FRACTURES AND DISLOCATIONS OF THE CARPAL BONES
The diagnosis of fractures and dislocations of the carpal bones remains one of the most challenging aspects of hand and wrist trauma. The inherent difficulty arises from the complex, overlapping osseous anatomy; the outlines of the eight carpal bones are superimposed in standard radiographic views. Even in a true anteroposterior (AP) projection, at least one bone overlies another, obscuring subtle cortical disruptions.
All radiographic views must be interpreted with a profound understanding of normal osseous contours, intercarpal relationships, and the dynamic kinematic changes that occur during the various arcs of wrist motion. Because of the difficulty in recognizing nondisplaced fractures in acute injuries, significant pathology in this region may be missed at the initial clinical examination. Articular cartilage damage and intrinsic ligamentous injuries (e.g., scapholunate or lunotriquetral tears) are even more difficult to evaluate acutely. These ligamentous disruptions permit abnormal rotations and subluxations of the carpal bones, leading to predictable patterns of carpal instability (e.g., DISI or VISI).
Special radiographic techniques and advanced imaging modalities are indispensable. Nakamura et al. demonstrated that scaphoid fracture displacement is more readily detected and quantified with three-dimensional computed tomography (3D-CT) than with plain tomography. Despite these advanced techniques, establishing a precise diagnosis can be elusive. Furthermore, the prognosis is often guarded due to the precarious peculiarities of the blood supply to these bones, most notably the scaphoid and the lunate. Perlik and Guilford compared magnetic resonance imaging (MRI) with plain radiographs, tomograms, and the surgeon’s intraoperative impression in the assessment of scaphoid nonunions. They concluded that MRI is significantly more accurate than other modalities in predicting the vascularity of the proximal pole in scaphoid nonunions.
FRACTURES OF THE SCAPHOID
Fracture of the carpal scaphoid is the most common fracture of the carpus, accounting for up to 70% of all carpal bone fractures. Unfortunately, the diagnosis is frequently delayed. A delay in the diagnosis and treatment of a scaphoid fracture significantly alters the prognosis for osseous union and increases the risk of avascular necrosis (AVN) and subsequent scaphoid nonunion advanced collapse (SNAC).
Clinical Pearl: A wrist sprain that is sufficiently severe to require radiographic examination initially should be treated as a possible occult fracture of the scaphoid. Radiographs should be repeated in 10 to 14 days, even if the initial films are entirely negative, or advanced imaging (MRI/CT) should be obtained immediately.
Etiology and Biomechanics
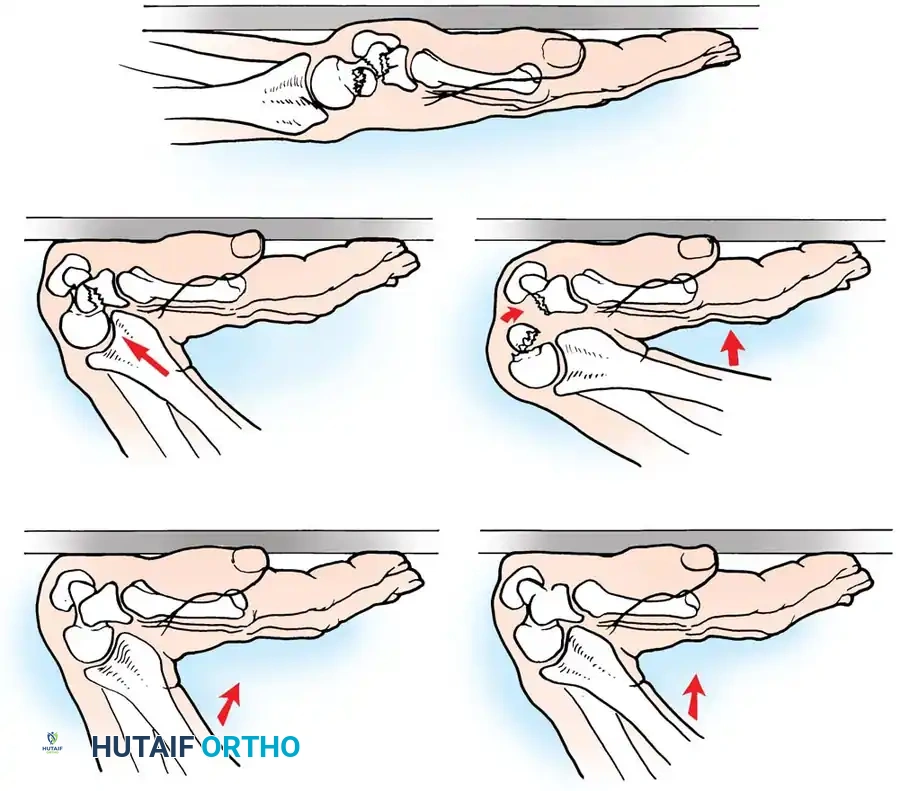
Scaphoid fractures have been reported in individuals ranging from 10 to 70 years of age, though they are overwhelmingly most common in young, active males. The classic mechanism of injury is a fall on the outstretched hand (FOOSH), resulting in severe hyperextension and slight radial deviation of the wrist.
