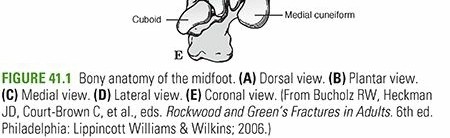
Comprehensive Introduction and Patho-Epidemiology
Injuries to the midfoot and forefoot, particularly those involving the midtarsal (Chopart) joint complex, represent a highly complex and challenging subset of orthopedic trauma. While relatively rare in isolation, these injuries carry a profound potential for long-term morbidity if misdiagnosed or inadequately managed. The annual incidence of midfoot fractures is approximately 3.6 per 100,000 population per year, reflecting their relative scarcity compared to ankle or forefoot metatarsal fractures. Among these, the most commonly fractured bone is the cuboid, accounting for 50% of midfoot fractures, followed closely by the navicular at 44%, and the cuneiforms making up the remaining 6%. The demographic distribution demonstrates a slight male predominance, with a male-to-female ratio of 1:1.2, often correlating with occupational hazards and high-impact athletic participation.

The pathophysiology of these injuries is broadly divided into high-energy and low-energy mechanisms, each presenting with distinct clinical profiles and fracture morphologies. High-energy trauma is the most common etiology for severe, displaced fractures and fracture-dislocations. These typically result from direct impact, such as in motor vehicle collisions, or from a complex combination of axial loading and torsional forces experienced during a fall or jump from a significant height. In these scenarios, the energy imparted to the foot overwhelms the robust ligamentous restraints, leading to catastrophic failure of the bony architecture and surrounding soft tissue envelope. The "nutcracker" mechanism, where the cuboid is crushed between the calcaneus and the metatarsal bases during forced forefoot abduction, is a classic example of such high-energy force transmission.

Conversely, low-energy injuries frequently manifest as sprains or subtle avulsion fractures and are commonly seen in athletic or dance activities. These injuries occur when the foot is subjected to sudden, forceful inversion, eversion, or plantarflexion beyond its physiological range of motion. While the bony disruption may appear minimal on initial imaging, the true extent of the injury often lies in the disruption of the critical ligamentous stabilizers of the Chopart joint. Furthermore, repetitive low-energy cyclic loading can lead to stress fractures, particularly in the tarsal navicular of young, competitive athletes. These stress injuries are exacerbated by underlying biomechanical abnormalities, such as a rigid cavus foot architecture or an undiagnosed calcaneonavicular coalition, which abnormally concentrate forces across the midfoot.

Isolated fractures of the tarsal navicular are exceedingly rare and must be approached with a high index of suspicion for concomitant injuries. The diagnosis of an isolated navicular fracture should only be accepted after an exhaustive clinical and radiographic evaluation has definitively ruled out subtle subluxations or ligamentous disruptions within the broader midtarsal joint complex. The interconnected nature of the midfoot dictates that an injury to one component inevitably alters the biomechanical loading of the adjacent structures. Therefore, the orthopedic surgeon must view these fractures not as isolated osseous defects, but as disruptions of a highly synchronized, multi-articular functional unit.

Detailed Surgical Anatomy and Biomechanics
The midfoot is anatomically defined as the section of the foot situated distal to the Chopart joint line (talonavicular and calcaneocuboid joints) and proximal to the Lisfranc joint line (tarsometatarsal joints). This region is comprised of five distinct tarsal bones: the navicular, the cuboid, and the medial, middle, and lateral cuneiforms. The midtarsal (Chopart) joint acts as a critical biomechanical transition zone, functioning in concert with the subtalar joint to facilitate complex inversion and eversion of the foot. This synchronized motion is essential for accommodating uneven terrain during the stance phase of gait and for transitioning the foot from a flexible shock absorber at heel strike to a rigid lever arm during toe-off.

The navicular serves as the structural keystone of the medial longitudinal arch. Morphologically, it is wider on its dorsal and medial aspects than on its plantar and lateral surfaces, a wedge-like shape that contributes to the intrinsic stability of the arch. The medial prominence, known as the navicular tuberosity, is a critical landmark as it provides the primary attachment point for the posterior tibialis tendon on its medial inferior surface. Proximally, the navicular's articular surface is deeply concave, articulating with the convex head of the talus. This talonavicular joint enjoys a significant arc of motion and is responsible for transmitting the complex, multi-planar motion of the subtalar joint to the forefoot; it is the precise point from which forefoot inversion and eversion are initiated.

