Introduction to Proximal Femoral Fractures
Fractures of the proximal femur, universally referred to as hip fractures, represent one of the most common and consequential injuries managed by orthopedic surgeons. Epidemiological data indicates a rising incidence of these fractures, directly correlating with the increasing life expectancy of the global population. In the United States alone, over 280,000 hip fractures occur annually, a figure projected to double by the year 2050.
The socioeconomic and healthcare burdens of hip fractures are staggering, with estimated annual treatment costs exceeding $10 billion. More critically, these injuries are associated with profound morbidity and mortality. Approximately 30% of elderly patients succumb within one year of sustaining a hip fracture. Those who survive the initial 12 months typically return to their age-adjusted mortality baseline, underscoring the critical nature of the perioperative and immediate postoperative periods.
Bimodal Distribution and Injury Mechanisms
Hip fractures exhibit a classic bimodal distribution:
* Low-Energy Trauma (Elderly): Accounting for nearly 90% of cases, these fractures occur in patients over 65 years of age, predominantly females (3:1 ratio compared to males). The mechanism is typically a simple fall from standing height. Risk factors include osteoporosis, neurological impairment, malnutrition, impaired vision, and generalized sarcopenia.
* High-Energy Trauma (Young Adults): Occurring in patients aged 20 to 40, these fractures result from motor vehicle collisions, falls from significant heights, or other high-velocity impacts. These injuries are frequently associated with polytrauma, severe soft tissue compromise, and higher rates of complications such as nonunion and osteonecrosis.
Clinical Pearl: Despite anatomical similarities, the physiological and biomechanical differences between low-velocity osteoporotic fractures and high-velocity young adult fractures dictate entirely different treatment algorithms. High-energy injuries demand meticulous attention to associated life-threatening injuries and often require more complex, biologically preserving fixation strategies.
Diagnostic Evaluation and Imaging
The classic clinical presentation of a displaced hip fracture includes a shortened, externally rotated lower extremity with profound pain upon any attempted range of motion. However, nondisplaced or impacted fractures may present subtly, with patients occasionally able to bear weight.
Radiographic Assessment
Standard initial imaging includes an anteroposterior (AP) radiograph of the pelvis and a cross-table lateral radiograph of the affected hip. These views are usually sufficient to diagnose and classify the majority of proximal femoral fractures.
Advanced Imaging for Occult Fractures
In cases where the clinical suspicion for a hip fracture is high but plain radiographs are equivocal, advanced imaging is mandatory.

Fig. 52-1: (A) Nondisplaced intertrochanteric fracture not visible on an initial AP radiograph. (B) The same fracture clearly identified on a T1-weighted MRI, demonstrating a hypointense fracture line.
- Magnetic Resonance Imaging (MRI): T1-weighted MRI is the gold standard for occult hip fractures. Studies by Quinn and McCarthy demonstrated that MRI is 100% sensitive and specific for identifying radiographically occult fractures.
- Bone Scintigraphy: Traditionally considered unreliable within the first 48-72 hours, modern studies (Holder et al.) have shown a 93% sensitivity for bone scans regardless of the time from injury, making it a viable alternative if MRI is contraindicated.