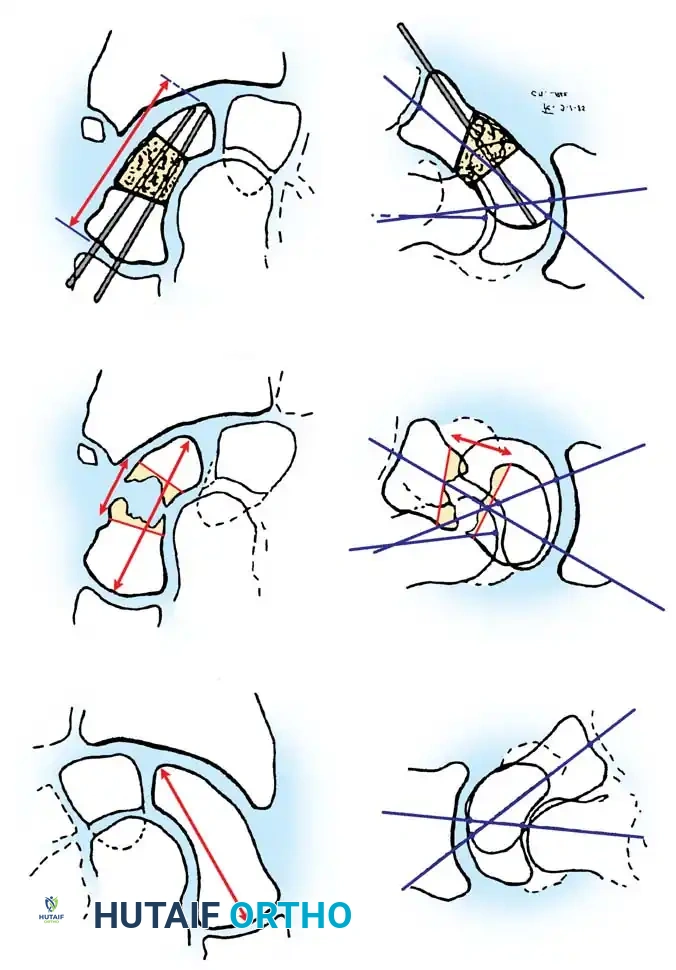
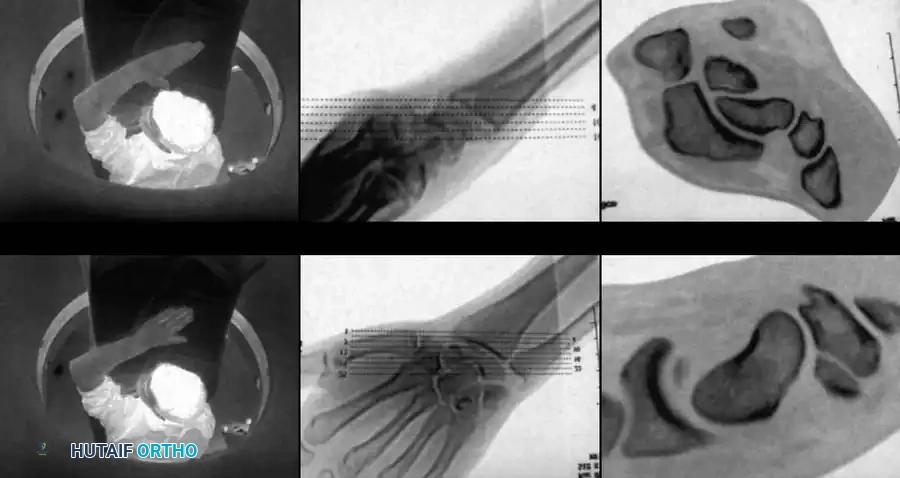
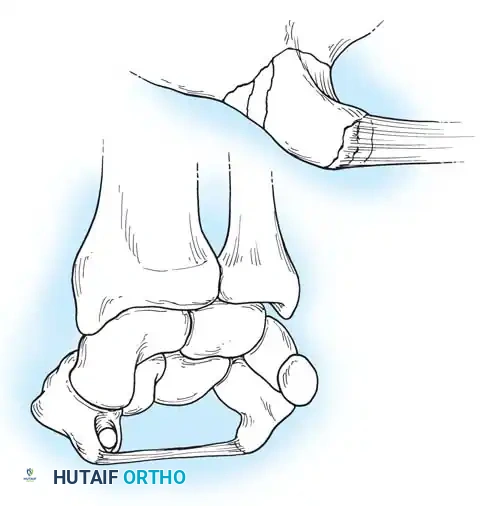
Weber and Chao conducted seminal biomechanical studies demonstrating that the scaphoid typically fractures in tension when the wrist is extended, concentrating the load on the radial-palmar aspect of the bone. During this hyperextension injury, the proximal pole locks securely within the scaphoid fossa of the distal radius, while the distal pole is forced into excessive dorsal translation.
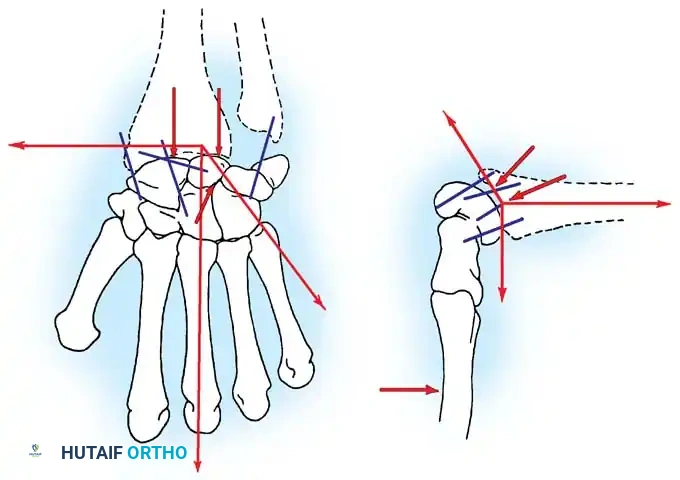
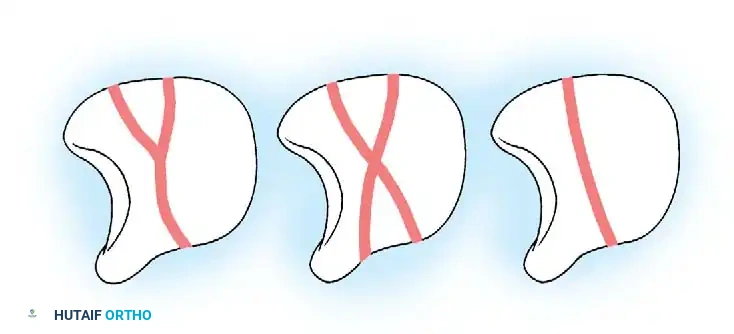
Fig. 66-19: Representation of potential load-carrying structures involved in proximal carpal articulation. Tensile loads are transmitted when the wrist is in strong dorsiflexion. (From Weber ER, Chao EY: An experimental approach to the mechanism of scaphoid waist fractures, J Hand Surg 3A:142, 1978.)
Epidemiologically, 60% to 80% of scaphoid fractures occur at the waist (midportion). Approximately 17% of patients present with concomitant fractures of the carpus and forearm, including transscaphoid perilunar dislocations, fractures of the trapezium, Bennett fractures, radial head fractures, lunate dislocations, and distal radius fractures. When associated carpal injuries require open reduction, the fractured scaphoid must also be anatomically reduced and rigidly fixed.