Distally, the articular surface of the navicular is divided into three separate, broad facets that articulate with the three cuneiforms. Unlike the highly mobile talonavicular joint, these naviculocuneiform joints permit very little motion, functioning primarily to dissipate and distribute axial loading stresses into the forefoot rays. Laterally, the navicular rests on the dorsal medial aspect of the cuboid, sharing a variable articular surface. The cuboid itself acts as a vital linkage across the lateral column and the three naviculocuneiform joints, allowing only minimal motion while providing essential lateral column stability.

The osseous stability of the midfoot is massively augmented by a complex network of stout ligaments. Key ligamentous attachments include the plantar calcaneonavicular (spring) ligament, which supports the talar head; the bifurcate ligament (calcaneonavicular and calcaneocuboid bands); the dorsal talonavicular ligament; the dorsal calcaneocuboid ligament; the dorsal cuboideonavicular ligament; and the expansive long plantar ligament. The superficial deltoid also provides strong support to the medial aspect of the talonavicular joint. Surgeons must also be acutely aware of anatomic variants, most notably the presence of an accessory navicular (os tibiale externum). Present in 4% to 15% of the population and bilateral in 70% to 90% of those cases, this variant can alter the insertion of the posterior tibialis and must not be misidentified as an acute avulsion fracture during trauma evaluation.

Exhaustive Indications and Contraindications
The management of midfoot and forefoot fractures is dictated by the precise fracture morphology, the degree of articular displacement, and the overall stability of the medial and lateral columns. The overarching goal of any intervention is the anatomic restoration of the talonavicular and calcaneocuboid joint surfaces and the maintenance of absolute column length. Because the talonavicular joint is highly congruent and concave, even a 2-mm separation or step-off in any plane is considered incongruent and will lead to rapid, debilitating posttraumatic osteoarthritis. Most academic authors and trauma specialists agree that these injuries must be managed aggressively with operative reduction and rigid internal fixation.

Indications for nonoperative management are strictly limited to truly nondisplaced fractures, stable sprains, and minor cortical avulsions that do not compromise joint stability. Nondisplaced fractures of the navicular or cuboid may be treated with a short leg cast or a rigid fracture brace, requiring strict initial non–weight-bearing for 6 to 8 weeks. Cortical avulsion fractures (which account for up to 50% of navicular injuries) caused by excessive flexion or eversion can be treated nonoperatively if the fragment is small and nonarticular. However, if the avulsed fragment involves greater than 25% of the articular surface, or if it represents a significant portion of the dorsal anterior surface, operative reattachment with lag screw fixation is strongly indicated to prevent chronic instability.

Operative indications encompass any unstable injury, fractures resulting in loss of column length, or articular incongruity exceeding 2 mm. High-energy mechanisms resulting in displaced fracture patterns (such as Type II and Type III Sangeorzan navicular body fractures) require Open Reduction and Internal Fixation (ORIF). Tuberosity fractures caused by forced eversion—often part of a "nutcracker" injury—require ORIF with lag screw fixation if the fragment is large or if the function of the posterior tibial tendon is compromised. Furthermore, stress fractures in young athletes that exhibit a complete sagittal fracture line, comminution, or delayed healing are absolute indications for surgical intervention, typically involving screw fixation combined with autologous bone grafting.
| Clinical Scenario | Operative Indication | Nonoperative Indication / Contraindication to Surgery |
|---|---|---|
| Navicular Body Fracture | Displacement > 2mm, articular step-off, medial column shortening. | Strictly nondisplaced fractures (confirmed on CT); severe non-ambulatory baseline. |
| Cortical Avulsion | Fragment > 25% of articular surface; significant instability. | Small, nonarticular fragments; isolated sprains. |
| Tuberosity Fracture | Large fragment with compromised posterior tibial tendon function. | Small, minimally displaced fragments; asymptomatic accessory navicular. |
| Cuboid "Nutcracker" | Lateral column shortening, significant articular comminution. | Nondisplaced; severe active foot infection (absolute contraindication). |
| Stress Fracture | Comminuted, complete sagittal line, failed conservative therapy. | Incomplete fracture line without sclerosis, compliant patient. |
Contraindications to operative intervention include severe, life-threatening polytrauma where the patient is unstable for prolonged extremity surgery. Local factors such as severe soft tissue compromise, active blistering, or gross infection over the surgical site necessitate delaying definitive internal fixation, often requiring temporary stabilization with external fixation. Additionally, extreme cases of peripheral neuropathy (e.g., severe Charcot arthropathy) or severe peripheral vascular disease may preclude standard ORIF, pushing the surgeon toward conservative management or primary salvage procedures.