Preoperative Optimization and Surgical Timing
The timing of surgical intervention is a critical determinant of patient survival. While elderly patients frequently present with multiple medical comorbidities requiring optimization, excessive surgical delay is detrimental.
Surgical Warning: Delaying operative fixation for more than 48 to 72 hours significantly increases mortality. Zuckerman et al. demonstrated that a delay of more than 3 days doubles the mortality rate within the first year. McGuire noted a 15% increase in immediate mortality when fixation was delayed beyond 48 hours.
Traction and Anesthesia
The routine use of preoperative Buck traction has been largely abandoned. Jerre et al. demonstrated that traction does not reduce preoperative pain or facilitate intraoperative fracture reduction. Furthermore, in femoral neck fractures, traction may compromise the tenuous blood supply to the femoral head by increasing intracapsular pressure.
Surgery may be performed under general, spinal, or epidural anesthesia. Current evidence shows no significant difference in perioperative mortality between regional and general anesthesia, though regional techniques may offer benefits in immediate postoperative pain control and reduced delirium.
Intertrochanteric Femoral Fractures
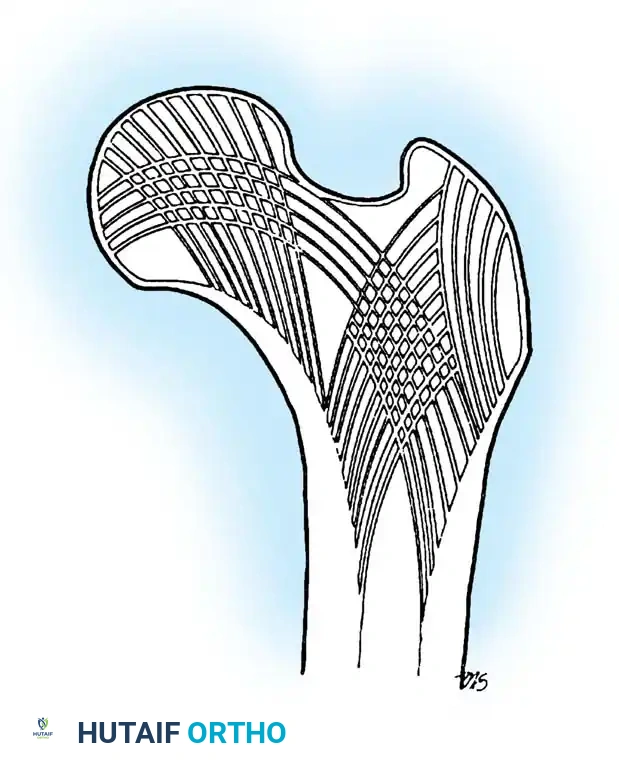
Intertrochanteric fractures occur in the highly vascularized, cancellous bone between the greater and lesser trochanters. Because this region is extracapsular, the blood supply to the femoral head is rarely compromised, making osteonecrosis a rare complication. The primary challenge in treating these fractures is mechanical rather than biological; the goal is to achieve stable fixation that resists the massive deforming forces of the hip musculature until union occurs.
Anatomical Classification Systems
Accurate classification is essential for determining fracture stability and selecting the appropriate implant.
Boyd and Griffin Classification
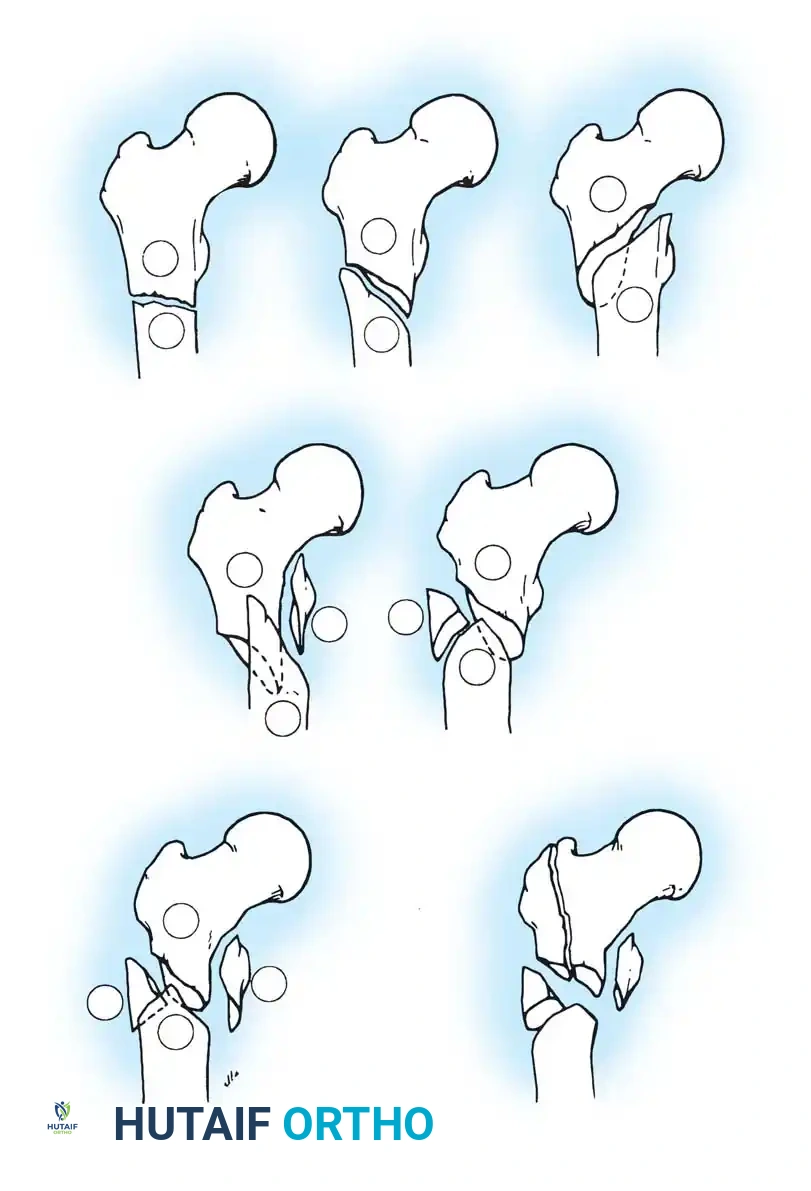
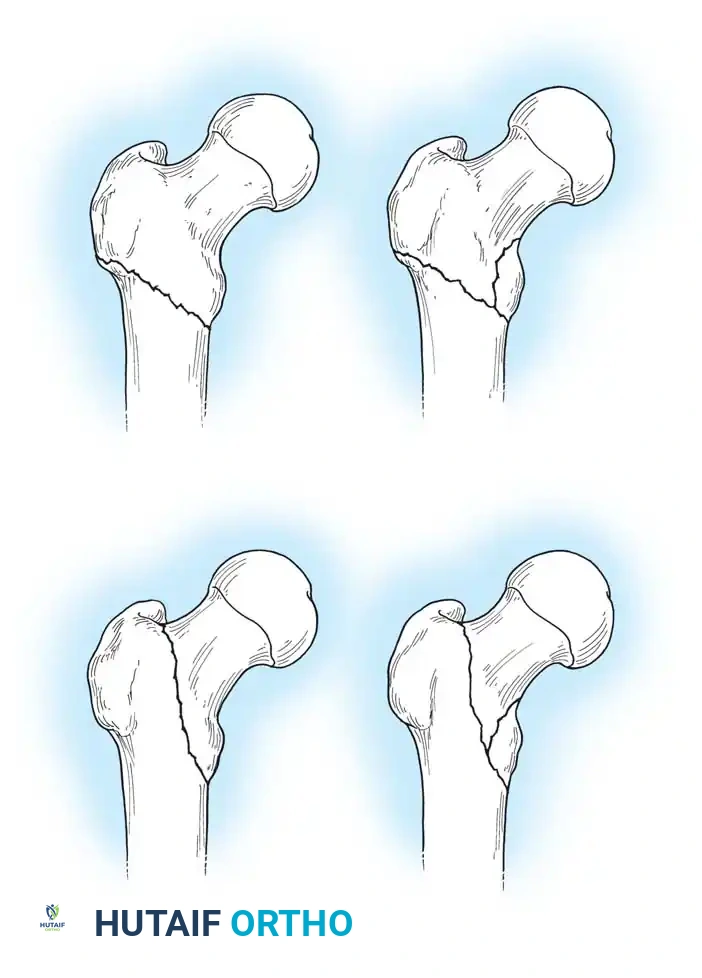
Boyd and Griffin (1949) classified peritrochanteric fractures into four types based on the ease of reduction and the presence of comminution:
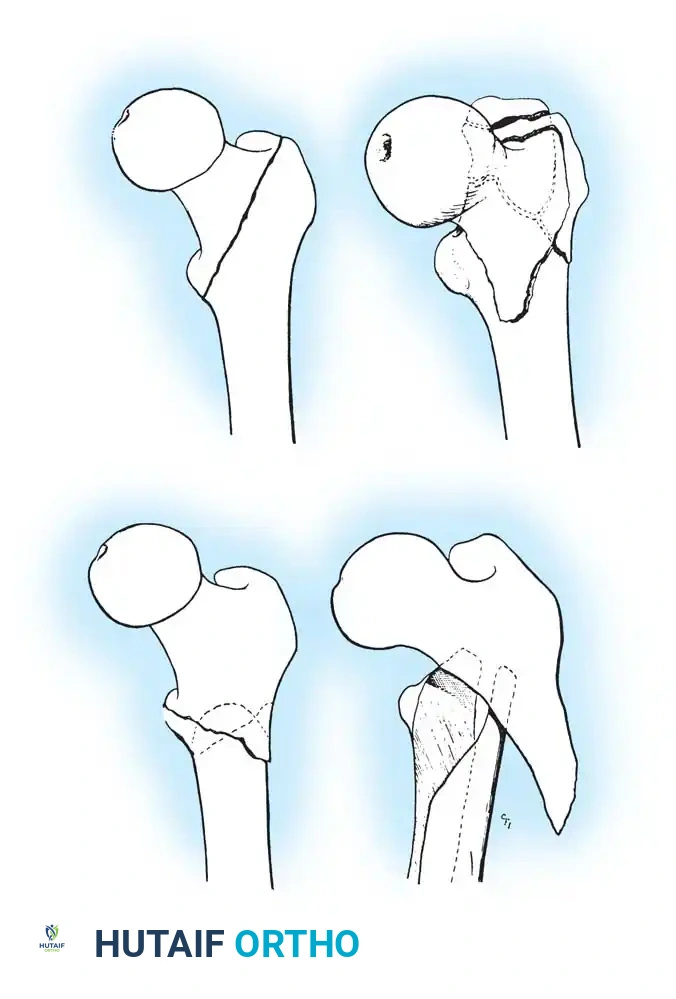
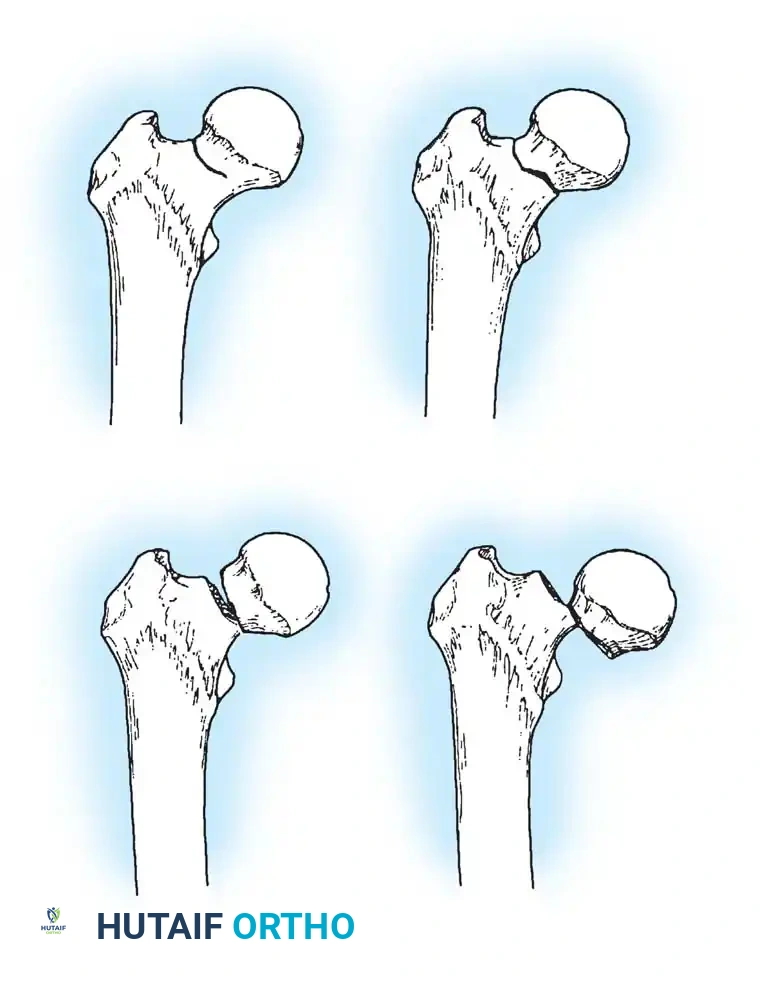
Fig. 52-2: Boyd and Griffin Classification of trochanteric fractures. Types 1 and 2 represent relatively simple patterns, while Types 3 and 4 involve subtrochanteric extension and multi-planar comminution.
- Type 1: Non-comminuted fractures extending along the intertrochanteric line. Simple to reduce and highly stable.
- Type 2: Comminuted fractures along the intertrochanteric line. Reduction is more challenging due to cortical comminution.
- Type 3: Fractures with a subtrochanteric extension. These are inherently unstable and difficult to manage.
- Type 4: Complex fractures involving the trochanteric region and proximal shaft in at least two planes (sagittal and coronal).
Evans Classification
The Evans classification divides fractures into stable and unstable patterns based on the integrity of the posteromedial cortex (the calcar femorale).
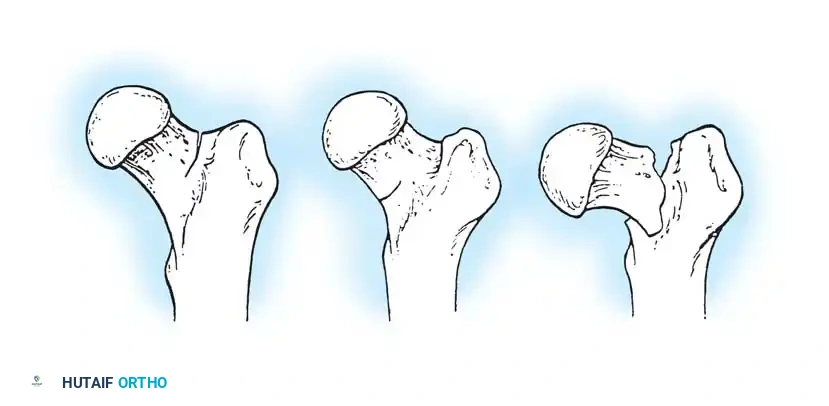
* Stable: The posteromedial cortex is intact or can be anatomically reduced.
* Unstable: Characterized by posteromedial comminution, subtrochanteric extension, or a reverse obliquity pattern (where the fracture line extends outward and downward from the lesser trochanter). Reverse obliquity fractures are highly unstable due to the medializing pull of the adductor musculature.