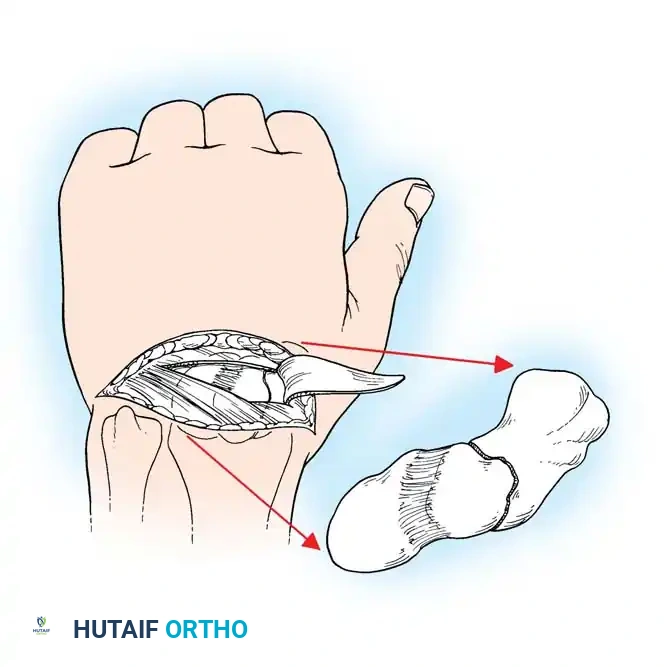
Surgical Anatomy and Blood Supply
The unique anatomy of the scaphoid predisposes it to delayed union, nonunion, and profound wrist disability. As the critical link between the proximal and distal carpal rows, it articulates with the distal radius and four of the remaining seven carpal bones (capitate, trapezium, trapezoid, and lunate). Consequently, the scaphoid participates in nearly all carpal motions, particularly volar flexion. Any alteration of its articular surface through fracture or subluxation, or any loss of stability via ligamentous rupture, induces severe secondary degenerative changes throughout the entire carpus.
The blood supply of the scaphoid is notoriously precarious. Obletz and Halbstein demonstrated that only 67% of scaphoid bones possess arterial foramina throughout their entire length (distal, middle, and proximal thirds). Of the remaining bones, 13% have a blood supply predominantly in the distal third, and 20% have most arterial foramina localized to the waist area, with no more than a single foramen near the proximal third. Consequently, one-third of scaphoid fractures occurring in the proximal pole may be entirely devoid of an adequate blood supply.
Clinically, this vascular anatomy dictates outcomes: the prevalence of osteonecrosis can reach 35% in proximal third fractures. Proximal pole fractures inherently take longer to heal and exhibit significantly higher rates of nonunion.
Taleisnik and Kelly mapped the extraosseous vascularity, showing that vessels enter the scaphoid from the radial artery via laterovolar, dorsal, and distal branches. The laterovolar and dorsal systems share the blood supply to the proximal two-thirds of the scaphoid. Gelberman and Menon further refined this, finding that the vascularity of the proximal pole and 70% to 80% of the intraosseous circulation are provided by branches of the radial artery entering through the dorsal ridge. The distal tuberosity region (20% to 30% of the bone) receives its independent blood supply from volar branches of the radial artery. This retrograde intraosseous blood flow is the fundamental reason why proximal pole fractures are at such high risk for ischemia.

Clinical Evaluation and Advanced Imaging
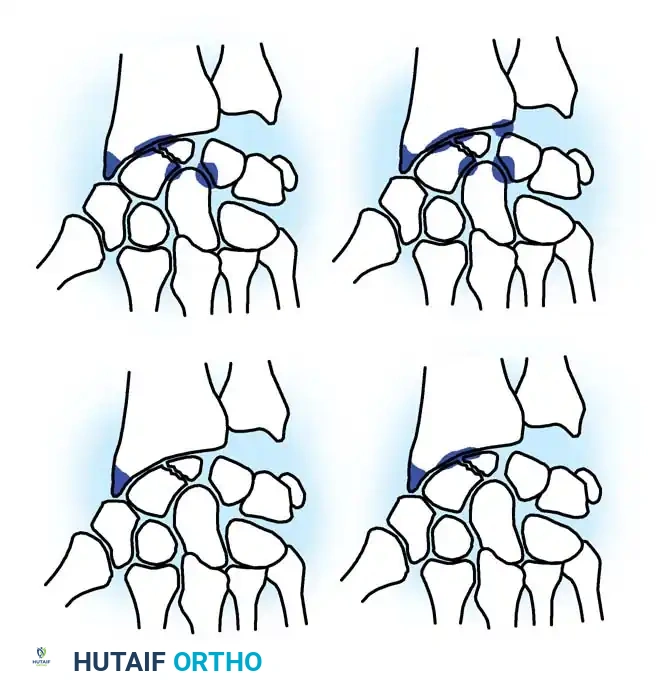
Treatment of scaphoid fractures is dictated by the anatomic location, degree of displacement, and inherent stability of the fracture. Cooney, Dobyns, and Linscheid classified scaphoid fractures broadly into undisplaced/stable and displaced/unstable categories.
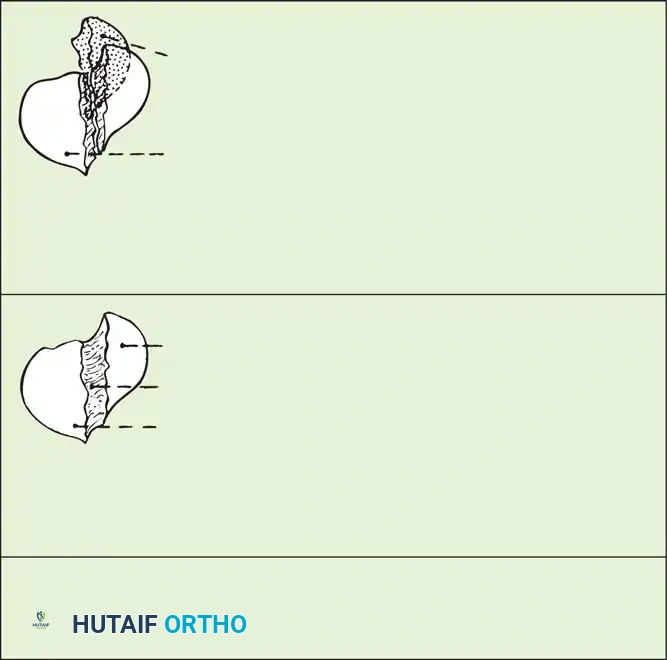
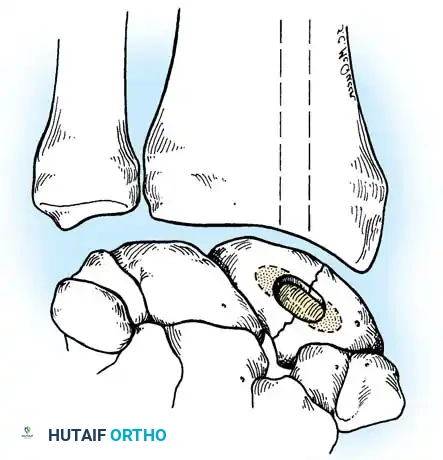
Fig. 66-20: Union of the scaphoid after bone grafting is influenced significantly by the location of the fracture and the amount of displacement. (From Cooney WP, Dobyns JH, Linscheid RL: Nonunion of the scaphoid: analysis of the results from bone grafting, J Hand Surg 5A:343, 1980.)