Pre-Operative Planning, Templating, and Patient Positioning
Thorough clinical and radiographic evaluation is the cornerstone of successful pre-operative planning. Patient presentation is highly variable, ranging from a mild limp with localized swelling and tenderness on the dorsum of the midfoot to a completely nonambulatory status accompanied by significant pain, gross swelling, massive ecchymosis, and variable structural deformity. Plantar ecchymosis is a classic hallmark and is usually indicative of a severe midfoot or Lisfranc-type injury. A meticulous neurovascular examination must be performed and documented upon presentation. In cases of extreme pain out of proportion to the injury and tense swelling, serial examinations are absolutely warranted to evaluate the possibility of foot compartment syndrome, a devastating complication if missed.

Standard radiographic evaluation mandates Anteroposterior (AP), lateral, and oblique radiographs of the foot. If the patient's pain tolerance permits, stress views or weight-bearing x-rays are invaluable for delineating subtle ligamentous injuries and dynamic instabilities. Medial and lateral oblique x-rays of the midfoot specifically aid in assessing the lateral pole of the navicular as well as the medial tuberosity. Furthermore, stress maneuvers performed under fluoroscopy—consisting of forefoot abduction, adduction, flexion, and extension—can reproduce pain and unmask latent instability that is not apparent on static, non-weight-bearing films.

In the modern era of orthopedic trauma, Computed Tomography (CT) is considered mandatory for any suspected midfoot fracture-dislocation. CT scanning with fine 1-mm cuts and 3D reconstructions provides unparalleled characterization of fracture patterns, articular comminution, and occult subluxations that plain films frequently miss. Magnetic Resonance Imaging (MRI) or technetium bone scans are reserved for evaluating isolated ligamentous injuries, chondral shear defects, or subtle stress fractures that remain radiographically occult. The classic navicular stress fracture, for instance, typically presents as a sagittally oriented line in the relatively avascular middle third of the bone, best appreciated on an MRI.

Pre-operative templating involves utilizing the CT scan to map the fracture lines and plan the trajectory of fixation. For patient positioning, the patient is placed supine on a radiolucent flat Jackson table. A bump is placed under the ipsilateral hip to internally rotate the leg, bringing the foot into a neutral, upward-facing position. A thigh tourniquet is applied to provide a bloodless surgical field. The fluoroscopy unit (C-arm) must be positioned to allow unobstructed AP, lateral, and oblique views of the midfoot without compromising the sterile field or the surgeon's working space.

Step-by-Step Surgical Approach and Fixation Technique
Surgical access to the midfoot requires precise, anatomically safe incisions to prevent devastating soft tissue necrosis and nerve injury. For the tarsal navicular, a dorsomedial approach is most commonly utilized. The incision is centered over the talonavicular joint and extended distally toward the medial cuneiform. The interval is typically developed medial to the tibialis anterior tendon, or between the tibialis anterior and the extensor hallucis longus (EHL). Meticulous care must be taken to identify and protect the branches of the superficial peroneal nerve dorsally and the saphenous nerve medially. The thick dorsal capsule is incised longitudinally to expose the articular surfaces.

Reduction maneuvers must prioritize the restoration of the articular congruity of the talonavicular joint and the absolute length of the medial column. In cases of a Type I or Type II Sangeorzan body fracture, a small femoral distractor or a mini-external fixator can be applied spanning from the talus to the medial cuneiform. This distraction unloads the joint, restores column length, and allows for direct manipulation of the articular fragments using dental picks and fine K-wires. Once anatomically reduced, provisional fixation is achieved with multiple 1.25-mm or 1.6-mm K-wires.

Definitive fixation is highly dependent on the fracture pattern. For simple split fractures (Type I or II), multiple 3.5-mm or 4.0-mm cortical lag screws, or headless compression screws, are inserted perpendicular to the fracture plane. In Type III comminuted fractures, lag screw fixation alone is often insufficient. These injuries frequently require the application of a low-profile mini-fragment locking plate applied to the dorsal or medial surface of the navicular to act as a buttress and neutralize deforming forces. Individual articular fragments may need to be "stabbed" or pinned individually, and any residual subchondral voids must be aggressively packed with cancellous bone graft, typically harvested from the ipsilateral proximal tibia or calcaneus.

For lateral column injuries, such as the "nutcracker" fracture of the cuboid, a dorsolateral approach is utilized. The incision is made over the calcaneocuboid joint, taking care to protect the sural nerve. Similar to the medial side, a distractor is placed between the calcaneus and the 4th/5th metatarsals to restore lateral column length. The crushed cuboid is disimpacted, elevating the articular surface. Because this mechanism creates a significant bony void, structural bone grafting is almost universally required following reduction. A lateral bridging plate is then applied to maintain the length and alignment while the graft incorporates. In severe crush injuries with extensive, irreparable comminution, primary arthrodesis of the affected joints may be necessary to restore the longitudinal arch of the foot and provide a stable, plantigrade limb.

Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following midfoot and Chopart joint fractures remain unfortunately common, largely due to the precarious blood supply of the tarsal bones and the unforgiving nature of the midtarsal articulations. The most frequent and debilitating complication is posttraumatic osteoarthritis. This occurs as a direct result of residual articular incongruity, initial chondral impaction injury at the time of trauma, or avascular necrosis (AVN). The navicular is particularly susceptible to AVN due to its watershed blood supply, with the central third receiving tenuous perfusion. Posttraumatic arthritis presents with chronic, activity-limiting midfoot pain, stiffness, and progressive deformity.

Malunion and nonunion are also significant concerns. Failure to restore medial column length results in a progressive planovalgus (flatfoot) deformity, characterized by forefoot abduction and hindfoot valgus. Conversely, failure to restore lateral column length in a cuboid fracture leads to a cavovarus deformity. Both scenarios drastically alter the biomechanics of gait, leading to adjacent joint arthritis and intractable pain. Nonunion of navicular stress fractures is a known entity, particularly if treated nonoperatively in an active patient, often requiring secondary intervention with structural grafting and rigid internal fixation.

Soft tissue complications are paramount in the immediate postoperative period. The thin dorsal soft tissue envelope is prone to wound dehiscence, marginal necrosis, and deep infection. Furthermore, unrecognized compartment syndrome of the foot leads to devastating ischemic contractures, resulting in rigid claw toes, intrinsic minus foot deformity, and severe neuropathic pain. Iatrogenic nerve injuries, particularly to the superficial peroneal or sural nerves, can result in painful neuromas that complicate footwear and rehabilitation.
| Complication | Estimated Incidence | Salvage Management / Treatment |
|---|---|---|
| Posttraumatic Osteoarthritis | 30 - 50% (High-energy) | Custom orthotics; Isolated Talonavicular or Triple Arthrodesis. |
| Avascular Necrosis (Navicular) | 10 - 25% | Prolonged protected weight-bearing; Core decompression; Arthrodesis. |
| Malunion (Column Shortening) | 15 - 20% | Corrective opening/closing wedge osteotomies; corrective fusions. |
| Nonunion | 5 - 10% | Revision ORIF with autogenous bone grafting and robust plating. |
| Foot Compartment Syndrome | < 5% (If monitored) | Emergent dual-incision fasciotomies; delayed closure/skin grafting. |
Salvage management for severe, debilitating posttraumatic arthritis or failed fixation typically involves arthrodesis. If the arthritis is isolated to the talonavicular joint, an isolated fusion may provide adequate relief while preserving some hindfoot motion. However, due to the coupled mechanics of the Chopart joint complex, a talonavicular fusion effectively eliminates subtalar motion. Therefore, in cases of widespread midtarsal damage or severe deformity, a formal triple arthrodesis (fusion of the subtalar, talonavicular, and calcaneocuboid joints) is often the most reliable salvage procedure to provide a painless, stable, and plantigrade foot.

Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation following midfoot fracture fixation is a prolonged and phased process, requiring strict patient compliance and close coordination with physical therapy. The prognosis is generally guarded and is heavily dependent on the degree of initial articular incongruity and the success of the anatomic reduction. The primary goal of the initial phase (Weeks 0-2) is the protection of the soft tissue envelope and the surgical repair. The patient is placed in a bulky, nonrigid sterile dressing and a posterior splint. Strict non-weight-bearing (NWB) status is enforced. Elevation above the level of the heart and aggressive edema control are critical to prevent wound breakdown.

During the subacute phase (Weeks 2-6), patients are seen in the clinic for suture removal and wound evaluation. If the incisions are fully healed, the patient is transitioned to a well-molded short leg cast or a rigid Controlled Ankle Motion (CAM) boot. Non-weight-bearing status is strictly maintained for a minimum of 6 to 8 weeks to allow for initial bony consolidation. During this period, if the fixation is deemed absolutely rigid by the operating surgeon, early gentle active range of motion (ROM) of the toes and the ankle joint may be initiated to prevent profound stiffness, although motion across the Chopart joint is inherently restricted by the boot.

The intermediate phase (Weeks 6-12) begins with a clinical and radiographic reassessment. Repeat radiographs are obtained to confirm the maintenance of reduction, absence of hardware failure, and the presence of bridging callus.
Clinical & Radiographic Imaging Archive