AO/OTA Classification
The AO/OTA system provides a comprehensive alphanumeric categorization:
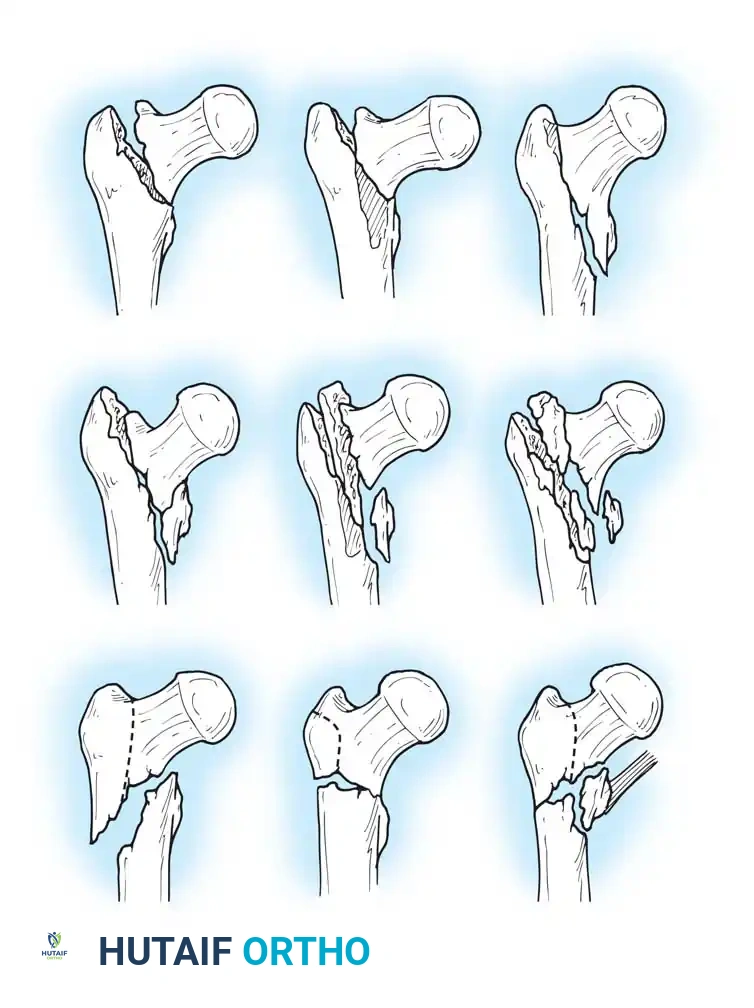
Fig. 52-4: AO Classification of trochanteric fractures. A1 (simple), A2 (comminuted), and A3 (reverse obliquity/transverse).
- 31-A1: Simple, two-part fractures (Stable).
- 31-A2: Comminuted fractures with posteromedial fragmentation (Unstable).
- 31-A3: Reverse obliquity or transverse fractures extending into the lateral cortex (Highly Unstable).
Operative Management: Principles and Biomechanics
The nonoperative treatment of displaced intertrochanteric fractures is reserved strictly for patients who are nonambulatory at baseline, have minimal pain, or possess prohibitive medical comorbidities that make anesthesia uniformly fatal. For all others, operative fixation is the standard of care.
Goals of Surgery
- Achieve a stable, anatomical or near-anatomical reduction.
- Provide rigid internal fixation to allow immediate weight-bearing.
- Restore the abductor lever arm and femoral offset.
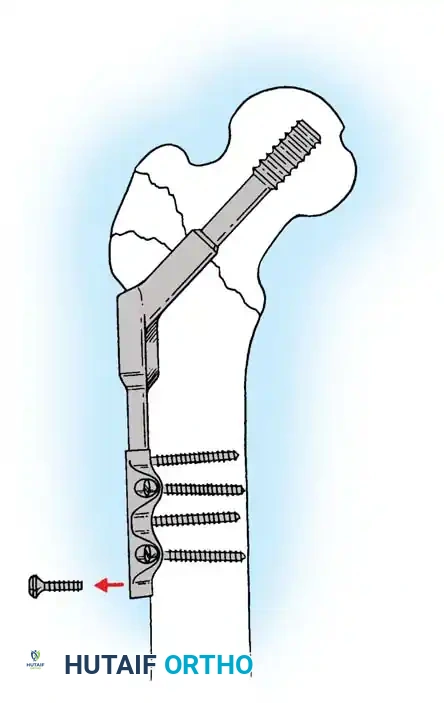
Implant Selection: SHS vs. Cephalomedullary Nail
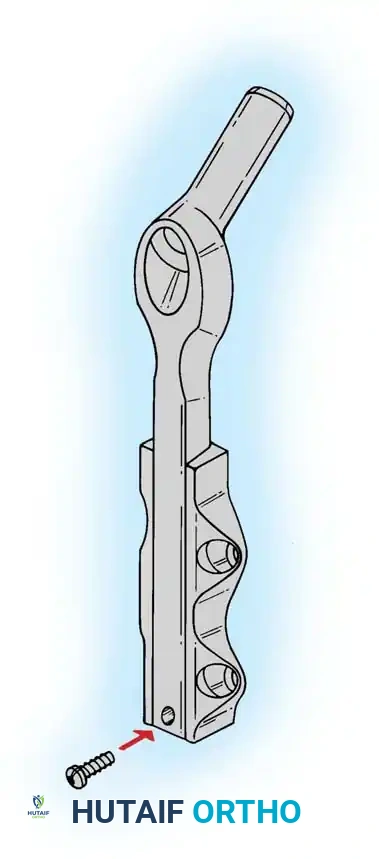
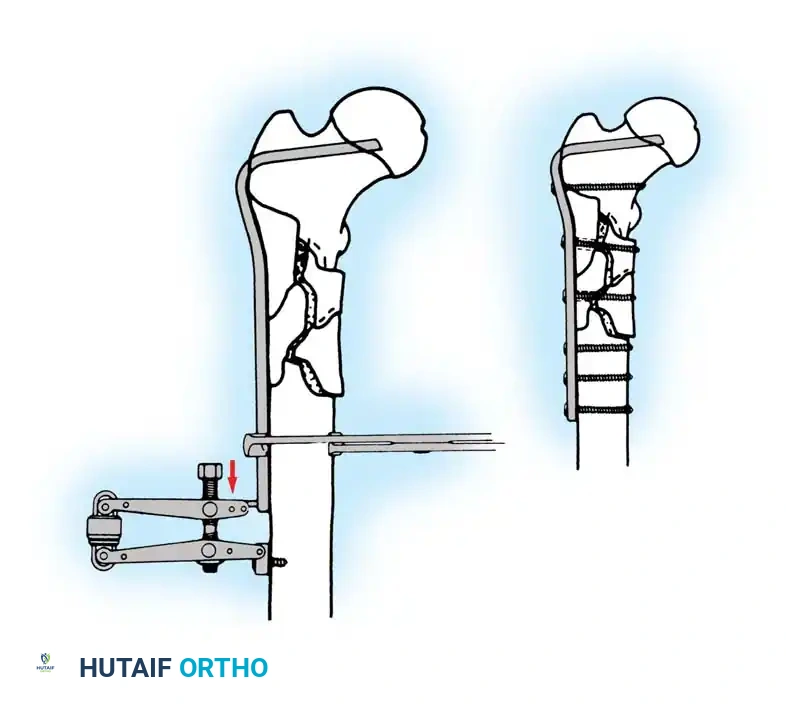
- Sliding Hip Screw (SHS): The gold standard for stable intertrochanteric fractures (Evans Type I, AO 31-A1). The SHS allows controlled dynamic collapse along the axis of the femoral neck, compressing the fracture site and promoting primary bone healing.
- Cephalomedullary Nail (CMN): The implant of choice for unstable patterns, particularly reverse obliquity (AO 31-A3) and fractures with subtrochanteric extension. The intramedullary position of the nail decreases the lever arm of the implant, reducing bending moments and the risk of hardware failure.
Biomechanical Pearl: In reverse obliquity fractures, an SHS is contraindicated. The sliding mechanism of the SHS allows the femoral shaft to medialize uncontrollably due to adductor pull, leading to catastrophic failure. A cephalomedullary nail acts as a lateral buttress, preventing this medialization.
Step-by-Step Surgical Technique
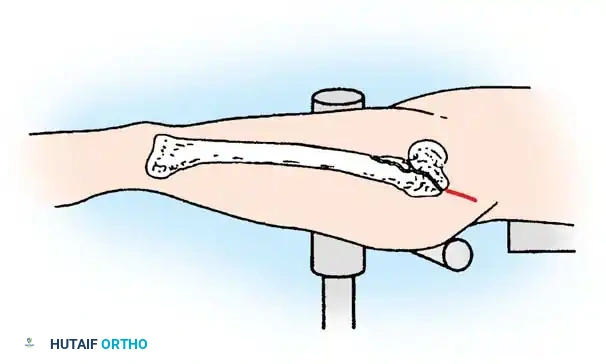
1. Patient Positioning and Reduction
The patient is placed supine on a radiolucent fracture table. The operative leg is secured in a traction boot, and the well leg is placed in a hemilithotomy position or scissored posteriorly to allow unobstructed access for the C-arm fluoroscope.

Proper patient positioning on the fracture table is paramount. Ensure the C-arm can freely rotate from AP to lateral without obstruction.