For nondisplaced fractures, initial radiographic diagnosis can be exceptionally difficult. A posteroanterior (PA) plain radiograph with the wrist slightly extended and in ulnar deviation (the "scaphoid view") elongates the scaphoid profile and is highly recommended.
While repeating radiographs after 2 weeks of cast immobilization is a time-honored protocol for suspected occult fractures, modern practice favors immediate advanced imaging to prevent unnecessary immobilization and expedite definitive care. Technetium bone scans, MRI, and CT (reformatted in the sagittal and coronal planes of the scaphoid) provide rapid diagnostic clarity.

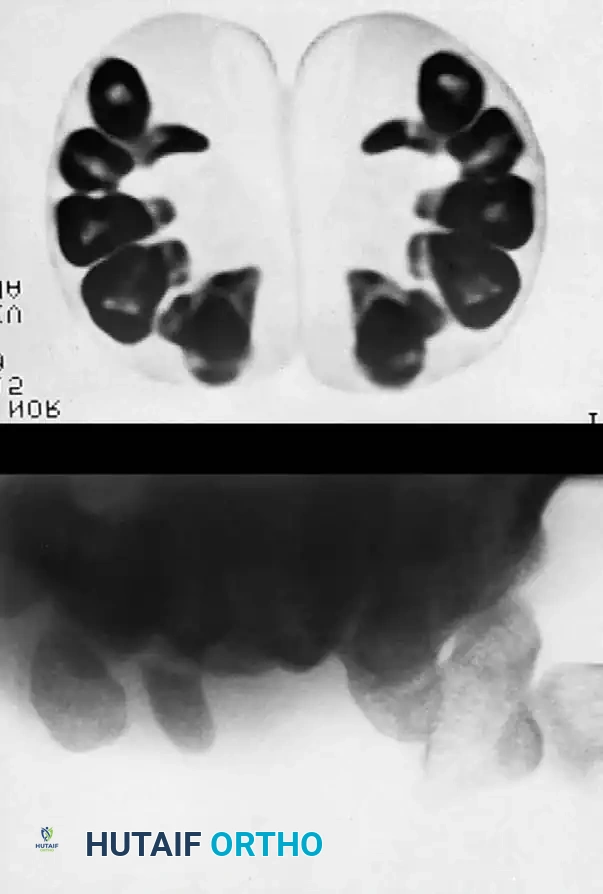
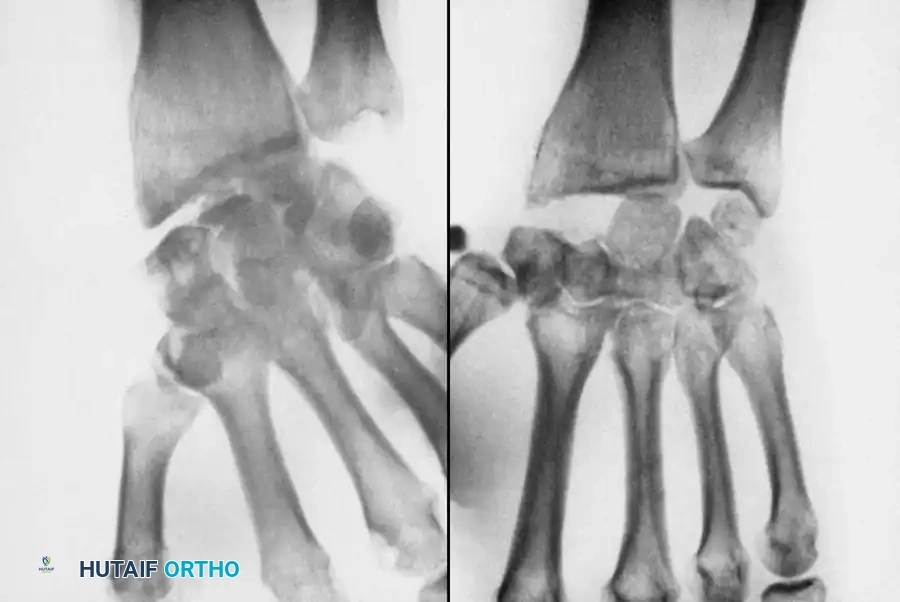
Fig. 66-21: MRI is highly sensitive for the diagnosis of “occult” scaphoid fractures (A) and for the evaluation of the vascularity of the fractured scaphoid (B). (From Segalman KA, Graham TJ: Scaphoid proximal pole fractures and nonunions, J Am Soc Surg Hand 4:233, 2004.)
Gaebler et al. reported 100% sensitivity and specificity using MRI to diagnose occult scaphoid fractures at an average of 2.8 days post-injury. Furthermore, MRI—especially with gadolinium enhancement—is the gold standard for assessing the vascularity of the proximal pole.
Management of Nondisplaced, Stable Scaphoid Fractures
Nonoperative treatment is traditionally successful for acute, nondisplaced, stable fractures through the scaphoid waist and distal pole, provided there is no associated carpal instability. The prognosis is highly favorable if the fracture is diagnosed and immobilized early.
