECH FIG 5 • A. When there is diaphyseal comminution, a temporary external fixator may be useful. B. A long, 3.5-mm limited contact dynamic compression plate is used for fixation. A 22-gauge stainless steel wire is used to enhance fixation of the comminuted olecranon fragments. C. The comminution extending into the diaphysis heals with the bridging plate. The trochlear notch is restored with good elbow function. (B,C: Copyright , MD.)
Anterolateral Monteggia Fractures
ANTEROLATERAL MONTEGGIA FRACTURES
EXPOSURE
The ulna is exposed through a dorsal incision elevating the muscle from one side of the ulnar diaphysis, leaving the periosteum intact and disrupting the muscle on the opposite side as little as possible ( TECH FIG 6).Exposure of the radiocapitellar and PRUJs should rarely be necessary. Inadequate radiocapitellar/PRUJ alignment is nearly always due to residual malunion of the ulna. If necessary, expose the joint as for a radial head fracture.
FIXATION
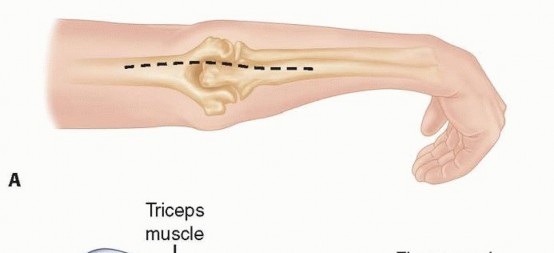
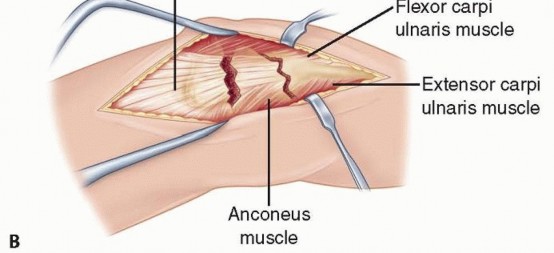
TECH FIG 6 • A. Posterior midline incision positioned just off the lateral aspect of the olecranon. B. Deep surgical interval uses the internervous plane between the anconeus and flexor carpi ulnaris.

TECH FIG 7 • Malunion of the ulna with resulting apex dorsal angulation results in dislocation of the radial head.
PEARLS AND PITFALLS
Prominence ▪ The use of two small (22-gauge) wires rather than one large one will result inof olecranon smaller knots. Care taken to place the Kirschner wires below the triceps insertion hardware and impacting them into bone will limit prominence and the potential formigration. 5,8Narrowingof trochlear notch1.The surgeon should not use a tension wire alone on a comminuted fracture. Anintact articular surface to absorb compressive forces with active motion is mandatory for tension band wiring to be effective.Plateloosening1.The surgeon should use a dorsal plate contoured to wrap around the olecranon,providing a greater number of screws and screws at different, nearly orthogonalangles. Use of a medial or lateral plate should be avoided. 10,11Loss offixation of the proximal (olecranon) fragment1.Screw fixation alone should not be trusted if the fragment is small, fragmented, orosteoporotic. A tension wire engaging the triceps insertion should be added.Failure torecognize a complex injury1.The surgeon should be vigilant for subluxation or dislocation of the elbow,fracture of the coronoid or radial head, and injury to the lateral collateral ligament. When identified, each injury is treated accordingly. The olecranon and proximal ulna are always secured with a plate and screws.
POSTOPERATIVE CARE
When good fixation is obtained (which occurs in most patients), active-assisted and gravity-assisted elbow and forearm exercises can be initiated immediately after surgery. A delay of several days for comfort is reasonable.If the lateral collateral ligament was repaired, the patient must be instructed not to abduct the shoulder for the first month, as this imparts a varus moment across the elbow and stresses the ligament repair.If the fixation is tenuous, it is reasonable to immobilize the arm in a splint for a month or so before beginning exercises.
OUTCOMES
Nonunion is nearly unheard of after simple olecranon fractures, and early implant failure is usually due to non-compliance. 6The appeal of tension band wiring has been limited by prominence of the implants; however, if thetechniques described herein are followed, few patients will request a second surgery specifically forimplant removal. 8Macko and Szabo 5 pointed out that it was initial implant prominence and not migration that led to implant-related problems after tension band wiring of olecranon fractures.In any case, a second surgery for implant removal is not unreasonable and it may not be appropriate to consider this a complication.Some surgeons have considered plate-and-screw fixation of simple, noncomminuted olecranonfractures. 1 However, plates can also cause symptoms, and if only a few screws can be placed in the olecranon fragment, particularly in the setting of fragmentation or osteoporosis, it may be preferable to use the soft tissue attachments to enhance fixation rather than relying on implant-bone purchase alone.Medial and lateral plates have been associated with early failure, malunion, and nonunion in the treatment of complex proximal ulnar fractures. 10,11Dorsal plates perform better, but the elbow is often compromised in the setting of such complex injuries.P.194
COMPLICATIONS
Implant loosening Implant breakage Nonunion Malunion Instability Arthrosis
REFERENCES
- Bailey CS, MacDermid J, Patterson SD, et al. Outcome of plate fixation of olecranon fractures. J Orthop Trauma 2001;15: 542-548.
- Doornberg J, Ring D, Jupiter JB. Effective treatment of fracture-dislocations of the olecranon requires a stable trochlear notch. Clin Orthop Relat Res 2004;(429):292-300.
- Jupiter JB, Leibovic SJ, Ribbans W, et al. The posterior Monteggia lesion. J Orthop Trauma 1991;5:395-402.
- Karlsson M, Hasserius R, Besjakov J, et al. Comparison of tension-band and figure-of-eight wiring techniques for treatment of olecranon fractures. J Shoulder Elbow Surg 2002;11:377-382.
- Macko D, Szabo RM. Complications of tension-band wiring of olecranon fractures. J Bone Joint Surg Am 1985;67(9):1396-1401.
- Morrey BF. Current concepts in the treatment of fractures of the radial head, the olecranon, and the coronoid. J Bone Joint Surg Am 1995;77A:316-327.
- O'Driscoll SW, Jupiter JB, Cohen M, et al. Difficult elbow fractures: pearls and pitfalls. Instruct Course Lect 2003;52:113-134.
- Ring D, Gulotta L, Chin K, et al. Olecranon osteotomy for exposure of fractures and nonunions of the distal humerus. J Orthop Trauma 2004;18:446-449.
- Ring D, Jupiter JB, Sanders RW, et al. Transolecranon fracture-dislocation of the elbow. J Orthop Trauma 1997;11:545-550.
- Ring D, Jupiter JB, Simpson NS. Monteggia fractures in adults. J Bone Joint Surg Am 1998;80(12):1733-1744.
- Ring D, Tavakolian J, Kloen P, et al. Loss of alignment after surgical treatment of posterior Monteggia fractures: salvage with dorsal contoured plating. J Hand Surg Am 2004;29(4):694-702.