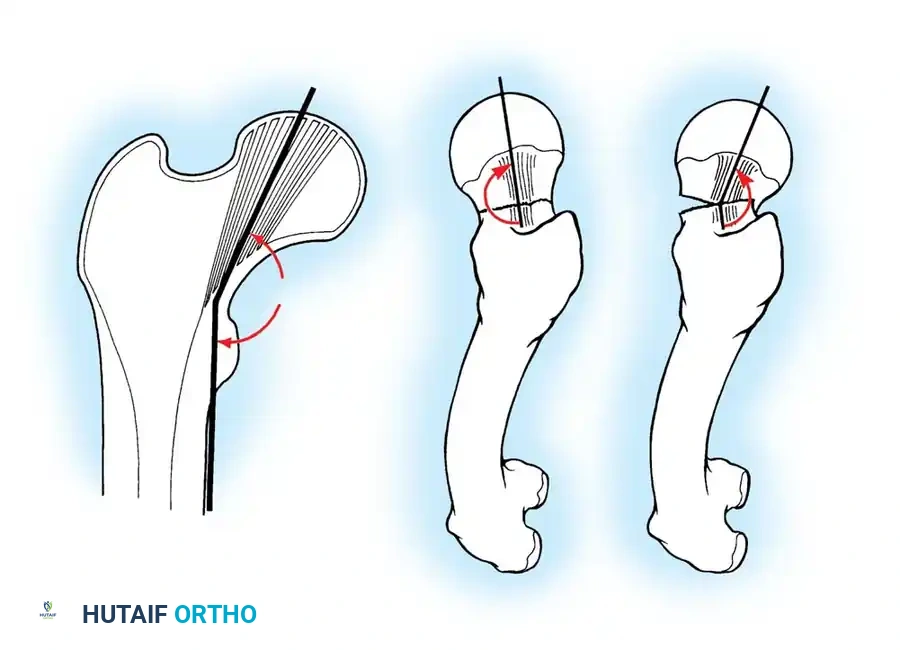
Closed Reduction Maneuver:
1. Apply longitudinal traction to restore leg length.
2. Internally rotate the leg (typically 10 to 15 degrees) to correct the external rotation deformity and bring the femoral neck parallel to the floor.
3. Verify reduction on both AP and lateral fluoroscopic views. An acceptable reduction must have cortical apposition medially and anteriorly.
2. Surgical Approach (Lateral)
A longitudinal incision is made over the lateral aspect of the proximal femur, starting at the tip of the greater trochanter and extending distally. The fascia lata is incised, and the vastus lateralis is elevated or split to expose the lateral femoral cortex.
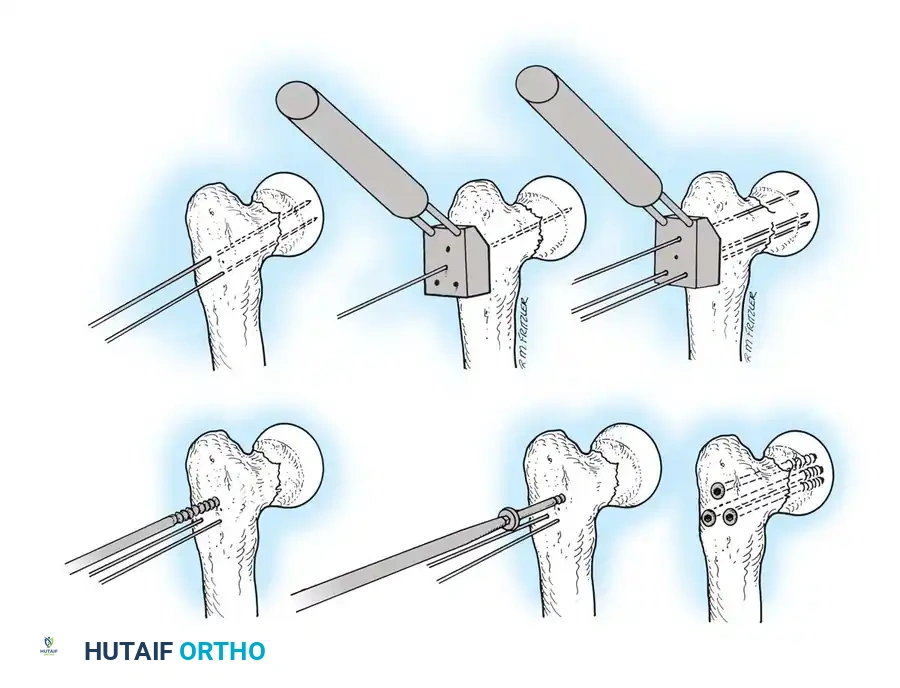
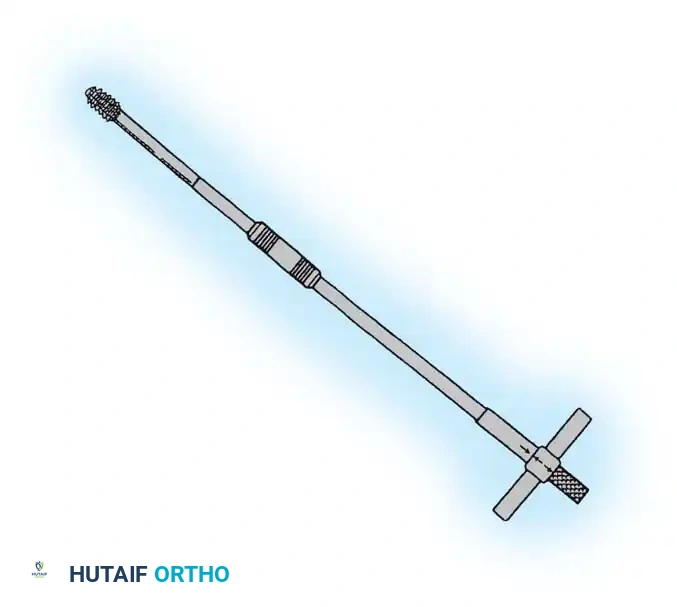
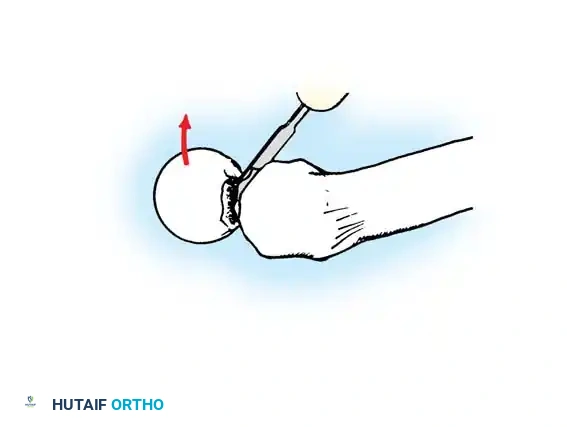
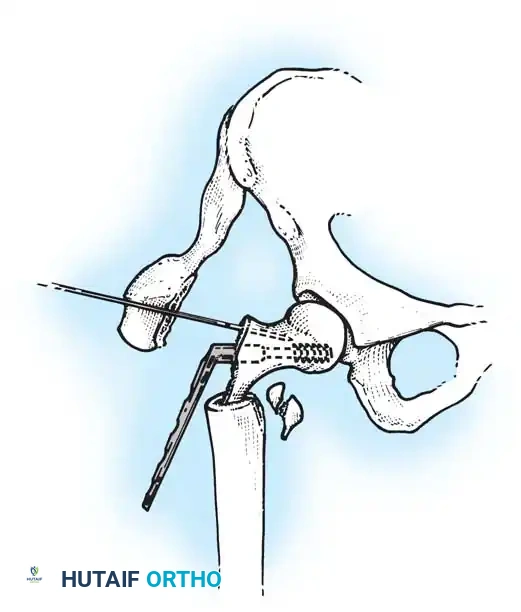
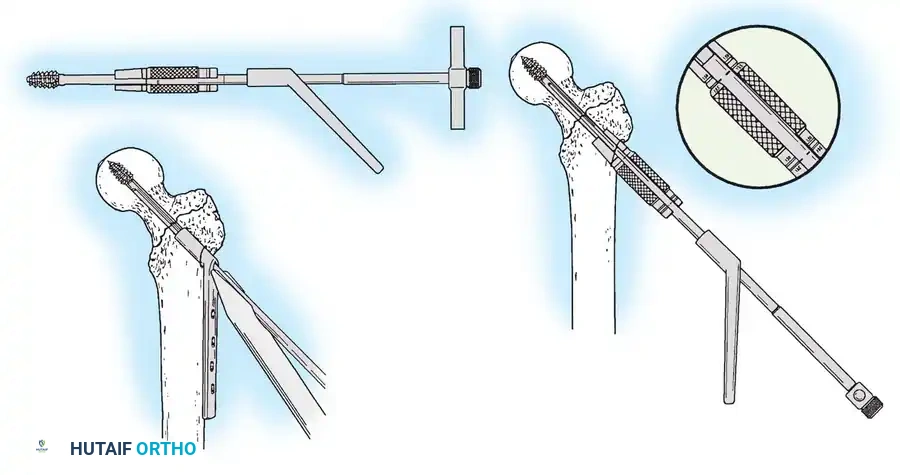
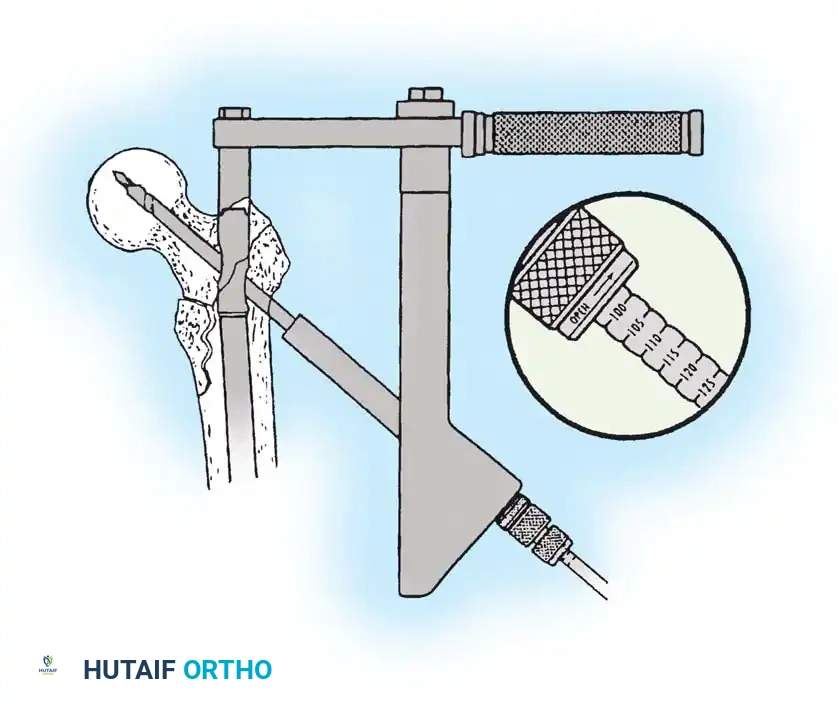
3. Guide Wire Placement
Whether using an SHS or a CMN, accurate placement of the guide wire into the femoral head is the most critical step of the operation.