Controversies persist regarding the optimal position of the wrist, the inclusion of the elbow (short vs. long arm cast), and the necessity of thumb immobilization. Terkelsen and Jepsen found no significant difference in nonunion rates between patients treated with a removable short-arm thumb spica cast versus a long-arm thumb spica cast. Conversely, Gellman et al. reported that the time to union was accelerated by up to 3 months in patients treated initially for 6 weeks in a long-arm thumb spica cast.
Biomechanically, Kaneshiro et al. demonstrated that displacement of more than 3 mm can occur between fracture fragments during forearm pronation and supination if only a short-arm cast is used. Therefore, many surgeons prefer a Munster-type cast or a long-arm cast initially. The wrist is typically positioned in slight radial deviation and neutral flexion, with the thumb in a functional position.

Using strict nonoperative casting techniques, the expected rate of union is 90% to 95% within 10 to 12 weeks. During this period, serial radiographs are mandatory to monitor for interval displacement or "humpback" collapse. Singh et al. utilized CT scanning at 12 to 18 weeks to evaluate healing, noting that fractures distal to the waist heal significantly faster than proximal pole fractures.
The Shift Toward Early Operative Fixation
If the diagnosis is delayed, or if the fracture involves the proximal third, the prognosis with casting plummets. Mack et al. found that stable middle-third fractures diagnosed 1 to 6 months post-injury required an average of 19 weeks of casting to heal, compared to 10 weeks for acute fractures.
Due to the morbidity of prolonged immobilization (joint stiffness, muscle atrophy, economic impact), there is a strong, well-established trend toward early operative fixation of even nondisplaced fractures, particularly in young laborers and athletes.
Prospective, randomized studies by Bond et al. and Adolfsson et al. comparing percutaneous screw fixation with cast immobilization demonstrated that operatively treated patients regained motion and returned to work/sports significantly earlier, with no detrimental effects on fracture healing. Dias et al. reported zero nonunions in a cohort treated with Herbert screw fixation, compared to 10 nonunions in a matched cast-treated group at 12 weeks.
Techniques such as "limited access" percutaneous and arthroscopically assisted fixation (championed by Slade, Jaskwhich, and Inoue) minimize trauma to the volar radiocarpal ligaments and preserve the tenuous dorsal blood supply.
Management of Displaced, Unstable Scaphoid Fractures
A displaced, unstable scaphoid fracture demands operative intervention. The criteria for instability include:
* Displacement or step-off > 1 mm on any radiographic view.
* Lunocapitate angulation > 15 degrees.
* Scapholunate angulation > 60 degrees (or > 45 degrees depending on the baseline).
* Lateral intrascaphoid angle > 45 degrees.
* Anteroposterior intrascaphoid angle < 35 degrees (Amadio et al.).
* Height-to-length ratio ≥ 0.65 (Bain et al.).
Surgical Warning: Failure to recognize and correct a "humpback" flexion deformity of the scaphoid will result in a malunion, leading to a permanent loss of wrist extension and inevitable dorsal intercalated segment instability (DISI) with subsequent radiocarpal arthrosis.
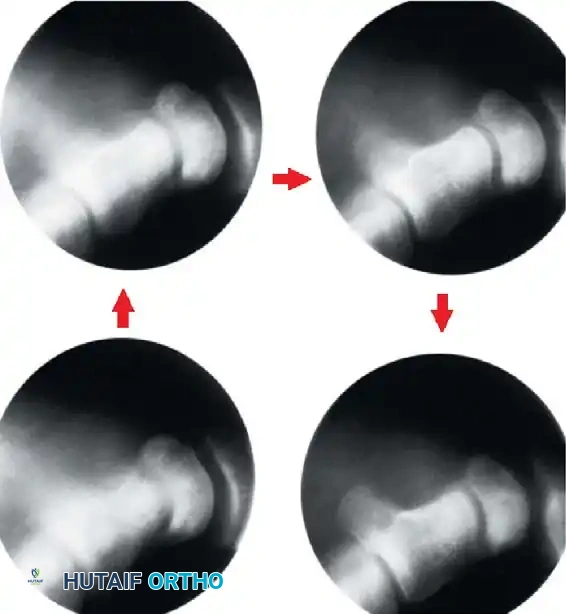
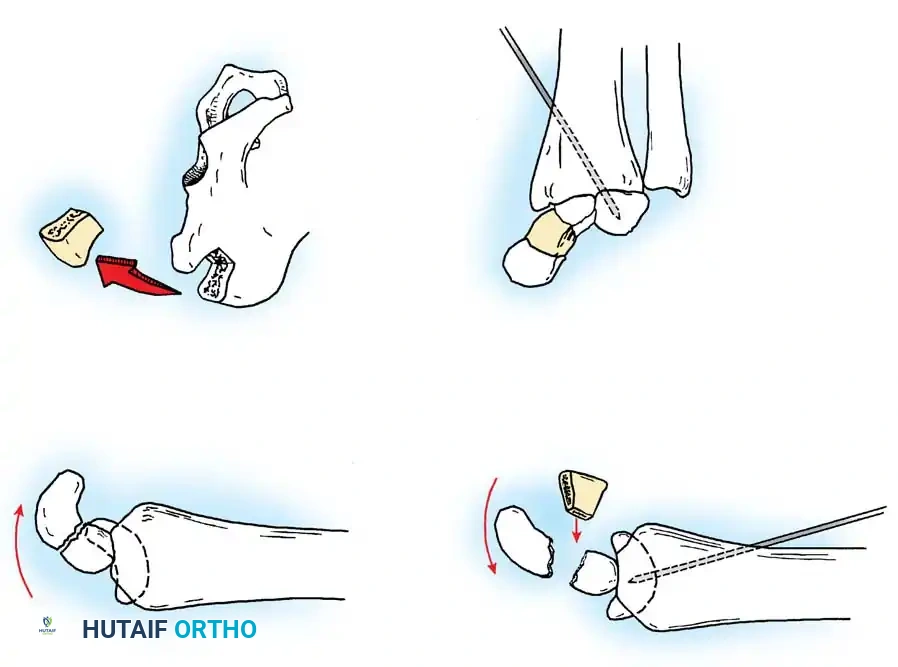
Closed Reduction and Percutaneous Fixation
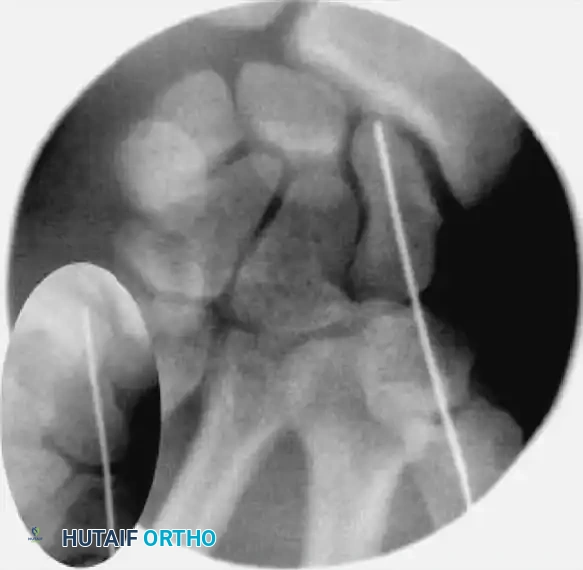
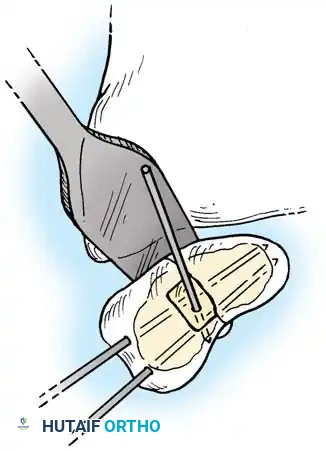
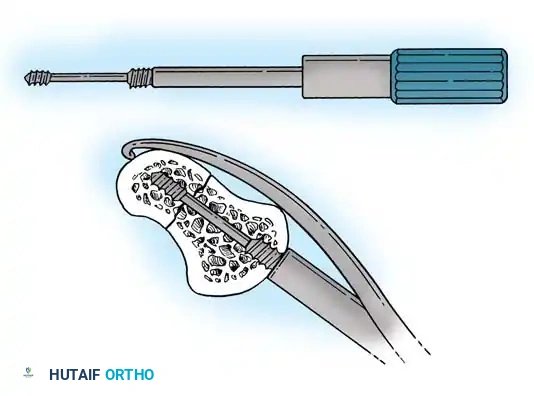
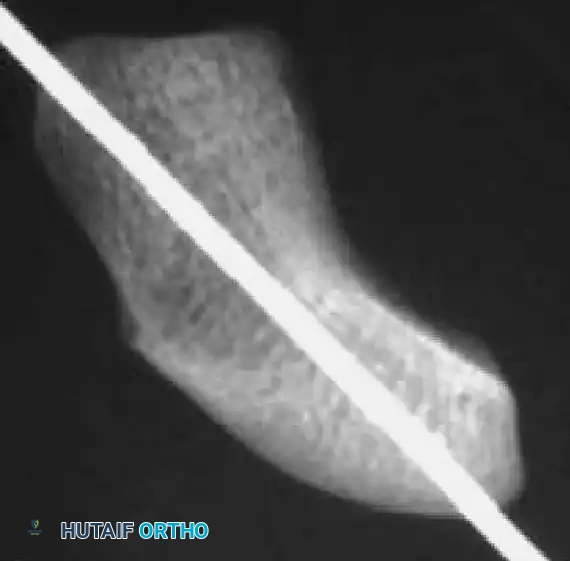
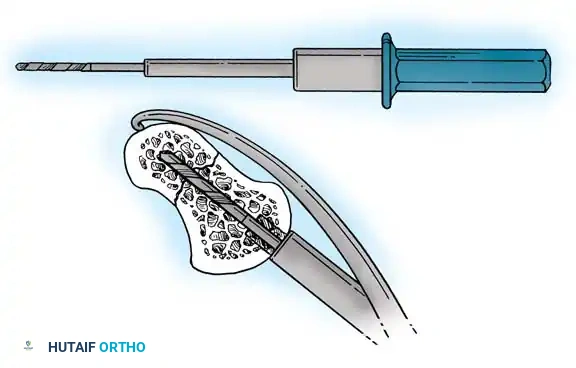
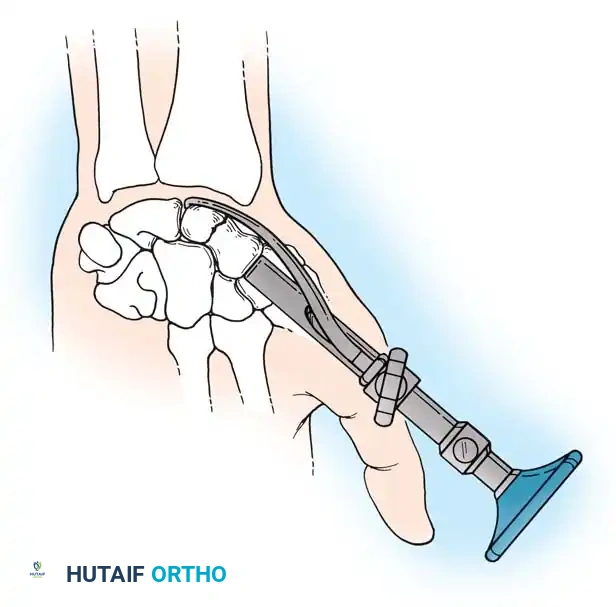
Reduction can initially be attempted via longitudinal traction, ulnar deviation, and direct volar pressure over the scaphoid tuberosity. If anatomic reduction is achieved fluoroscopically, percutaneous fixation with a cannulated headless compression screw (e.g., Acutrak, Herbert) is performed.

The guidewire must be placed down the central axis of the scaphoid. Biomechanical studies confirm that a centrally placed screw provides the maximum biomechanical stiffness and highest load-to-failure, as it captures the densest bone in the proximal pole.