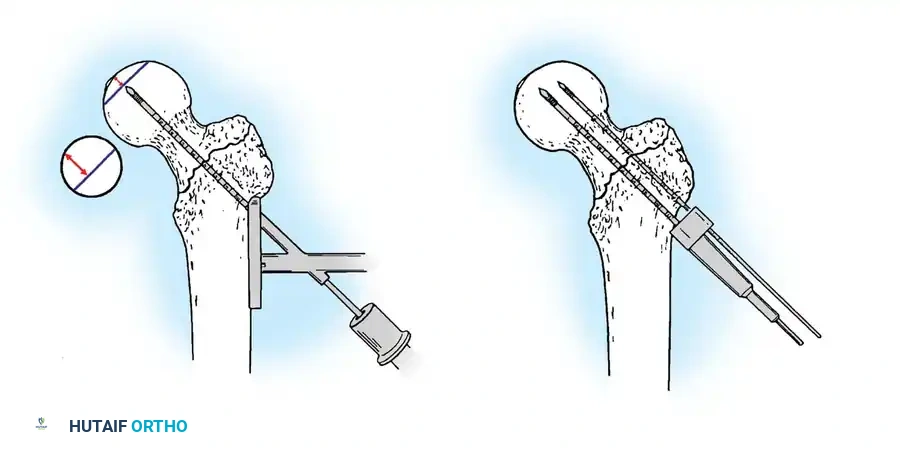
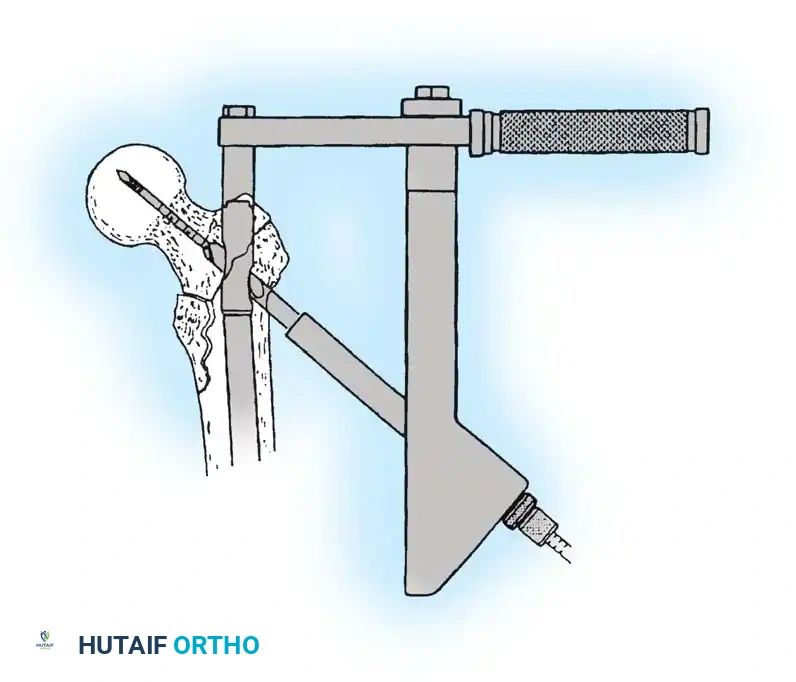
Insertion of the guide wire. The wire must be positioned centrally in the femoral head on both AP and lateral views.
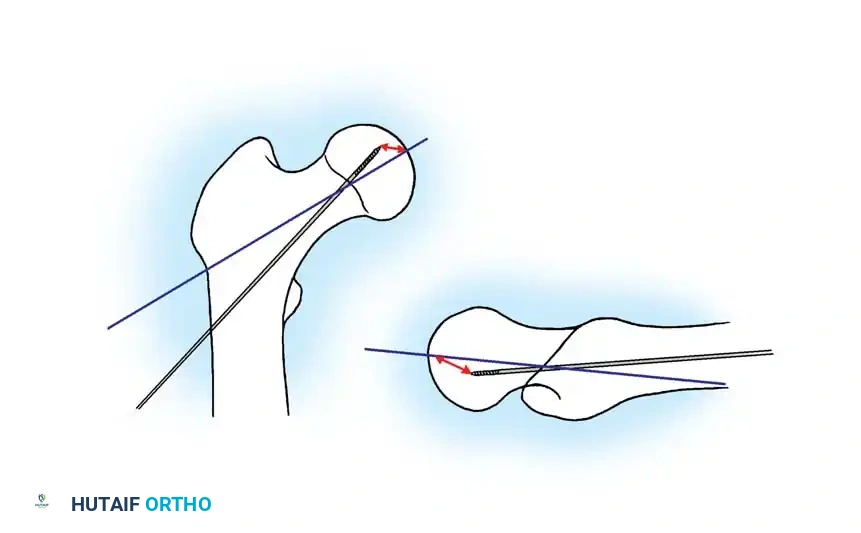
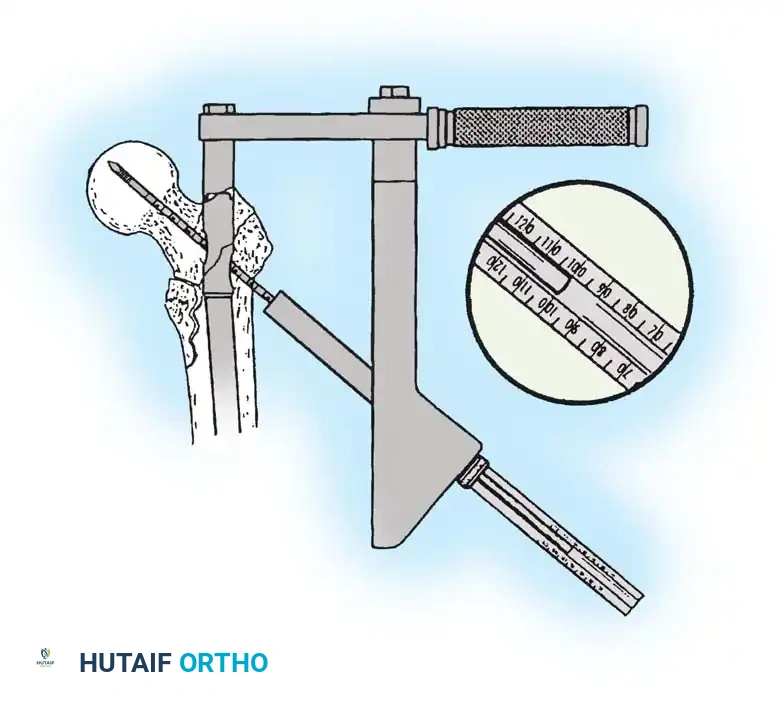
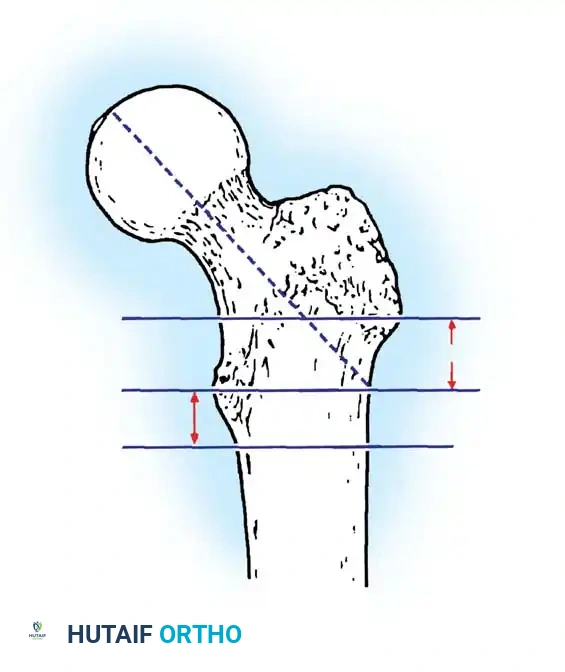
The Tip-Apex Distance (TAD):
Described by Baumgaertner, the TAD is the sum of the distance from the tip of the lag screw to the apex of the femoral head on both the AP and lateral radiographs. A TAD of less than 25 mm is strongly predictive of successful fixation; a TAD > 25 mm significantly increases the risk of screw cut-out.
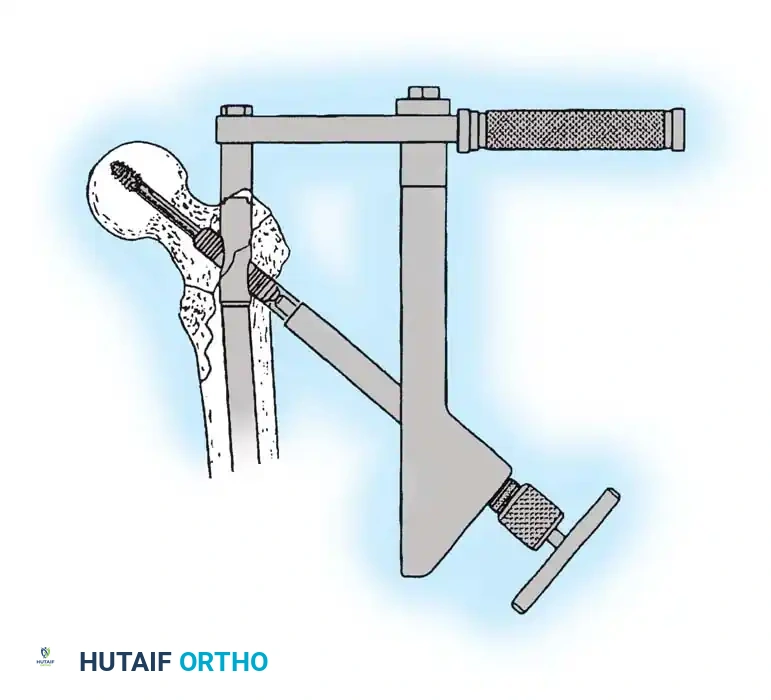
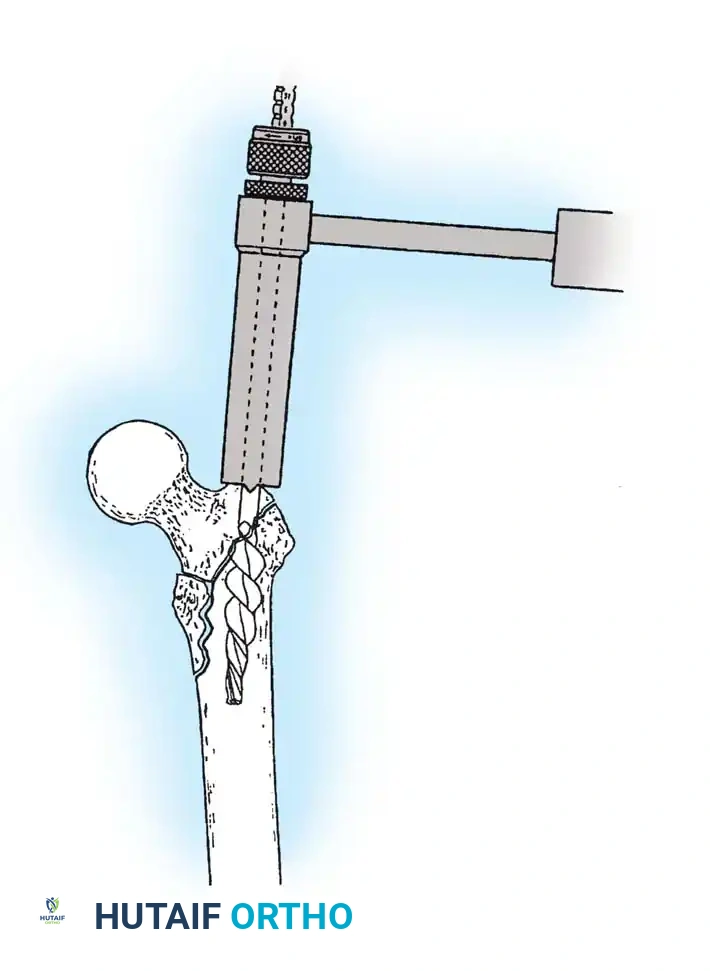
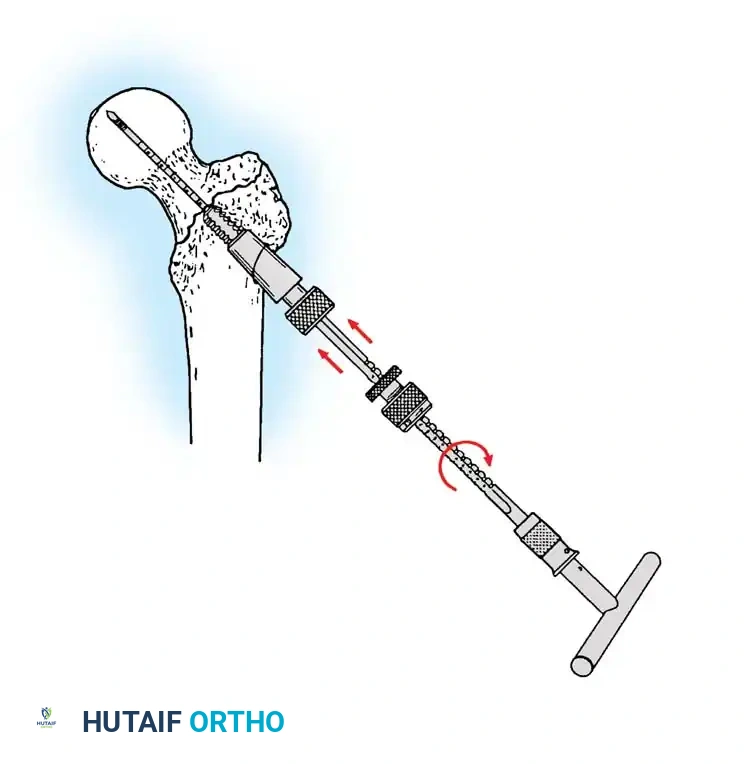
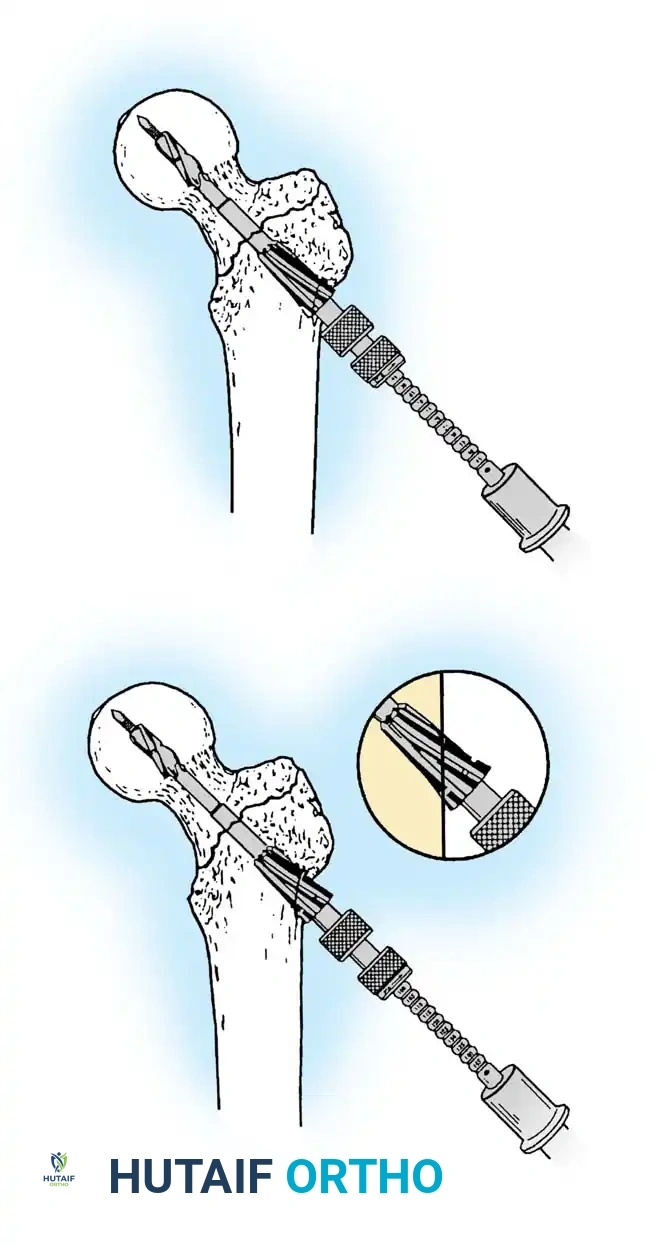
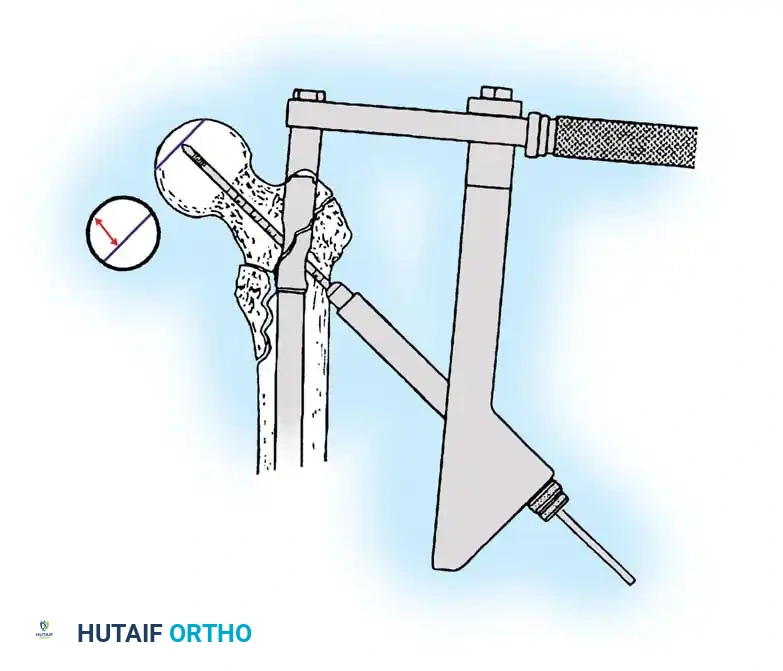
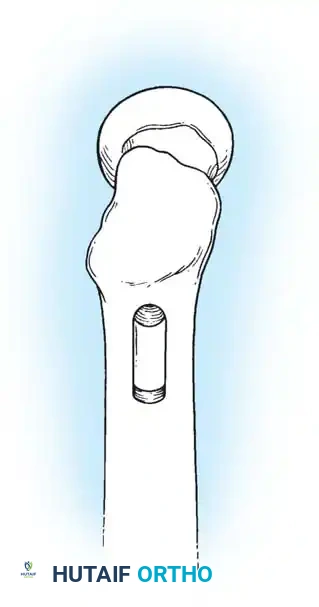
4. Reaming and Lag Screw Insertion
Once the guide wire is perfectly positioned, the lateral cortex is opened, and the femoral neck is reamed over the wire.