Open Reduction and Internal Fixation (ORIF)
If closed reduction fails, or if there is significant comminution requiring bone grafting, ORIF is indicated. The choice of surgical approach depends on the fracture location:
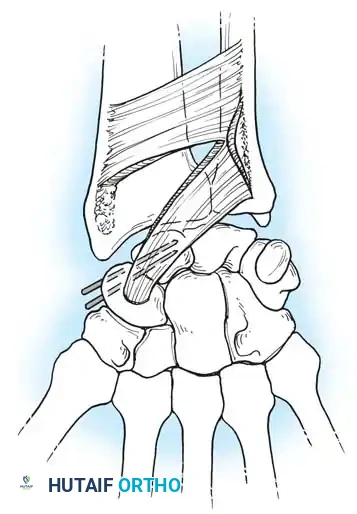
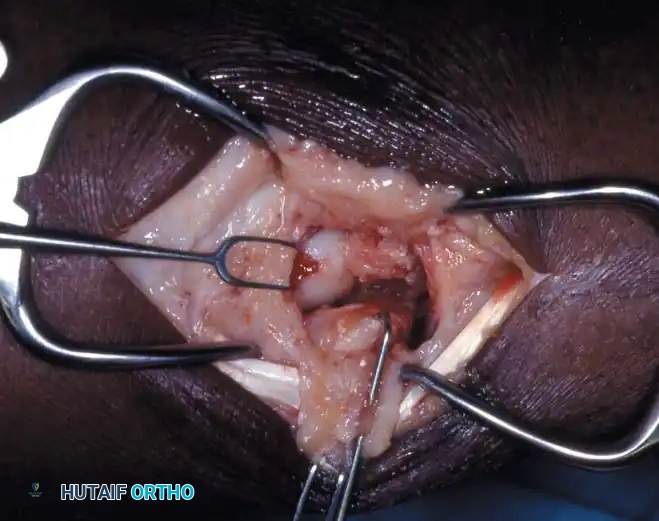
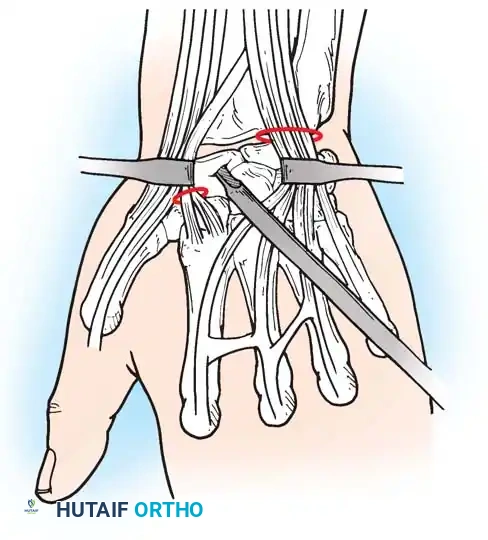
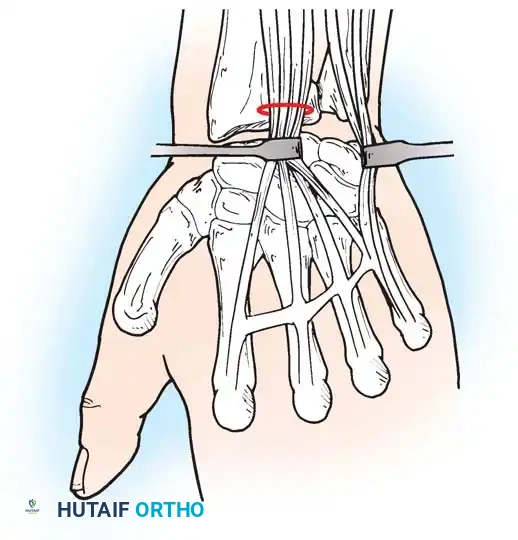
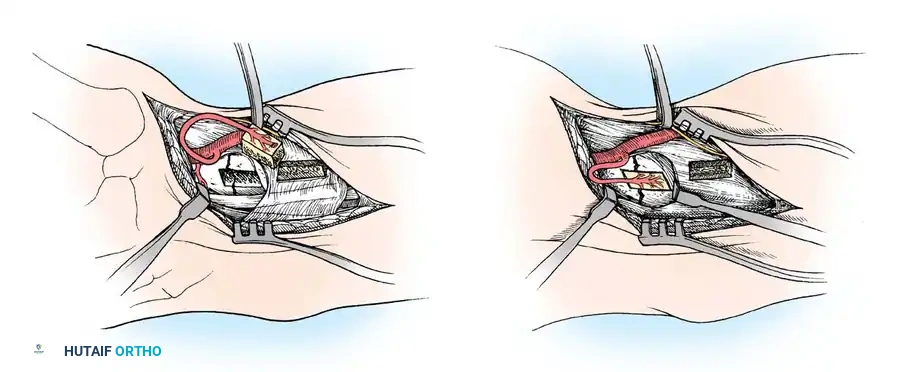
1. Volar Approach (Russe):
Ideal for waist and distal pole fractures.
* An incision is made over the flexor carpi radialis (FCR) tendon.
* The FCR sheath is opened, and the tendon is retracted ulnarly.
* The posterior sheath is incised to expose the volar wrist capsule.
* The capsule is incised longitudinally, carefully preserving the critical volar radioscaphocapitate (RSC) ligament.
* The fracture is debrided, reduced, and provisionally pinned. A headless compression screw is inserted from distal to proximal.

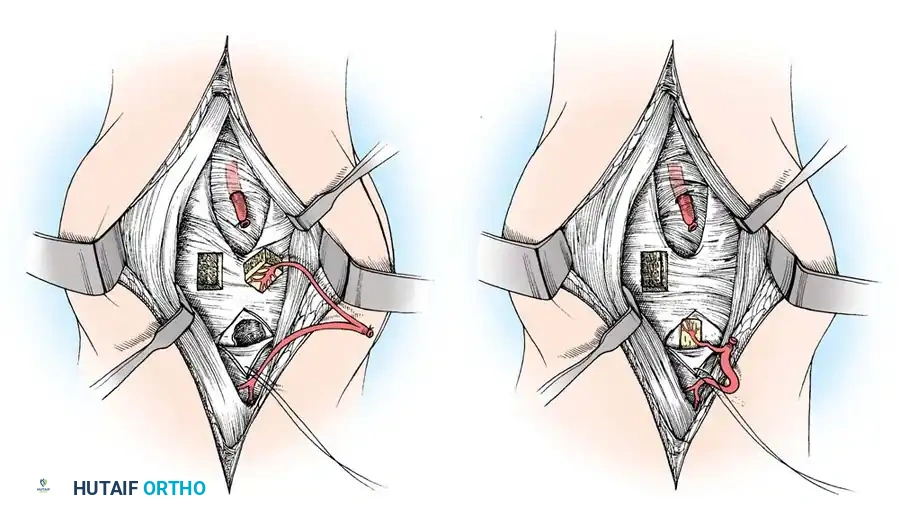
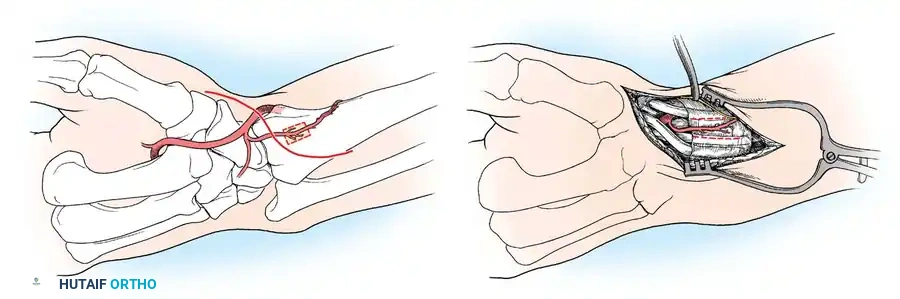
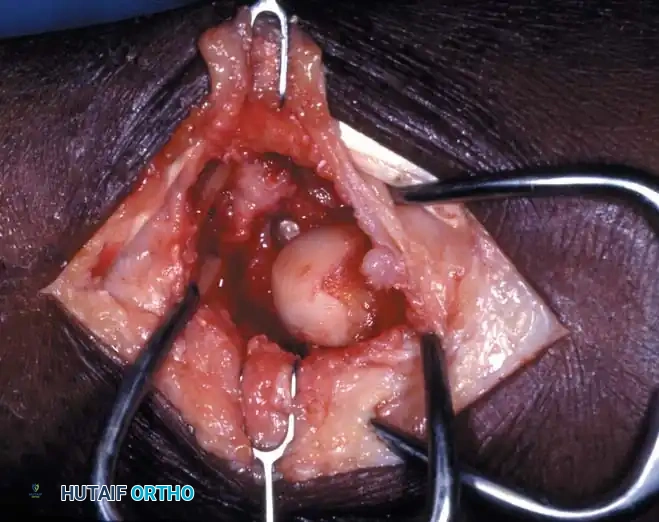
2. Dorsal Approach:
Mandatory for proximal pole fractures to allow direct, antegrade screw insertion perpendicular to the fracture plane.
* A longitudinal incision is made centered over Lister's tubercle.
* The extensor pollicis longus (EPL) is mobilized and retracted radially.
* The dorsal capsule is incised, exposing the proximal scaphoid and scapholunate interval.
* Extreme care is taken not to strip the dorsal ridge, as this houses the primary intraosseous blood supply.
* The screw is inserted from proximal to distal, ensuring the trailing threads are buried beneath the articular cartilage to prevent radiocarpal impingement.
Advanced Fixation Techniques and Bone Grafting
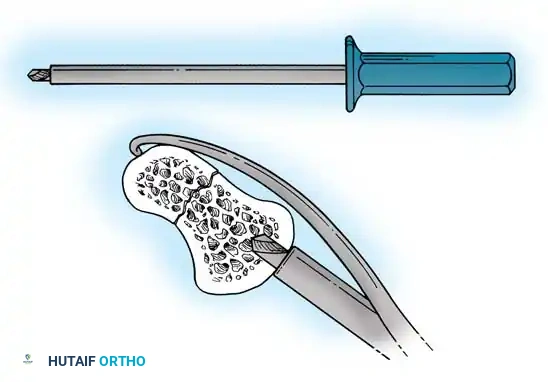
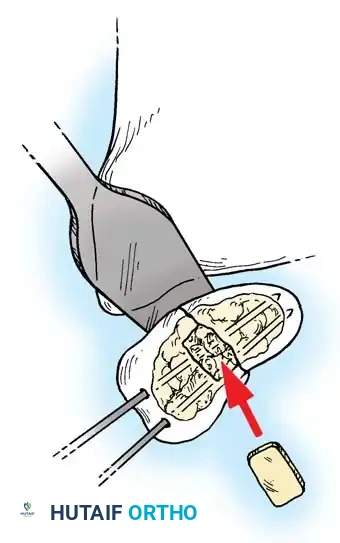
In cases of delayed presentation or established nonunion, simple compression is insufficient. The sclerotic bone ends must be aggressively debrided back to punctate bleeding bone. If a humpback deformity exists, a volar wedge graft (typically harvested from the iliac crest or distal radius) is required to restore scaphoid length and correct the carpal alignment.

For proximal pole nonunions with avascular necrosis, vascularized bone grafts (VBGs) are indicated. The 1,2-Intercompartmental Supraretinacular Artery (1,2-ICSRA) graft, popularized by Zaidemberg, is a reliable pedicled graft harvested from the dorsal distal radius. Alternatively, free vascularized grafts from the medial femoral condyle (MFC) have shown excellent union rates for recalcitrant cases with severe proximal pole ischemia.
Postoperative Protocol
Following rigid internal fixation, the wrist is typically immobilized in a bulky dressing and volar splint for 10 to 14 days to allow soft tissue healing. If fixation is deemed absolutely rigid (e.g., robust screw purchase in good bone stock), early active range of motion may be initiated. However, if bone grafting was performed or fixation is tenuous, a thumb spica cast is maintained for 4 to 6 weeks, followed by a removable splint and progressive therapy.
Serial radiographs are obtained at 2, 6, and 12 weeks. CT scanning is highly recommended at 10 to 12 weeks to definitively confirm osseous bridging before releasing the patient to heavy manual labor or contact sports.
Complications
1. Nonunion: Occurs in 5-10% of treated fractures, but much higher in proximal pole injuries or delayed presentations. Treatment requires ORIF with structural or vascularized bone grafting.
2. Avascular Necrosis (AVN): The proximal pole is highly susceptible. MRI is diagnostic. Treatment ranges from vascularized bone grafting to salvage procedures (e.g., proximal row carpectomy or four-corner fusion) if advanced collapse has occurred.
3. Scaphoid Nonunion Advanced Collapse (SNAC): A predictable pattern of degenerative arthritis beginning at the radioscaphoid joint and progressing to the midcarpal joint.

By adhering to strict diagnostic protocols, utilizing advanced imaging judiciously, and applying rigid biomechanical principles during surgical fixation, the orthopedic surgeon can reliably navigate the complexities of scaphoid fractures and restore optimal wrist kinematics.
(Additional intraoperative and radiographic references for complex carpal reconstructions are provided below for comprehensive review.)