Reaming of the femoral neck and head over the precisely placed guide wire, preparing the channel for the lag screw.
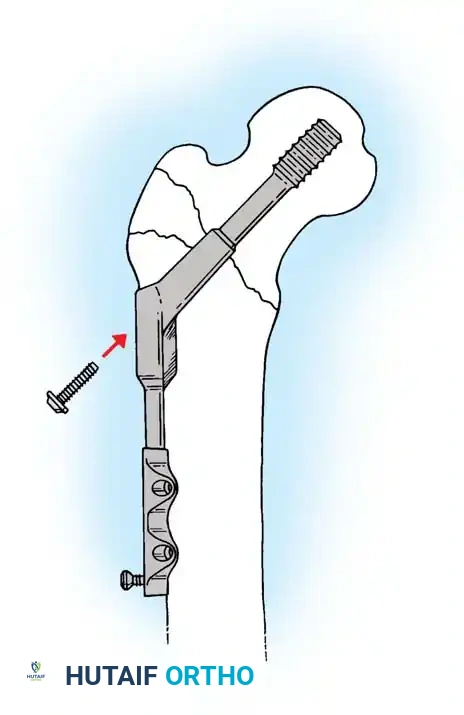
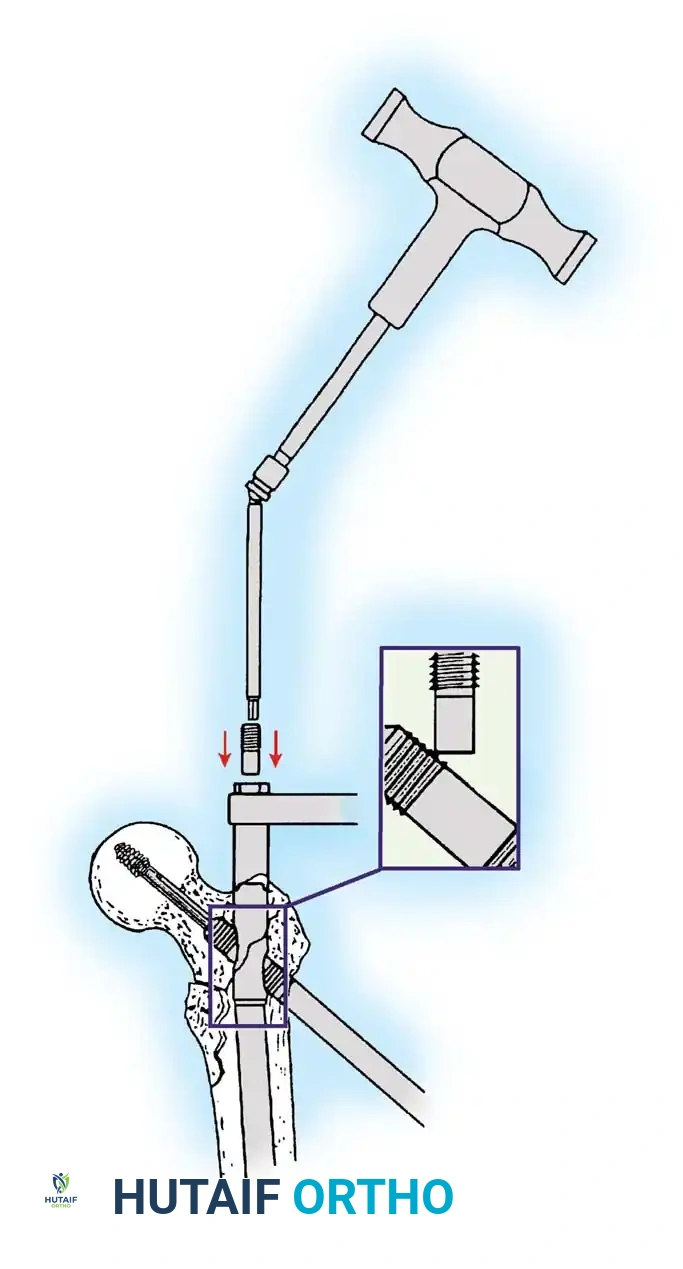
The lag screw is then inserted. It is crucial not to over-insert the screw, which can penetrate the articular cartilage, nor to under-insert it, which compromises fixation.
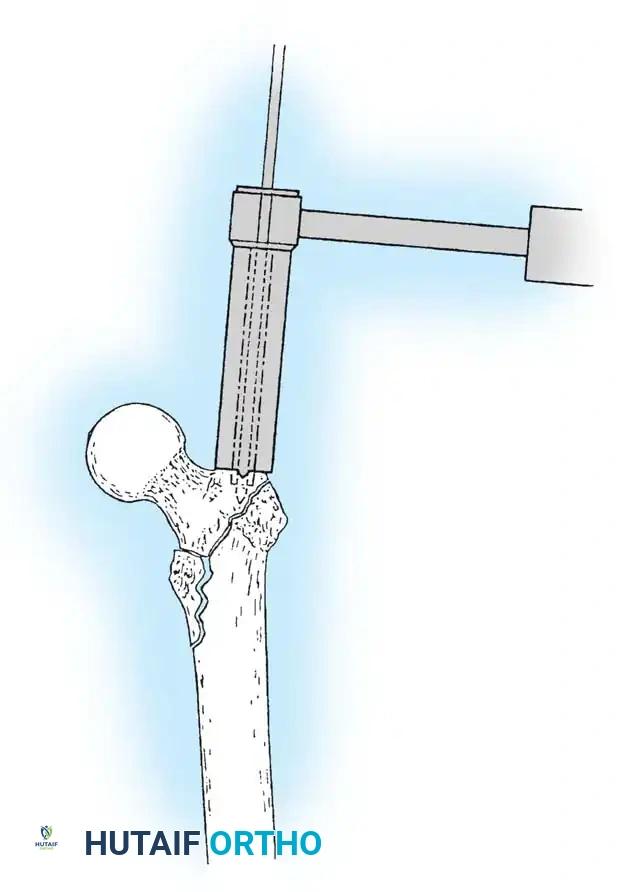
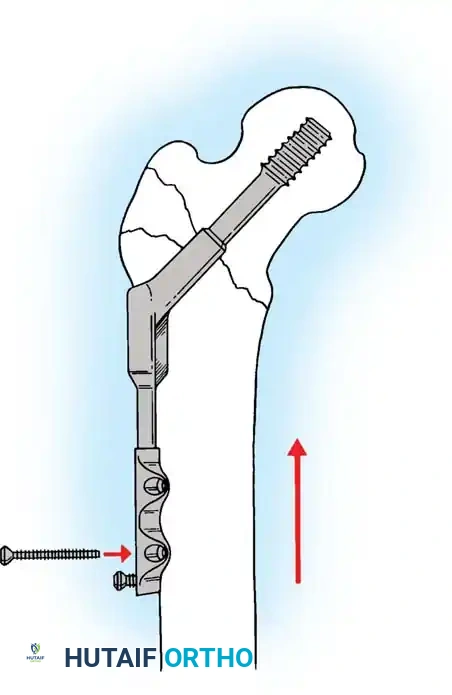
5. Intramedullary Nailing (For Unstable Fractures)
If a cephalomedullary nail is chosen, the entry point is established at the tip of the greater trochanter (or slightly medial, depending on the specific implant design).
Insertion of the cephalomedullary nail down the femoral shaft. Care must be taken not to distract the fracture site during insertion.
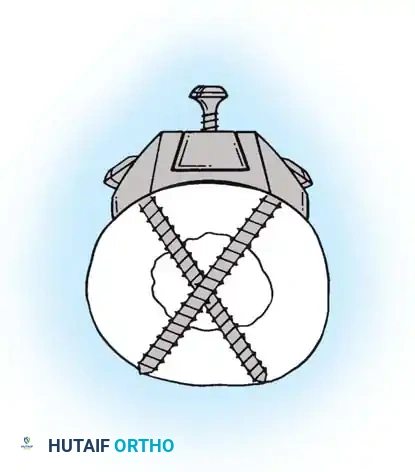
After the nail is seated, the proximal lag screw(s) are inserted through the nail into the femoral head, adhering to the same TAD principles.
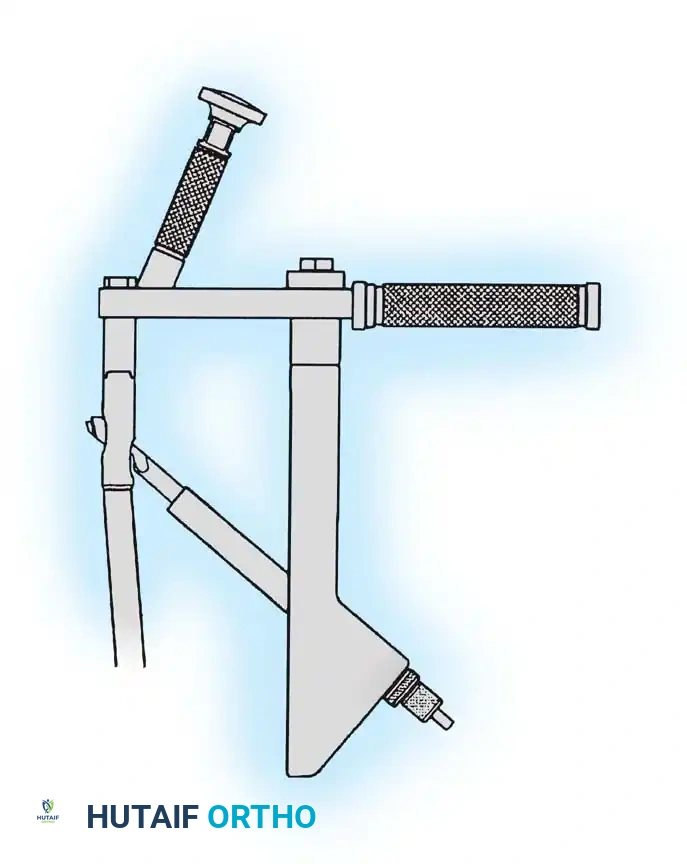
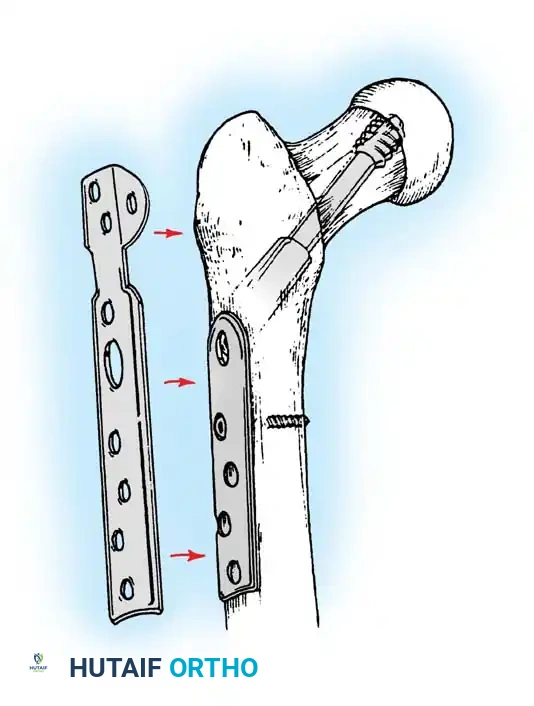
Proximal locking of the cephalomedullary nail. The targeting guide ensures accurate trajectory into the femoral neck.
Finally, distal locking screws are placed to control rotation and maintain length.
Final fluoroscopic evaluation confirming anatomical reduction, optimal implant placement, and restoration of the neck-shaft angle.
Postoperative Protocol and Rehabilitation
The primary objective of operative fixation is to allow immediate mobilization. Prolonged bed rest in the elderly is associated with devastating complications, including deep vein thrombosis (DVT), pulmonary embolism, pneumonia, decubitus ulcers, and rapid physical deconditioning.
- Weight-Bearing: Patients should be allowed weight-bearing as tolerated (WBAT) immediately postoperatively. Studies by Koval et al. demonstrated that patients voluntarily limit their loading based on pain, and early weight-bearing does not increase the rate of hardware failure in well-reduced fractures.
- VTE Prophylaxis: Chemical prophylaxis (e.g., Low Molecular Weight Heparin, Direct Oral Anticoagulants) combined with mechanical prophylaxis is mandatory for a minimum of 28 to 35 days postoperatively.
- Osteoporosis Management: A fragility fracture of the hip is a sentinel event. Postoperative protocols must include a DEXA scan and the initiation of bone-modifying agents (bisphosphonates, denosumab, or teriparatide) to prevent contralateral hip fractures.
Complications and Salvage
Despite meticulous surgical technique, complications can occur, particularly in osteoporotic bone.
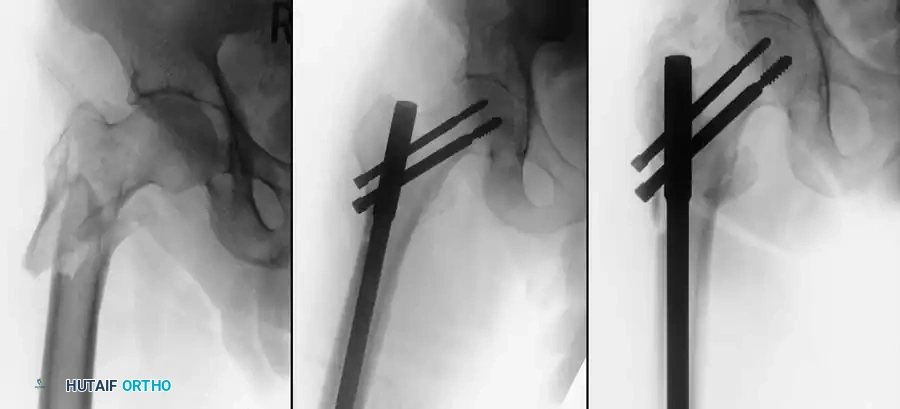
1. Hardware Cut-Out
The most common mechanical failure is the "cut-out" of the lag screw through the superior aspect of the femoral head. This is almost exclusively the result of a poor initial reduction (varus malalignment) or an excessive Tip-Apex Distance (>25 mm).

Example of hardware failure and varus collapse. Note the superior migration of the lag screw, necessitating revision surgery.
2. Nonunion and Malunion
While nonunion is rare in intertrochanteric fractures due to the rich cancellous bone bed, malunion (typically varus collapse and shortening) is more common. Significant malunions alter hip biomechanics, leading to a Trendelenburg gait and early abductor fatigue.
3. Infection
Deep surgical site infections occur in 1-2% of cases. Acute infections may be managed with aggressive debridement and implant retention, while chronic infections often require hardware removal, placement of an antibiotic spacer, and eventual conversion to a total hip arthroplasty (THA).
Conclusion
The operative management of hip fractures requires a synthesis of rapid medical optimization, precise biomechanical understanding, and flawless surgical execution. By adhering to strict classification-based implant selection—utilizing sliding hip screws for stable patterns and cephalomedullary nails for unstable configurations—and demanding anatomical reduction with a Tip-Apex Distance of less than 25 mm, orthopedic surgeons can reliably restore function and mitigate the high mortality associated with these severe injuries. Early mobilization remains the cornerstone of postoperative care, ensuring the best possible outcome for this vulnerable patient population.
Associated Surgical & Radiographic Imaging















📚 Medical References
- hip fractures, J Bone Joint Surg 85A:899, 2003.
- Hamadouche M, Kerboull L, Meunier A, et al: Total hip arthroplasty for the treatment of ankylosed hips: a fi ve to twenty-one year follow-up study, J Bone Joint Surg 83A:992, 2001.
- Harris WH: Allografting in total hip arthroplasty: in adults with severe acetabular defi ciency including a surgical technique for bolting the graft to the ilium, Clin Orthop Relat Res 162:150, 1982.
- Harris WH, Crothers O, Oh I: Total hip replacement and femoral-head bone-grafting for severe acetabular defi ciency in adults, J Bone Joint Surg 59A:752, 1977.
- Hartley WT, McAuley JP, Culpepper WJ, et al: Osteonecrosis of the femoral head treated with cementless total hip arthroplasty, J Bone Joint Surg 82A:1408, 2000.
- Hozack WJ, Rushton SA, Carey C, et al: Uncemented total hip arthroplasty in Paget’s disease of the hip, J Arthroplasty 14:872, 1999.
- Hungerford DS: Bone marrow pressure, venography, and core decompression in ischemic necrosis of the femoral head. In The hip, St Louis, 1979, Mosby. Inao S, Matsuno T: Cemented total hip arthroplasty with autogenous acetabular bone grafting for hips with developmental dysplasia in adults: the results at a minimum of ten years, J Bone Joint Surg 82B:375, 2000.
- Jana AK, Engh CA, Lewandowski PJ, et al: Total hip arthroplasty using porous coated femoral components in patients with rheumatoid arthritis, J Bone Joint Surg 83B:686, 2001.
- Katz RL, Bourne RB, Rorabeck CH, et al: Total hip arthroplasty in patients with avascular necrosis of the hip, Clin Orthop Relat Res 281:145, 1992.
- Keisu KS, Orozco F, McCallum JD, et al: Cementless femoral fi xation in the rheumatoid patient undergoing total hip arthroplasty: minimum 5-year results, J Arthroplasty 16:415, 2001.
- Kelley SS, Lachiewicz PF, Gilbert MS, et al: Hip arthroplasty in
